

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Anatomic total shoulder arthroplasty (TSA) has proven to be a reliable procedure for a variety of shoulder pathologies with good long-term results.123456) TSA is most commonly performed for degenerative shoulder conditions such as glenohumeral osteoarthritis (OA). Reverse shoulder arthroplasty (RSA) has been used in Europe since the 1980s and was approved by the Food and Drug Administration in 2004.7) RSA is a treatment option for patients with cuff tear arthropathy (CTA), which has yielded consistent results. The number of TSA and especially RSA procedures performed each year continues to increase.8) The cause of the increase in RSAs performed is multifactorial, but includes increased surgeon's confidence in the procedure, as well as expanding indications such as use in revision shoulder arthroplasty, posterior glenoid bone loss, and fracture sequelae.910)
Given the increase in utilization, prevalence of shoulder OA and rotator cuff disease, increasing life span of patients, and expanding indications, it is common for patients to require staged bilateral shoulder arthroplasties. Historically, one concern of bilateral RSAs has been the impact on the performance of activities of daily living (ADLs), especially maintenance of perineal hygiene. However, recent evidence suggests that patients with bilateral RSAs are able to adequately perform these activities.11121314) Several other studies have reported the results of bilateral TSAs and RSAs independently.1516171819) However, no studies have directly compared the outcomes of patients with bilateral TSAs to bilateral RSAs.
The purpose of this study was to compare the clinical and functional outcomes of patients who underwent bilateral TSAs for OA to patients who underwent bilateral RSAs for CTA. We hypothesized that patients who underwent bilateral TSAs would have better clinical and functional outcomes than patients who underwent bilateral RSAs.
METHODS
Institutional Review Board approval was obtained from Thomas Jefferson University Hospital prior to conducting this retrospective analysis (IRB No. 45 CFR 46.110, Control #17D.020). All data collection was retrospective and all patients provided informed consent preoperatively for retrospective data review. Our institutional billing database was queried using the CPT code 23472 (arthroplasty, glenohumeral joint; total shoulder) to identify all patients who underwent a TSA or RSA from 2004 to 2015. A retrospective chart review was performed to identify all patients who underwent staged bilateral TSAs for OA or staged bilateral RSAs for CTA. Inclusion criteria were patients who underwent bilateral TSAs for OA or bilateral RSAs for CTA with at least 2 years of clinical follow-up from the latest arthroplasty surgery. Exclusion criteria were patients (1) undergoing bilateral TSAs for any diagnosis other than OA, (2) undergoing RSAs for any diagnosis other than CTA, (3) undergoing revision arthroplasty surgery, and (4) having chronic neurologic conditions (cerebrovascular accident, multiple sclerosis, and Parkinson disease). Rotator cuff integrity was assessed intraoperatively for all patients undergoing a TSA procedure. If their rotator cuff was determined to be insuffient, they received an RSA and were thus excluded from the study. For primary OA, all patients had Smilson-Prieto grade 2 or greater changes; for primary CTA, all patients had Hamada grade 2 or greater changes.2021) From 2004 to 2015, 5,261 primary shoulder arthroplasties were performed at our institution. After retrospective chart review, 26 TSA patients (52 shoulders) were matched 2 to 1 with 13 RSA patients (26 shoulders) according to sex, age at first surgery, and time from first arthroplasty surgery.
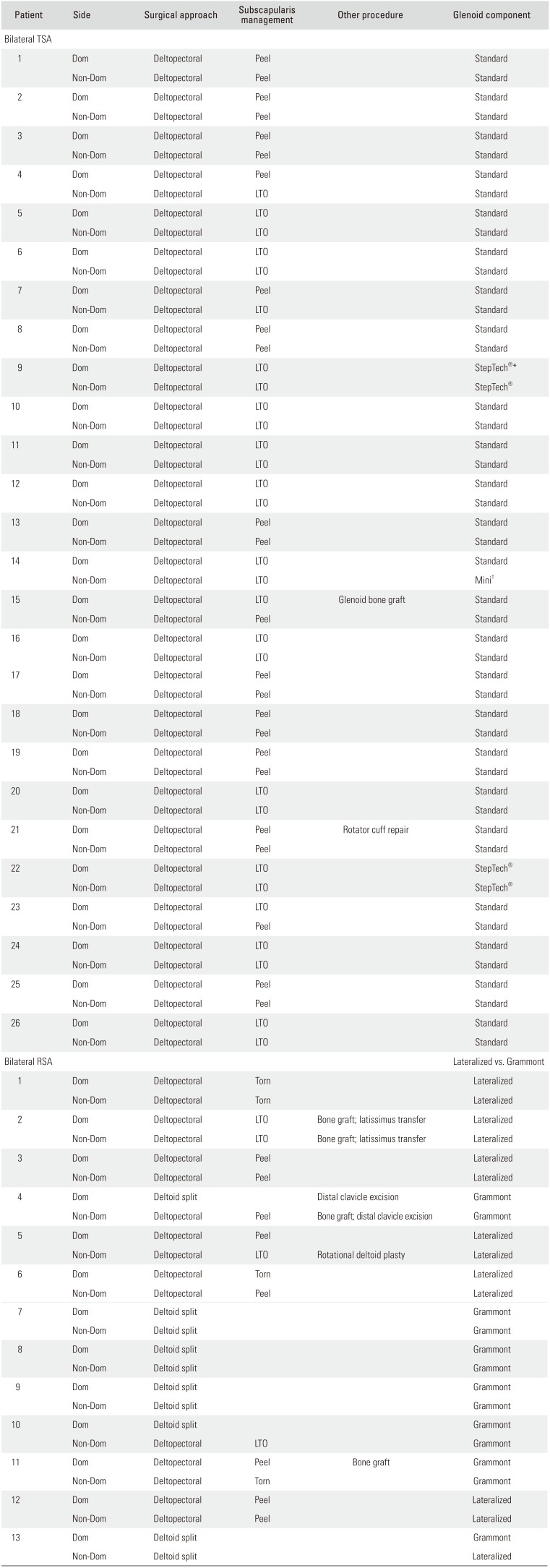
Preoperative and postoperative active ranges of motion (ROMs) in forward elevation (FE), external rotation (ER), and internal rotation (IR) were assessed by chart reviews of clinician-documented ROM. Postoperative complications, readmissions, and reoperations were recorded. Identified patients were then assessed at follow-up visits or contacted via phone for activities of daily living external and internal rotations (ADLEIR; 0–36 point scale of ADL performance) scores, American Shoulder and Elbow Surgeons (ASES) shoulder scores, Single Assessment Numerical Evaluation (SANE), and visual analog scale (VAS) pain and VAS patient satisfaction scores of both shoulders.22232425) All procedures were performed by one of five fellowship-trained shoulder and elbow surgeons (CLG, MDL, MLR, GRW, JAA). All surgeries were performed either through a standard deltopectoral approach or through a superolateral deltoid–splitting approach if prior surgical incisions required this approach.26) Full details of the surgical procedures can be found in Table 1. All patients were immobilized in a sling for 2–4 weeks postoperatively and then were enrolled in a standardized postoperative physical therapy protocol. The main difference in rehabilitation protocols was that patients undergoing TSA begin passive FE and passive ER starting the day of surgery while RSA patients typically do not. All patients begin active assisted ROM at 6 weeks and then begin strengthening at 12 weeks.
Study population characteristics are reported by using measures of central tendency (mean) and variability (standard deviation). Patients' shoulders were compared by using independent samples t-tests for continuous variables and chi-square analyses for categorical variables to detect differences between groups. For all statistical tests, a p-value < 0.05 was used to determine significance. All statistics were calculated with Microsoft Excel (2013; Microsoft, Redmond, WA, USA).
RESULTS
Patient Demographics and Clinical Characteristics
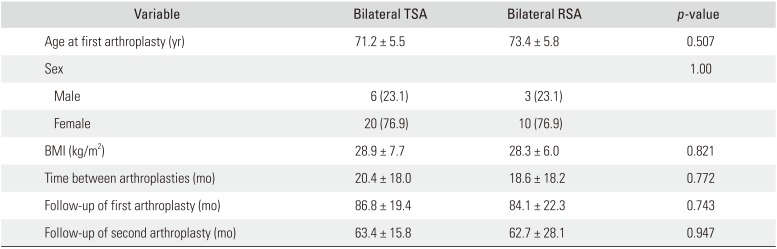
A summary of patient demographics and clinical characteristics is shown in Table 2. After application of the matching criteria, there were no significant differences in age at first arthroplasty surgery (71.2 ± 5.5 vs. 73.4 ± 5.8 years, p = 0.507), percentage of male or female patients (p = 1.00), or body mass index (28.9 ± 7.7 vs. 28.3 ± 6.0 kg/m2, p = 0.821) between bilateral TSA and bilateral RSA cohorts. There were also no significant differences in time between arthroplasties (20.4 ± 18.0 vs. 18.6 ± 18.2 months, p = 0.772), follow-up from first arthroplasty (86.8 ± 19.4 vs. 84.1 ± 22.3 months, p = 0.743), or follow-up from second arthroplasty (63.4 ± 15.8 vs. 62.7 ± 28.1 months, p = 0.947) between these two cohorts. There were no intraoperative complications.
Shoulder ROM
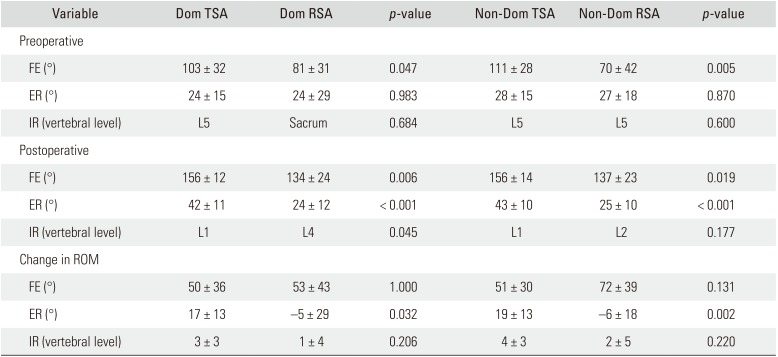
Shoulder ROM was compared between dominant (Dom) and nondominant (non-Dom) sides of the shoulder instead of right versus left to avoid the confounding effect of hand dominance (Table 3). Patients who underwent bilateral TSA had significantly better preoperative FE of their Dom (103° ± 32° vs. 81° ± 31°, p = 0.047) and non-Dom (111° ± 28° vs. 70° ± 42°, p = 0.005) arms compared to patients who underwent bilateral RSAs. There were no significant differences in preoperative ER between Dom (24° ± 15° vs. 24° ± 29°, p = 0.983) and non-Dom (28° ± 15° vs. 27° ± 18°, p = 0.870) arms or preoperative IR between Dom (L5 vs. sacrum, p = 0.684) and non-Dom (L5 vs. L5, p = 0.600) arms in patients who underwent bilateral TSAs or RSAs.
In regards to postoperative ROM, patients who underwent bilateral TSAs had significantly better FE of their Dom (156° ± 12° vs. 134° ± 24°, p = 0.006) and non-Dom (156° ± 14° vs. 137° ± 23°, p = 0.019) arms, ER of their Dom (42° ± 11° vs. 24° ± 12°, p < 0.001) and non-Dom (43° ± 10° vs. 25° ± 10°, p < 0.001) arms, and IR of their Dom arm (L1 vs. L4, p = 0.045) compared to patients who underwent bilateral RSAs. There was no significant difference in IR of their non-Dom arms (L1 vs. L2, p = 0.177).
Patients who underwent bilateral TSAs had significantly better overall improvement in ER of their Dom (17° ± 13° vs. −5° ± 29°, p = 0.032) and non-Dom (19° ± 13° vs. −6° ± 18°, p = 0.002) arms compared to patients who underwent bilateral RSAs. There were no significant differences in overall ROM improvement between bilateral TSAs and bilateral RSAs in FE of their Dom (50° ± 36° vs. 53° ± 43°, p = 1.000) or non-Dom (51° ± 30° vs. 72° ± 39°, p = 0.131) arms or IR of their Dom (3 ± 3 vertebral levels vs. 1 ± 4 vertebral levels, p = 0.206) or non-Dom (4 ± 3 vertebral levels vs. 2 ± 5 vertebral levels, p = 0.22) arms.
Functional Outcomes Scores
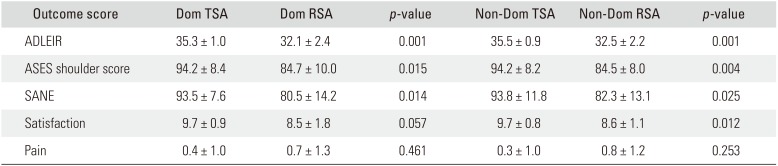
Functional outcome scores were also compared according to hand dominance to avoid any confounding effect. Patients who underwent bilateral TSAs had significantly better ADLEIR scores of their Dom (35.3 ± 1.0 vs. 32.1 ± 2.4, p = 0.001) and non-Dom (35.5 ± 0.9 vs. 32.5 ± 2.2, p = 0.001) arms, ASES scores of their Dom (94.2 ± 8.4 vs. 84.7 ± 10.0, p = 0.015) and non-Dom (94.2 ± 8.2 vs. 84.5 ± 8.0, p = 0.004) arms, and SANE scores of their Dom (93.5 ± 7.6 vs. 80.5 ± 14.2, p = 0.014) and non-Dom (93.8 ± 11.8 vs. 82.3 ± 13.1, p = 0.025) arms, and were more satisfied with their non-Dom arms (9.7 ± 0.8 vs. 8.6 ± 1.1, p = 0.012) compared to bilateral RSA patients (Table 4). There were no significant differences in satisfaction of their Dom arms (9.7 ± 0.9 vs. 8.5 ± 1.8, p = 0.057) or VAS pain scores of their Dom (0.4 ± 1.0 vs. 0.7 ± 1.3, p = 0.461) and non-Dom (0.3 ± 1.0 vs. 0.8 ± 1.2, p = 0.253) arms.
Complications and Reoperations
There were no intraoperative complications for patients in either cohort. In the TSA cohort, 1 patient had a postoperative hematoma that required an irrigation and debridement 6 weeks postoperatively, 1 patient underwent an arthroscopic distal clavicle excision 2 years postoperatively for acromioclavicular joint arthritis, and 1 patient underwent an open reduction and internal fixation (ORIF) for a clavicle fracture sustained over 3 years postoperatively. In the RSA cohort, 1 patient sustained an acromioclavicular joint separation 4 years postoperatively that was treated nonoperatively and 1 patient sustained a periprosthetic fracture 2 years postoperatively that was treated with ORIF. There were no dislocations, infections, or nerve injuries in either cohort.
DISCUSSION
This retrospective cohort comparison shows that in general patients who received bilateral TSAs had better postoperative ROM and patient-reported functional outcomes than patients who received bilateral RSAs. Patients with bilateral TSAs had better postoperative ROM in every measured plane except IR of their non-Dom arms. However, the only plane in which bilateral TSA patients had significantly better improvement in ROM was ER. Bilateral TSA patients also had significantly better functional outcome scores (ASES, SANE, and ADLEIR) than did their bilateral RSA counterparts. Despite the superior functional outcome scores in the bilateral TSA cohort, these two groups had equal final satisfaction for their Dom arms and equal pain relief (VAS pain score) in both arms.
Surgeons remain concerned with the ability of patients to perform all of their ADLs after RSA given the inherent limitations in IR with this arthroplasty design. However, recent evidence suggests that these deficits may not be as profound as previously thought. Stevens et al retrospectively reviewed the outcomes of 15 consecutive patents who underwent staged bilateral RSA for CTA and found that all patients were able to adequately perform ADLs that require IR including maintaining perineal hygiene.13) Wirth et al.14) reported the results of 57 staged bilateral RSAs at least 1 year from their second arthroplasty surgery and found that at 1 year postoperatively 21% of patients had insufficient IR after their first surgery and 33% had insufficient IR after their second surgery. However, at 2 years postoperatively, only 5% of patients lacked sufficient IR bilaterally. At a mean follow-up of 48.4 months, Levy et al.11) reported the results of 19 patients who underwent staged bilateral RSAs and all patients had no limitations in their leisure activities or ADLs including maintaining perineal hygiene. In the largest cohort study published to date, Mellano et al.12) retrospectively reviewed 50 patients who underwent staged bilateral RSA for CTA, OA, massive rotator cuff tear, or revision shoulder arthroplasty and found that all patients remained independent with ADLs and personal hygiene 2 years postoperatively. All of these studies clearly demonstrate that patients can remain functional with bilateral RSAs. Similarly, all of the patients in our bilateral RSA cohort reported that they were able to adequately maintain personal hygiene. While the bilateral TSA cohort had superior functional outcomes and superior ADL scores (over 35/36 in ADLEIR testing for both arms), the bilateral RSA cohort still achieved reasonable ADL scores (over 32/36 in both arms).
Certainly, this study has several weaknesses. First, this is a purely retrospective study and is therefore subject to the limitations of retrospective data specifically on the inability to elucidate causal relationships rather than simply correlative ones. The ROM measurements were obtained by retrospectively reviewing the physical examinations dictated by physicians. These measurements would be more accurate if they were assessed using a goniometer. We did not have preoperative patient-reported functional outcome scores or ADLEIR scores to compare with the postoperative scores and therefore could not assess net improvement in functional outcomes between cohorts. There were also some variations in surgical details and specific TSA and RSA systems patients received may have influenced the results. However, all procedures were performed by high-volume fellowship-trained shoulder and elbow surgeons, so we do not believe these variations would significantly affect the results. Additionally, this sample size may be underpowered to show a significant difference between cohorts. This is an inherent limitation of a retrospective analysis and cannot be modified. Despite these weaknesses, we were able to achieve a direct matched comparison of bilateral TSA to RSA. We found superior functional outcomes in the bilateral TSA cohort, equal pain relief in both cohorts, and a satisfactory ability to perform ADLs in both cohorts.
Overall, patients who underwent bilateral TSAs for OA and bilateral RSAs for CTA exhibited improved ROM and patient-reported functional outcomes. Patients who underwent bilateral TSAs had superior functional results to patients who underwent bilateral RSAs. Both groups exhibited equal pain relief. Despite the difference in functional results, patients with bilateral RSAs were satisfied with their results and able to perform their ADLs with minimal limitations.
 XML Download
XML Download