

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the fifth most common cancer worldwide and the second leading cause of cancer-related death.12 Liver cirrhosis is the most important risk factor for the development of HCC and present in > 85% of patients with HCC.34 Portal hypertension derived from liver cirrhosis commonly causes splenomegaly, which may lead to a decrease of hematologic indices, such as thrombocytopenia by splenic sequestration.5 Hence, a significant number of patients with HCC are associated with thrombocytopenia secondary to hypersplenism. This hematologic abnormality can adversely affect the critical treatment for HCC by limiting their treatment options and delaying the planned diagnostic or therapeutic procedures, because cirrhotic patients with severe thrombocytopenia are at high risk for bleeding and mortality.6789
Transarterial chemoembolization (TACE) has been widely performed in patients with HCC who are not amenable to curative treatment modality based on the advanced tumor stages, and this stratum of patients showed a survival benefit from TACE.1011121314 However, in some patients with HCC with cirrhosis, this treatment option could not be applied due to severe thrombocytopenia, which is likely to result in uncontrolled bleeding during and after the procedure. In addition, chemotherapeutic agents during TACE may also induce and worsen peripheral cytopenia through myelosuppression.15
Owing to the lack of effective pharmacologic therapies currently available to increase platelet count, surgical splenectomy has been performed in these situations but has been discontinued due to high mortality rate.1617 Instead, partial splenic embolization (PSE) was proposed as an alternative strategy to surgery for improving severe thrombocytopenia due to hypersplenism.18 PSE via splenic arterial catheterization to occlude a portion of the splenic arterial blood flow resulting in partial splenic necrosis is a minimally invasive approach with low mortality and has been known to be an effective method to treat hypersplenism in cirrhotic patients with severe thrombocytopenia.81619202122 It may enable HCC patients with severe thrombocytopenia related to splenomegaly to undergo TACE procedures. Although several studies have reported the positive clinical results of combination therapy with PSE and TACE for HCC patients with severe thrombocytopenia, to the best of our knowledge, the long-term clinical results of more than 1 year of PSE treatment combined with TACE in HCC patients with severe thrombocytopenia have not been reported.152324 Therefore, the current study aimed to evaluate the long-term efficacy and safety of PSE combined with TACE in HCC patients with severe thrombocytopenia.
METHODS
Study population
The study population consisted of HCC patients with thrombocytopenia (< 100 × 109/L) related to splenomegaly caused by liver cirrhosis, who underwent TACE for the treatment of HCC at Kangbuk Samsung Hospital from January 2006 to June 2016 (n = 934). Of these patients, 18 with HCC underwent additional PSE concurrently with TACE (PSE group) due to severe thrombocytopenia (< 50 × 109/L). Four controls per patient (n = 72) were randomly selected from the HCC patients with thrombocytopenia related to splenomegaly who underwent TACE alone (non-PSE group) during the same study period.
HCC was diagnosed based on the recommendations of the European Association for the Study of the Liver or American Association for Study of Liver Disease guidelines.12 TACE was recommended as the initial treatment for patients with asymptomatic, large, multifocal HCC without main portal vein invasion, and extrahepatic spread, which were unsuitable for hepatic resection or radiofrequency ablation if patients had preserved hepatic function.25 All TACE and PSE procedures were performed by an experienced interventional radiologist with more than 10 years of experience for radiologic intervention in our institution.
Measurements and definitions
Data of clinical, laboratory, and radiologic findings of enrolled patients were retrieved by retrospective review of electronic medical records and imaging findings in PACS program (Infinitt®; INFINITT Healthcare, Seoul, Korea). All patients underwent blood tests, including hemoglobin concentration, platelet count, leukocyte count, alfa-fetoprotein (AFP) level, liver enzymes, coagulation profile, and creatinine level during the procedures and at each subsequent clinic visit after procedures until the last follow-up. Enhanced computed tomography (CT) was performed in all patients in the PSE group before and 1 month after PSE to measure the splenic infarction rate.
HCCs were diagnosed by either a four-phase multi-detector row CT scan or dynamic contrast-enhanced magnetic resonance imaging.12 The lesion was diagnosed as HCC if the appearance was typical for HCC (i.e., hypervascular in the arterial phase followed by washout in the portal venous or delayed phase).12 Ultrasonography-guided percutaneous liver biopsy was performed for confirmative diagnosis if the findings were not characteristic or vascular profile was atypical.12 Cirrhosis was defined clinically when cirrhotic configuration of the liver (nodular liver surface or caudate lobe hypertrophy), and/or splenomegaly was confirmed, or when varices (abnormally enlarged veins, detected by upper endoscopy or cross-sectional images) were present.26 Splenomegaly was diagnosed when the largest diameter of the spleen in transverse planes of CT (the greatest anteroposterior dimension at the splenic hilum) exceeded 12 cm. The splenic infarction rate was defined as the proportion of infarcted splenic volume from the pre-infarction splenic volume. The infarcted splenic volume was calculated as the difference in the splenic volume before and after PSE.
Technique of PSE
Under strict aseptic condition, a 5.0 French catheter (Terumo, Tokyo, Japan) was inserted into femoral artery by the Seldinger method. Celiac angiography and selective splenic arterial angiography were routinely performed to determine the distribution of splenic arteries and collateral circulation. After superior, middle, and inferior splenic segmental arteries were inspected by angiography, dominant segmental arteries of splenic artery were superselected by co-axial technique using 3 French microcatheter (Progreat; Terumo) and 0.016-inch guide wire (GT; Terumo). Embolization of dominant segmental arteries of splenic artery was performed using 355-500 microm polyvinyl alcohol particles (Cook Inc., Bloomington, IN, USA), gelfoam (Cutanplast, Mascia Brunelli, Italy), and microcoils (Nester and/or Tornado coils; Cook Inc.). The therapeutic target of embolization was a splenic infarction rate of 70% to 80%. Intravenous prophylactic antibiotics were administered to the all patients who underwent PSE.
Statistical analysis
Data were expressed as mean ± standard deviation (SD), median (interquartile range [IQR]) or frequencies (%). The baseline characteristics between PSE and non-PSE groups were compared using the χ2 analysis or Fisher exact test for categorical variables and Student's t-test for continuous variables. The changes in platelet count, leukocyte count, hemoglobin levels, and Child-Turcotte-Pugh (CTP) scores at several time points from baseline were compared using a paired sample t-test, and these values between the two groups were compared using the Student's t-test. The association between the splenic infarction rate and increased platelet counts was analyzed using the simple correlation analysis (Spearman rank correlation coefficient). All reported P values were two-tailed, and a P value < 0.05 was considered statistically significant. SPSS software version 21 (IBM Corp., Armonk, NY, USA) was used to perform all statistical analyses.
RESULTS
Baseline characteristics of the study population
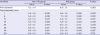
Of 90 HCC patients with thrombocytopenia related to splenomegaly, 18 underwent PSE concurrently in addition to TACE (PSE group) and 72 underwent TACE alone (non-PSE group). The baseline characteristics of the study participants based on performing additional PSE status are summarized in Table 1. The leukocyte (3,873.7 vs. 2,261.1; P = 0.001) and platelet counts (66.3 vs. 33.7 × 109/L; P < 0.001) at baseline in the non-PSE group were significantly higher than those in the PSE group. However, no significant difference was found in other baseline characteristics, including age, proportion of men subjects, etiology of cirrhosis, CTP class, laboratory findings (hemoglobin, aspartate aminotransferase, alanine aminotransferase, total bilirubin, international normalized ratio, albumin, and creatinine levels), AFP, tumor stages, or the type and dosage of chemoembolization drugs between the two groups. In addition, the majority of patients in this study had chronic hepatitis B (74.4%, 67/90) and among patients with chronic hepatitis B, the degree of viral suppression (response to antiviral therapy) such as virological remission, virological breakthrough, and suboptimal virological response, which may affect the changes of platelet concentration was not significantly different between the two groups (P = 0.126, P = 0.490, and P = 0.183, respectively, data not shown).
Table 1
Baseline characteristics of study population between PSE vs. Non-PSE group

Long-term clinical outcomes after PSE
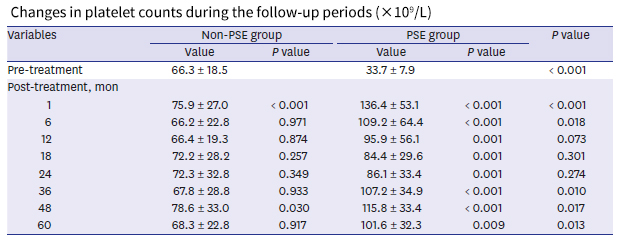
The changes in platelet count after treatment during the study periods are shown in Table 2. In the PSE group, the mean platelet counts at 1 month, and 1, 3, and 5 years after treatment significantly increased compared with baseline (1 month, and 1, 3, and 5 years vs. baseline; 136.4 ± 53.1, 95.9 ± 56.1, 107.2 ± 34.9, and 101.6 ± 32.3 × 109/L vs. 33.7±7.9 × 109/L; all P < 0.05), whereas the platelet count did not increase significantly in the non-PSE group during most of the treatment period. In addition, although the baseline platelet count was significantly lower in the PSE group than that in the non-PSE group (33.7 ± 7.9 × 109/L vs. 66.3 ± 18.5 × 109/L; P < 0.001), the platelet count at 1 and 6 months, and 3 and 5 years after treatment in the PSE group was significantly higher than those in the non-PSE group (1 month, 136.4 ± 53.1 × 109/L vs. 75.9 ± 27.0 × 109/L, P < 0.001; 6 months, 109.2 ± 64.37 × 109/L vs. 66.2 ± 22.8 × 109/L, P = 0.018; 3 years, 107.2 ± 34.9 × 109/L vs. 67.8 ± 28.8 × 109/L, P = 0.010; and 5 years, 101.6 ± 32.3 × 109/L vs. 68.3 ± 22.8 × 109/L, P = 0.013). The median splenic infarction rate in the PSE group was 77.8% (IQR, 67.2–86.4), and a significant positive association between the rate of splenic infarction and increase in platelet counts at 6 months and 1 year after PSE procedure was observed (6 months: r = 0.606, P = 0.008; 12 months: r = 0.478, P = 0.045, data not shown).
Table 2
Changes in platelet counts during the follow-up periods (×109/L)
Table 3 shows the changes in leukocyte counts and platelet levels after treatment during the study periods. In the PSE group, the mean leukocyte count at 1 month, 1, 3, and 5 years after treatment significantly increased compared with baseline (1 month, 1, 3, and 5 years vs. baseline; 5,438.3 ± 2,743.7, 5,122.9 ± 2,857.1, 4,193.3 ± 712.6, and 4,970.0 ± 1,963.9 vs. 2,261.1 ± 990.3; all P < 0.05), whereas the leukocyte count did not increase significantly after treatment in the non-PSE group (all P > 0.05). In addition, although the baseline leukocyte count in the PSE group was significantly lower than that in non-PSE group (2,261.1 ± 990.3 vs. 3,873.7 ± 1,946.7; P < 0.001), no significant difference was found in the leukocyte count between the PSE and non-PSE groups after treatment (all P > 0.05). The mean hemoglobin levels at 1, 3, and 4 years after treatment significantly increased compared with baseline in the PSE group (1, 3, and 4 years vs. baseline; 13.0 ± 2.0, 13.6 ± 1.9, and 13.5 ± 2.0 vs. 11.6 ± 1.8; all P < 0.05), whereas the hemoglobin levels did not increase significantly after treatment in the non-PSE group.
Table 3
Changes in leukocyte counts and hemoglobin concentrations during the follow-up periods
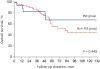
The clinical outcomes of the two groups during the study periods were compared in Table 4. The mean transfused amount of packed red blood cell and fresh frozen plasma in the PSE-group was not significantly lower than that in the non-PSE group (P = 0.520 and P = 0.828, respectively). The mean number of hospitalization from any cause and TACE-related hospitalization periods were not significantly different between the two groups (P = 0.322 and P = 0.433, respectively). Additionally, the overall survival was not significantly different between the two groups (P = 0.499, Fig. 1). However, the mean transfused amount of platelet concentration was significantly lower in the PSE-group than non-PSE group (7.9 vs. 18.6; P = 0.040), and the mean number of serially performed TACE procedures was significantly higher in the PSE group than non-PSE group (6.8 vs. 4.1; P = 0.046), although the mean follow-up periods between the two groups did not significantly differ (P = 0.442).
Table 4
Clinical outcomes during the follow-up periods
Safety of PSE
There was no significant deterioration in CTP scores after treatment in the PSE group throughout the study periods (Table 5). Although the CTP scores at 1 and 6 months after treatment in the PSE group were significantly higher than those in the non-PSE-group (1 month, 6.8 ± 1.4 vs. 5.9 ± 1.0, P = 0.003 and 6 months, 7.1 ± 1.9 vs. 5.9 ± 1.2, P = 0.032), the difference in the CTP scores between the two groups disappeared after those time points (all P < 0.05).
Table 5
Changes in Child-Turcotte-Pugh scores during the follow-up periods
Severe adverse events, such as sepsis, large pleural effusion with ascites, and variceal bleeding occurred in two (11.1%) and seven (9.7%) patients in the PSE and non-PSE groups, respectively, and no significant difference was found between the two groups (P = 0.861, data not shown) throughout the median observation period of 42.5 months (IQR, 21.5–61.0). No cases of splenic rupture, portal vein thrombosis, liver failure, or death were reported immediately after the PSE procedure.
DISCUSSION
This study retrospectively evaluated the clinical outcomes of PSE in HCC patients with severe thrombocytopenia. To the best of our knowledge, this is the first study that assessed the long-term efficacy and safety of PSE in HCC patients with severe thrombocytopenia who underwent TACE as treatment for HCC, with a median follow-up period of 42.5 months (IQR, 21.5–61.0 months). We found that the platelet and leukocyte counts and hemoglobin concentrations after the concurrent PSE and TACE procedure significantly increased compared with baseline, without deterioration of CTP score and unexpected side effects, and these clinical benefits persisted until the end of the follow-up period. In addition, although the baseline platelet count in the PSE group was significantly lower than that in the non-PSE group, the platelet counts at several time points after treatment in the PSE group were significantly higher than those in the non-PSE group. The platelet increase after PSE significantly reduced the need for platelet transfusions and enabled the subsequent TACE procedures in time. Our results suggest that PSE helps to perform initial and serial TACE for the treatment of HCC by long-term stabilization of hematologic parameters with well-tolerability, in HCC patients with severe thrombocytopenia related to splenomegaly.
Thrombocytopenia in patients with liver cirrhosis can be caused by shift of platelet distribution to an enlarged spleen, immunologically mediated platelet destruction, and decreased production of thrombopoietin.72728 The presence of thrombocytopenia in cirrhotic patients makes TACE procedures difficult because of the high incidence of hemorrhagic complications and their related mortality during and after the procedures.924 In clinical practice, prophylactic platelet transfusions are administered to mitigate the risk of bleeding in these cases. However, there is no current universal agreement on the use of prophylactic platelet transfusions, which may lead to serious complications, such as transfusion reaction, severe infection, and refractoriness to repetitive platelet transfusions. Surgical splenectomy is another treatment option for patients with thrombocytopenia. However, it is invasive and reported to be associated with high incidence of portal vein thrombosis and mortality.161729
Several studies have reported the positive results on the efficacy of PSE for HCC patients with thrombocytopenia caused by liver cirrhosis and supported its use in the treatment of hypersplenism, which is consistent with our results.15232430 One prospective study from China, including 50 HCC patients with hypersplenism caused by cirrhosis, showed that platelet and leukocyte counts after combined one-step TACE/PSE treatment were significantly higher compared with baseline during the three-month follow-up period (P < 0.001), whereas those after TACE alone were significantly lower compared with baseline (P < 0.001).15 A Japanese study including 101 HCC patients with thrombocytopenia showed that the platelet count at 2 weeks and 6 months after concurrent TACE/PSE was significantly higher than those after TACE alone (2 weeks; 10.2 vs. 4.5 × 104/mL, P < 0.05 and 6 months; 8.4 vs. 6.5 × 104/mL, P < 0.05), and the hepatic functional reserve was maintained although PSE was performed concurrently with TACE.24 Another study from Japan including 21 HCC patients with severe thrombocytopenia (platelet count < 5.0 × 104/mm3) also documented that 81% (17/21) of patients showed an increase in platelet count to ≥ 5.0 × 104/mm3 after simultaneous PSE and TACE for 1 month.23 However, the follow-up period of the previous studies was relatively short (1–6 months).
Recently, avatrombopag, a novel, oral, small-molecule thrombopoietin receptor agonist was developed for thrombocytopenic patients with chronic liver disease to increase their platelet count.31 In ADAPT-1 and ADAPT-2 phase 3 randomized controlled trials, avatrombopag was superior to placebo in reducing the need for platelet transfusions or rescue procedures for bleeding in patients with thrombocytopenia and chronic liver disease undergoing a scheduled procedure (all P < 0.001).31 However, the magnitude and duration of the increase in platelet count with avatrombopag in the ADAPT trials was short; platelet counts peaked 5–8 days after the last dose of the drug and then consistently declined within 7 days of the procedure, returning to baseline within 30 days of the last dose.31
On the contrary, the present study showed significant long-term efficacy of PSE on the improvement of thrombocytopenia in HCC patients with splenomegaly caused by liver cirrhosis who underwent TACE concurrently. The platelet-increasing effect after PSE in our study continued not only for 1 year but was also observed during a median follow-up of 42.5 months (IQR, 21.5–61.0 months). In addition, the platelet increase from PSE significantly reduced the need for platelet transfusions and enabled the subsequent TACE procedures in time, although it did not significantly reduce the occurrence of bleeding events requiring treatment and TACE-related hospitalization periods and did not achieve better overall survival. Improvement of thrombocytopenia was also accompanied by a marked increase in leukocyte counts and hemoglobin concentrations after PSE treatment, and the increase of these values were sustained until the end of their follow-up period. This is in line with the results of previous studies showing that PSE exerted maintenance effects on leukocyte counts and hemoglobin concentrations, as well as platelet counts.20303233
With regard to tolerability and safety, in the present study, 11.1% (2/18) of patients in the PSE group experienced adverse events, including pleural effusion with ascites, sepsis due to spontaneous bacterial peritonitis, and variceal bleeding after concurrent PSE and TACE, and they are not significantly different compared with those in the non-PSE group. Most of the complications that occurred after PSE and TACE treatment were temporary and controllable. These are consistent with positive results of previous studies on the safety of PSE.152430 In addition, there was no significant deterioration of CTP scores after PSE and TACE during the study period. The reason why the CTP scores of the PSE group at 1 and 6 months after treatments was higher than those of non-PSE group would be temporary improvement of CTP scores in the non-PSE group, not deterioration of CTP scores in the PSE group, although the exact mechanism for the temporary improvement of the CTP score in the non-PSE group could not be explained. Indeed, PSE has been reported to be effective not only in improving cytopenia, but also in enhancing hepatic functional reserve and hepatic protein synthesis by decreasing splenic blood flow and increasing hepatic artery and superior mesentery artery blood flow.2434
The present study has several limitations. First, this study was retrospective, hospital-based rather than population-based, and our cohort was recruited from a single tertiary medical center in Korea. Therefore, there was likely some degree of selection bias and care must be taken when generalizing our conclusion. On the other hand, all PSE and TACE procedures in our study were performed by one experienced interventional radiologist. Therefore, we could minimize technical discrepancy that may arise from different interventional radiologists within different facilities. Second, the accurate additional costs and procedure time resulting from the combination of PSE to TACE could not be calculated in this study, although there were no differences in the peri- and post-procedural complications between the two groups. Lastly, the number of enrolled patients in this study was relatively small and some of them (36.7%) were follow-up loss during the study periods. However, the proportion of the patients with follow-up loss due to any cause was not significantly different between the two groups (22.2% vs. 40.3% in the PSE and non-PSE group, respectively; P = 0.155), and the median follow-up period for the patients with follow-up loss was not short (32 months [IQR, 20.0–54.5 months]). A further multicenter prospective study with larger sample size is required to confirm our results.
Despite these limitations, our data provided significant information on long-term clinical outcomes of PSE combined with TACE for HCC patients with thrombocytopenia related to splenomegaly. Concurrent PSE with TACE is effective in inducing and maintaining thrombocytopenia improvement which reduces the need for the platelet transfusion and helps to perform initial and serial TACE, and is well-tolerated in HCC patients with thrombocytopenia. Our results support that PSE may be a promising treatment option for HCC patients with severe thrombocytopenia associated with splenomegaly who will undergo TACE for the treatment of HCC.
 XML Download
XML Download