

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Optimal growth and development of the brain and central nervous system is of paramount importance during the first 1000 days, the period from conception through to a child's second birthday, and largely depends on adequate nutrition, including that of long-chain polyunsaturated fatty acids (LCPUFAs) [12]. The most abundant LCPUFAs in the brain and those critical for proper development and function of the brain, nervous system, and eye are n-3 docosahexaenoic acid (DHA; 22:6n-3) and n-6 arachidonic acid (AA; 20:4n-6) [3]. DHA and AA are either obtained directly from the diet or synthesized in the body from the essential fatty acids (FAs), linoleic acid (LA; 18:2n-6) and α-linolenic acid (ALA; 18:3n-3), through a multi-step process that is slow and inefficient in humans [4]. The rapid accretion of DHA in cellular membranes of the central nervous system is required for optimal development of the retina and brain during late fetal development through the first two years of life [56]. Similarly, AA has a structural role in the brain as well as plays a role in rapid growth and development of the nervous system. Proper cognitive and visual development during early life is associated with the presence of adequate DHA and AA concentrations in breastmilk or infant formula [78]. Fetuses and breastfed infants are entirely dependent on the maternal dietary status of these FAs, AA and DHA are preferentially transported across the placenta during the prenatal period [9], and human milk provides both DHA and AA after birth [10].
Infants and young children have high nutritional demands in order to support adequate growth and development, particularly during the transition from complementary feeding at 12 months of age to a mixed and varied diet at 36 months of age [11]. Only certain foods contain LCPUFAs at concentrations sufficient for these needs. Additionally, fatty fish rich in DHA may not be regularly provided to infants due to concerns about potential food allergies or methylmercury exposure [4]. Although dietary recommendations for LCPUFAs and essential FAs in late infancy and early childhood (6–24 months) are specifically emphasized for this age range, they vary widely across the world. Optimal intake levels are not conclusively established and there are little data to estimate daily intake of preformed LCPUFAs in late infancy and early childhood [4]. It also remains unclear which foods are the greatest contributors to PUFA intake among infants and young children in South Korea, whose diet may differ from those of Korean adults [12]. Infants and young children may be nutritionally vulnerable, especially if they consume a restricted range of foods or an energy-rich but nutrient-poor diet [11].
To address these literature gaps, this study utilized crosssectional data from the 2010–2015 Korea National Health and Nutrition Examination Survey (KNHANES) to estimate the daily dietary intake of LCPUFAs (EPA, DHA, and AA) and essential FAs (ALA and LA) among toddlers aged 12–24 months. Dietary intakes were compared to those estimated for exclusively breastfed infants aged 0–5 months, intakes estimated from national representative data on non-Korean toddlers, and international dietary recommendations. The study also identified the key dietary sources of LCPUFAs and essential FAs in the toddler diets.
SUBJECTS AND METHODS
Study design and participants
The KNHANES is a population-based, cross-sectional survey designed to assess the health-related behavior, health condition, and nutritional status of the Korean population [13]. Since 1998, the KNHANES has been periodically conducted by the Korea Centers for Disease Control and Prevention (KCDC). In 2007, the KNHANES sample design changed to an on-going annual survey to avoid seasonal variance [14]. The KNHANES uses a stratified, multistage, and clustered probability sampling design to select household members aged 12 months or older. It consists of a health interview survey, health examination survey (physical examination, clinical measurements, and tests), and nutrition survey.
This study protocol was reviewed and approved by the Institutional Review Board of the KCDC (2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07CON-03-4C, 2013-12EXP-03-5C, and 2015-01-02-6C). Written informed consent was obtained from all subjects. Detailed information about the survey is available at http://knhanes.cdc.go.kr.
A total of 48,482 participants completed the fifth (2010–2012) and sixth (2013–2014) KNHANES. Toddlers aged 12–24 months were included in the data analysis. Of the original 669 age-eligible toddlers, 35 toddlers were excluded with missing data on dietary intake. Toddlers who were breastfed (n = 83) and mixed-fed (n = 5) at the time of the study were also excluded, due to insufficient information on the amount of breastmilk consumed.
Dietary assessment and estimation of fatty acid intake
Dietary intake data in the form of 24-h dietary recalls were collected by well-trained dietitians via face-to-face interviews with primary caregivers at participants' homes. To assess the intake of each PUFA, we used the KCDC's FA composition database, which assigns a nutrient quantity according to the reported type and amount of food consumed on a given day of the 24-h dietary recall. This database provides the FA contents for 5,144 foods. The food items were first filled with analytical values from national agencies from Korea, the United States (US), and Japan [1215]. Domestic sources were selected preferentially over foreign sources. Additionally, if nutrient information of single food items was not available, these missing values were replaced with calculated or imputed values, using the analytical values of similar food items from the data source. A total of 1,545 analytical values, 2,589 calculated values, and 1,010 imputed values were included in the FA database. It was also reported that total FA intake was estimated as 84.3% of daily total fat intake for 3,824 adults aged over 19 years in the 2011 KNHANES [15].
Since the KNHANES only contains the data of subjects aged over 12 months, other data sources were used to estimate the FA intake of infants for the first 6 months. For infants 0–5 months of age, the expected PUFA intake from breastfeeding was estimated by multiplying the PUFA content in breastmilk [10] by the average daily consumption of breastmilk (780 ml/day) by Korean infants [16]. For toddlers aged 12–24 months, an individual's daily dietary intake of FAs from selected food items was calculated by multiplying the content of each nutrient in each food item by the daily consumption value, summing across all foods consumed over the day. The probability of adequate intake was calculated by comparing each estimated intake with national and international recommendations. The major food sources of the particular PUFAs (ALA, EPA, DHA, LA, and AA) were obtained by dividing the sum of each PUFA contained in the consumed food by the sum of each PUFA intake from all consumed foods, weighted using the appropriate survey sampling weight. In this study, a total of 1,077 food items were consumed by 12–24-month-old toddlers and the KCDC's FA composition database covered 93.0% of the food items.
Statistical analysis
All data analyses were performed using SAS software (version 9.4; SAS Institute, Inc., Cary, NC, US). Due to the complex sampling design, the relevant primary sampling units, stratification, and sample weights provided by the KNHANES were considered in our analysis to produce estimates that were representative of the Korean population. For descriptive statistics, continuous variables were expressed as weighted means and standard errors of the means. Categorical variables were expressed as numbers and weighted percentages using the SAS procedures SURVEYMEANS and SURVEYFREQ, respectively.
RESULTS
Demographic characteristics
The demographic characteristics of Korean toddlers aged 12 to 24 months from 2010–2015 are shown in Table 1. The mean age and weight were 17.9 ± 0.2 months and 11.2 ± 0.1 kg, respectively. Almost half (49.7%) of the toddlers were boys. About 88% of them were breastfed, and the average age at weaning was 6.2 ± 0.1 months. Thirty-nine percent were reported to have taken dietary supplements during the first 12 months after birth while the corresponding value in toddlers aged 12–24 months was 12.2%.
Estimation of daily LCPUFA and essential FA intakes
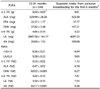
The average daily intake of n-3 and n-6 PUFAs for toddlers aged 12 to 24 months are shown in Table 2. To assess whether a noticeable reduction existed for toddlers who have been fully transitioned to family foods, the actual dietary intakes for 12–24-month-old toddlers were compared with the estimated daily intakes for infants aged 0–5 months. Dietary intakes of LCPUFAs (EPA, DHA, and AA), essential FAs (ALA and LA), and total n-3 and n-6 FAs in 12- to 24-month old toddlers tended to be lower than the estimated intake in exclusively breastfed infants aged 0–5 months (Table 2). In particular, DHA and AA intakes were 4 to 5 times lower than those of exclusively breastfed infants. An exclusively breastfed infant consumes approximately 147 mg/day DHA during the age range 0–5 months of age. The 37 mg/day average intake reported in this study corresponds to a reduction of 75%, as compared to breastfed infants. Similarly estimated average AA intake is roughly 109 for the 0–5-month age range. The 20 mg/day average intake reported in this study represents a reduction of about 82% as compared to breastfed infants. In addition, no significant differences were observed between boys and girls in the actual dietary intakes of 12–24-month-old toddlers (data not shown).
Comparison with national data and international recommendations
Table 3 compares the FA intake for 12–24-month-old Korean toddlers to those reported for toddlers in the US, the UK and Japan. Mean intakes of n-3 and n-6 FAs in Korean toddlers aged 12–24 months were similar to those reported for UK toddlers aged 12–18 months but were lower when compared to those reported for counterparts in Japan and the US.
Table 4 shows the current dietary recommendations published by national and international authorities for n-3 and n-6 FAs in late infancy and early childhood. The intake of n-3 and n-6 FAs (0.53 and 3.62 percent of energy intake [%E], respectively) was below the recommended level for Korean (> 1 and 4–10%E, respectively) and Japanese toddlers (0.78 and 5.0 g/d, respectively). ALA (0.37%E) and LA (3.50%E) intakes in Korean toddlers reached the range recommended by the FAO/WHO, but were lower than the levels recommended in the US, Europe, and Australia. The probability of adequate intake calculated following the FAO/WHO guidelines was 25.9% for ALA, and 18.9% for LA. Mean DHA intake (37 mg/day or 1.63 ± 0.39 mg/kg body weight/day) was approximately 30% lower than the Europe and 14–16% lower than the FAO/WHO recommendations. Moreover, 10.6% and 8.3% of 12–24-month-old Korean toddlers met the Europe and FAO/WHO recommendations.
Major dietary contributors to LCPUFA and essential FA intakes
The major food sources contributing to the intake of selected LCPUFAs and essential FAs among Korean toddlers were identified (Fig. 1). Except for growing-up milk, the main dietary sources of ALA and LA were soy foods (soy milk, soybean oil, and tofu; 28.2% for both ALA and LA), vegetable oils (perilla and rapeseed oils; 17.3% for ALA and 7.3% for LA), and egg (7.7% for ALA and 10.4% for LA), providing 53.2% of ALA and 41.5% of LA dietary intake, respectively. Fish and shellfish sources accounted for the majority of dietary EPA (86.3%) and DHA (97.3%) intake. More than 60.2% of EPA and 72.4% of DHA dietary intake came from anchovy, mackerel, croaker, oyster, and hairtail. Anchovy and mackerel were identified as common dietary sources of EPA (41.6%), DHA (52.5%), and AA (7.1%) intake. The majority of dietary AA intake came from pork (23.8%), chicken (18.2%), and cheese (11.7%).
DISCUSSION
To the best of our knowledge, this study is the first to estimate the dietary intake of LCPUFAs and essential FAs and also to determine the dominant food sources of these nutrients consumed by South Korean toddlers 12–24 months of age, based on a nationally representative sample. Moreover, the dietary intake among Korean toddlers was compared to the reported dietary intake of non-Korean toddlers in the same age range from national representative data and current international dietary recommendations. The present study indicates that dietary intakes of n-3 and n-6 PUFAs in Korean toddlers are lower than intakes reported in other countries, like the US [4] and Japan [18]; the mean intake of two essential FAs (ALA and LA) was below current international recommendations. In comparison to US recommendations, the intakes of total n-3 and n-6 FAs were lower, whereas the n-6:n-3 ratio was similar [19]. It has been reported that an n-6:n-3 FA or LA:ALA ratio below 4:1 is likely to result in a markedly different FA composition from that present in human milk [20]. Therefore, the recommended intake ratio ranges of 5:1–15:1 or 6:1–16:1 have been established for infant formulas and follow-up formulas [212223]. In the present study, although the Korean toddler intake ratio is similar to that of toddlers in the US [4], it was higher than those reported for toddlers in the UK [11], Japan [18], and China [24]. Thus, according to current recommendations, the diet of Korean and US toddlers is more balanced regarding n-6 and n-3 PUFA contents when compared with that of the UK and East Asian countries. In addition, Korean, US [4], and Belgian [25] toddlers obtained LCPUFAs from similar sources: fish and shellfish for EPA and DHA; and meat, poultry, and fish for AA. However, the major food sources of essential FAs for toddlers in Korea were distinct from sources for toddlers in the US and Belgium. Soy foods, vegetable oils, and eggs contributed to a significant proportion of both LA and ALA in Korean toddler diets, while fats and oils (mainly margarines), sweet products, and cereals were the main sources for both ALA and LA in Belgian toddler diets. In the US toddler's diet, ALA intake was obtained from milk and yogurt; grains; and poultry and LA intake was obtained from nuts, seeds and salty snacks; poultry; and grains.
Sufficient intake of LCPUFAs and essential FAs should be ensured during the first 1,000 days of life, as this is the period when nutrient-sensitive brain and neural development occurs [12]. This led us to compare the dietary intake of PUFAs by Korean toddlers aged 12–24 months with the expected PUFA intake of exclusively breastfed infants aged 0–5 months to determine if there is a noticeable reduction when toddlers are transitioned from breastmilk and/or formula to family foods. This study was unable to formally compare the PUFA intakes of infants aged 0–5 months with intakes of 12–24-month-old toddlers because the KNHANES does not collect data on the nutrient content of breast milk. However, using assumptions about the PUFA content in the breastmilk of Korean mothers [10] and the average daily consumption of breastmilk [1617], we estimated the PUFA intake by infants aged 0–5 months. Dietary intakes of LCPUFAs and essential FAs in 12–24-month-old toddlers tended to be lower than that estimated for exclusively breastfed infants aged 0–5 months. The mean DHA and AA intakes were 37 and 20 mg/day, respectively, corresponding to reductions of approximately 75% and 82% compared with the estimated intakes by exclusively breastfed infants. Dietary DHA and AA intakes in 12–24-month-old toddlers declined noticeably, due to the limitation of food sources. This result suggests that young children are nutritionally vulnerable during this food transition period [26]. Dietary DHA and AA are important for neurodevelopment, given the requirement of these two FAs for the growing and developing brain [327]. Conversion rates in the body from ALA and LA to DHA and AA, respectively, are known to be extremely low [27]. Therefore, ensuring a sufficient dietary supply of these two nutrients is critical for growth and development of the brain and immune system in late infancy and early childhood, while the transitioning from complementary feeding to a mixed and varied diet occurs. Plant-based complementary foods are insufficient to meet the physiological demands for DHA and AA, and intake of foods high in DHA and AA (i.e., meat, poultry, fish or egg yolks) need to be promoted [27]. Selection of complementary foods should require consideration of DHA and AA contents to ensure adequate intake during dietary transitioning [28].
Dietary DHA intake was higher in Korean toddlers (37 mg/day) than their US counterparts (20 mg/day) of the same age [4] while AA intake showed the opposite trend (20 versus 56 mg/day). This result suggests that the marked differences in the DHA intake between Korean toddlers and toddlers in other populations are consistent with differences in consumptions patterns of seafood (i.e., fish and shellfish) according to geographical factors. It has already been demonstrated that the consumption of DHA among lactating women in the coastland areas of China is higher than that for women living in inland regions [29]. Korea is a peninsula surrounded by sea on the east, south, and west sides, with mountainous inland areas in the center. The Korean adult population consumes higher quantities of fish and shellfish than the US adult population [30]. Furthermore, even though predominant dietary sources of DHA and EPA include fish, shellfish, and poultry, only slightly more than half of children surveyed by NHANES consume any fish [4]. Although DHA intake is extremely low in landlocked countries when compared with island countries, AA intakes are higher, reflecting relatively high meat consumption [31]. Nonetheless, dietary DHA intake is still lower than the current recommendations. This result highlights the need for efforts to increase dietary DHA intake during the second year of life.
In addition to absolute amounts of DHA and AA intake, the optimal ratio between these quantities has been recently recognized as important for optimal growth and development of infants and young children. In 2009, the European Food Safety Agency (EFSA) reviewed a proposed health claim establishing a new target AA:DHA ratio of between 1.4:1 and 2:1 in infant and follow-on formula, but concluded that the presented data were insufficient to establish a cause-and-effect relationship between the intake of formula supplemented with DHA and AA and the contribution to normal brain development in infants and young children between birth and 3 years of age [32]. However, at present, this notion has been challenged by many publications providing evidence that endogenous synthesis is low, and adequate dietary supplies of AA, with a concomitant supply of DHA, have positive effects on cognition and immune development in early life [27333435]. Notwithstanding the uncertainty surrounding the optimal balance of the AA:DHA ratio [32], this ratio could be important because it might contribute to LCPUFA deposition in the growing brain during the critical period of growth and development in infancy [27]. What has been demonstrated to be important is the concomitant supply of DHA and AA in the formula, as excessive DHA may suppress the benefits provided by AA [83336]. Given the absence of evidential data, in the context of the aforementioned ratio in the EFSA report, the AA:DHA ratio in Korean toddlers (0.53) who are no longer receiving breast milk is less balanced when compared with consumption for toddlers in other countries - 2.84 in the US [4], 1.62 in China [24], and 1.23 in developing countries [31].
The limitations of our analysis should be noted. First, a 24-h dietary recall tool might be insufficient to assess the usual daily intake of nutrients, due to imperfect memory and day-to-day dietary variation. Nevertheless, well-trained dietitians collected dietary data in order to minimize possible estimation and reporting errors by exploiting stringent protocols and procedures. In addition, a mean of 1-day nutrient intakes among 1- to 3-year-old US children was reported, taking into account that the abovementioned mean estimate of the usual intake distribution in the population can be used without refined statistical analysis in the NHANES dietary data tutorial [37]. In 2009, the KNHANES also showed that variations between 1-day and 2-day 24-h dietary recall data were not significantly different (variations of 3.9%E and 3.8% fat) [38]. Second, comparisons between studies conducted in different countries are limited by the differences in methodologies used and survey sampling procedures. Additionally, we potentially underestimated the PUFA intakes since intake from dietary supplements was not included with the models used here and there may have be possible recall bias. Despite the challenges of dietary surveys in toddlers and the scarcity of validated age-appropriate instruments, this study has strength in its representativeness of dietary PUFA intakes among the Korean population. However, our study did not assess correlations between dietary n-3 and n-6 LCPUFA intakes and neurocognitive development. Further prospective studies are warranted to examine whether dietary intakes of DHA and AA throughout infancy and early childhood influence neurocognitive development in early life.
In conclusion, this study is the first to estimate PUFA intakes in a nationally representative sample of Korean toddlers 12–24 months of age. Our current observational findings show that toddlers in Korea are not meeting recommendations for n-3 and n-6 FA intakes. Dietary DHA intake is slightly higher than in other countries since Korea is a peninsula surrounded by sea on three sides, but toddlers are still not meeting recommendations. Although the optimal balance of DHA and AA intake during the first 1000 days of life remains unknown, the AA:DHA ratio in Korea toddlers is below the proposed ratio. Considering the importance of DHA and AA for early development, this dietary pattern may have negative consequences for optimal brain development. Strategies that increase consumption of DHA and AA need to be implemented. Given the scientific and legislative emphasis on the importance of DHA and AA, a combined approach of dietary supplementation, food fortification, and diversification of food sources, may need to be considered to ensure recommendations are being met.




 XML Download
XML Download