

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Myasthenia gravis (MG) is a chronic rare autoimmune disease characterized by severe muscle weakness and caused by the inhibition of neuromuscular transmission due to the binding of autoantibodies at the neuromuscular junction and subsequent complement-mediated destruction of the end-plate region. The prevalence of MG has been estimated as ranging from 107 to 278 per million.12345 MG often first manifests as weakness of ocular muscles (ocular MG), but approximately 70–80% of patients eventually manifest generalized disease that affects other muscles including in the face, neck, hand, and/or limb.6789 This generalized muscle weakness can lead to symptoms that include slurred speech, difficulty swallowing, extreme fatigue, and weakness of the upper and lower extremities, which together can have a considerable impact on the ability to perform the activities of daily living (ADL).101112 Reportedly, 15–20% of patients experience severe weakness of the respiratory muscles that can lead to life-threatening respiratory failure (myasthenic crisis) and result in the need for intubation and mechanical ventilation.1314
Acetylcholinesterase inhibitors, corticosteroids, or steroid-sparing immunosuppressive therapies (ISTs) are effective against most or all of the disease symptoms for many patients with MG.1516 However, approximately 15% of patients do not exhibit adequate symptom control or cannot tolerate these treatments, and are therefore considered to have refractory MG.17 The criteria that are frequently used to define refractory disease include 1) failure to respond to adequate doses of conventional therapies, 2) inability to reduce IST use without clinical relapse or a need for ongoing rescue therapy including plasma exchange (PLEX) or intravenous immunoglobulin G (IVIg), 3) severe and/or intolerable side effects to IST, 4) comorbid conditions restricting the use of conventional therapies, and 5) frequent myasthenic crises.1318 A large number of patients with refractory MG spend many years receiving a range of traditional treatments in attempts to achieve disease control, before progressing to more-intensive treatments including chronic IVIg or PLEX.16 The health-related quality of life of patients with MG is negatively impacted when adequate symptom control cannot be achieved and by the possible burden of MG-treatment side effects.1920
In light of the persistent clinical burden experienced by patients with refractory MG as a result of poor symptom control and increased risk of MG exacerbations, it is reasonable to assume that patients with refractory MG use more healthcare resources than those with nonrefractory disease. Data from a United States (US) claims database have shown that compared with those with nonrefractory MG, patients with refractory MG who experience more myasthenic exacerbations (including crises) visit the emergency room (ER) more often and have more inpatient hospitalizations.21 Similar findings have been reported for a Japanese study analyzing anonymized patient health records.22
The present study used patient-reported data to further examine the impact of refractory MG on healthcare resource utilization (HRU) in the USA and to corroborate the findings reported based on US claims data.
METHODS
Data source
The Myasthenia Gravis Foundation of America (MGFA) Patient Registry is an active database of individuals with MG that has been developed for use in research and treatment development. This registry is open to adults who are ≥18 years of age and living in the USA. Participants enter the registry by completing an online enrollment survey that comprises approximately 200 questions covering categories including participant demographics, MG history, comorbidities, past and current therapies, family history of MG, functional status [assessed using the myasthenia gravis activities of daily living scale (MG-ADL)], lifestyle, and HRU. The MG-ADL is a validated eight-item, participant-reported outcome measure that was developed to assess MG symptoms and their functional impact; the MG-ADL total score ranges from 0 to 24, with a higher score indicating worse impact on ADL.1023
The present study included data from enrollment surveys completed between July 2013 (when the MGFA Patient Registry was instigated) and February 2018. Participants receive a shorter online survey to complete every 6 months after enrollment, but no data from these post enrollment surveys were included in the present study. Data were de-identified for research use, and consent for participation was provided by participants electronically at registration before they completed the enrollment survey. The study was approved by the Institutional Review Board of the University of Alabama at Birmingham, Birmingham, AL, USA (IRB No. 130401004).
Participants
Participants in the MGFA Patient Registry were included in this study if they were aged ≥18 years and <65 years. This age restriction was applied in order to minimize the impact on HRU of comorbidities and mortality that may be experienced by individuals aged ≥65 years. Moreover, US residents aged ≥65 years are eligible for Medicare, a government-funded hospital insurance cover, which may increase the number of times these individuals visit a healthcare establishment for MG-related treatment.
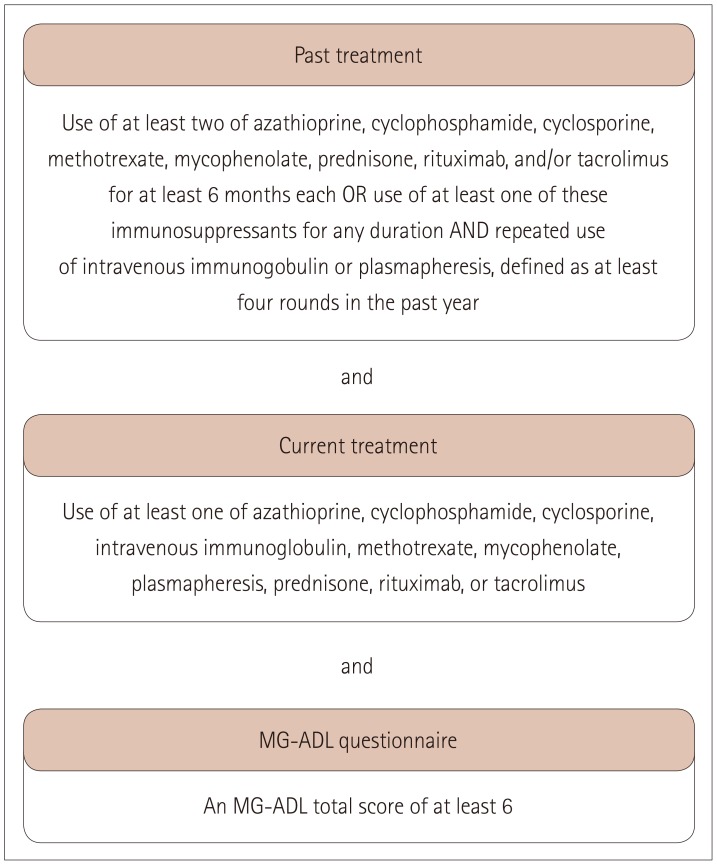
Participants were included in this study if they reported having been diagnosed by their doctor as having MG for ≥2 years before completing the enrollment survey. This time requirement was used to ensure that adequate time had elapsed between the diagnosis of MG and inclusion in the study for the presence of refractory disease (defined as no or inadequate response to therapy) to be determined. Participants were classified as having refractory MG based on their MG treatment history [previous use of at least two ISTs (azathioprine, cyclophosphamide, cyclosporine, methotrexate, mycophenolate, prednisone, rituximab, and/or tacrolimus) for at least 6 months each, or previous use of at least one of these ISTs for any duration and repeated use of IVIg or PLEX (at least four rounds in the previous year)], current use of at least one MG treatment, and having an MG-ADL total score of at least 6 (Fig. 1). Participants who did not meet the previous or current treatment criteria for refractory MG were considered to have nonrefractory MG regardless of their MG-ADL score. Participants for whom there were no data available to enable classification as refractory or nonrefractory were excluded from this analysis.
Study measures
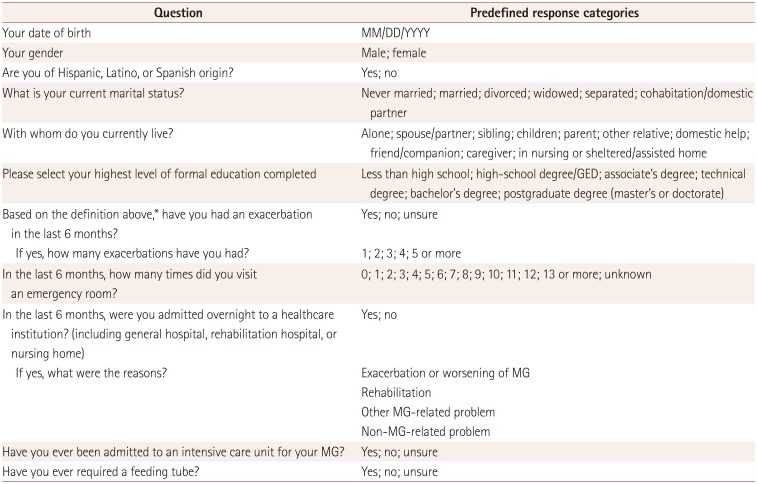
The primary outcome measures were the proportions of participants who had experienced at least one exacerbation, visited an ER at least once, and/or been hospitalized overnight at least once during the 6 months before enrollment, and the proportions who had ever been admitted to an intensive care unit (ICU) for reasons related to MG and/or required a feeding tube. The numbers of MG exacerbations and ER visits during the 6 months before enrollment were also recorded. The numbers of exacerbations and ER visits were each categorized into 0–3 and ≥4 in order to distinguish between lower and higher disease burdens. The enrollment survey defined an exacerbation of MG as the development of new symptoms or the worsening of existing symptoms that lasted >7 days and occurred ≥30 days after the last exacerbation. Other variables of interest due to their potential association with HRU included age, gender, ethnicity, living arrangement, marital status, and education level. The questions relating to the demographic and HRU data extracted for this study are listed in Table 1.
Statistical analyses
Summary statistics were calculated for all study variables. Bivariate analyses were used to compare demographic, exacerbation, and HRU data for the refractory- and nonrefractory-MG groups and to compare exacerbation and HRU data between younger and older female participants with refractory MG. χ2 tests (or Fisher's exact tests for small samples) were used for categorical variables, and t-tests were used for continuous variables.
Based on the median age of the study population (51 years), participants were classified as being younger if they were aged <51 years and older if they were aged ≥51 years. Analyses were based on fitting a logistic model for binary outcomes, except when analyzing the numbers of exacerbations and ER visits, for which proportional-odds models for ordinal outcomes were fitted. Unadjusted and adjusted models were fitted to examine the effects of covariates on the association between refractory status and the exacerbation and HRU outcomes. The covariates included were the living arrangement, marital status, age (with 51 years as the cutoff), gender, ethnicity, and education level. Subgroup analyses by age within the refractory group were applied to female participants only, since an equivalent subgroup analysis with male participants only was not possible due to the small number of males with refractory disease (n=10). No unknown or missing-value categories for any of the outcomes were included in the statistical analyses. Probability values of p<0.05 were deemed significant. Analyses were performed using SAS® (version 9.4, SAS Institute, Cary, NC, USA).
RESULTS
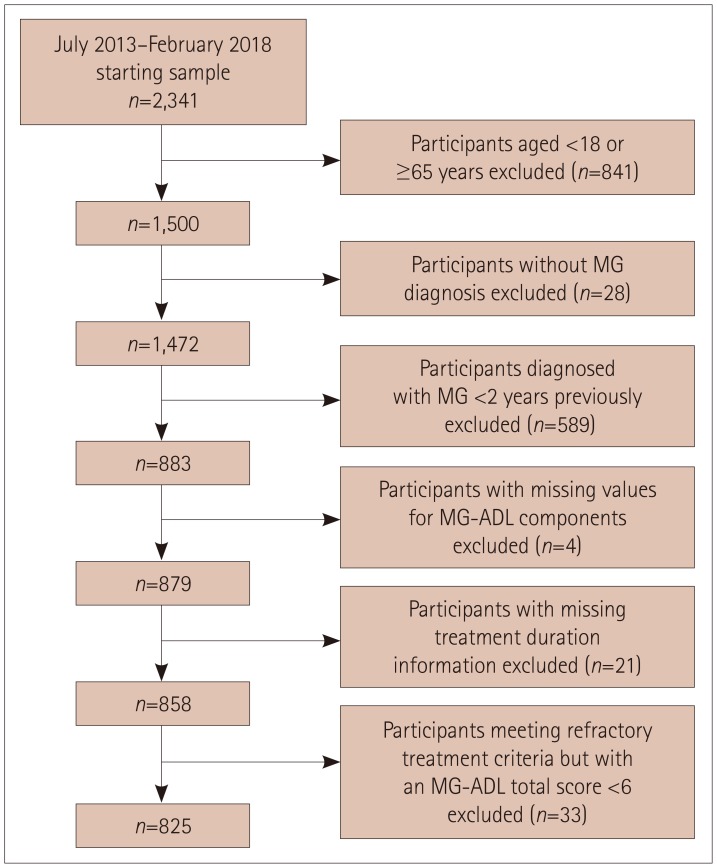
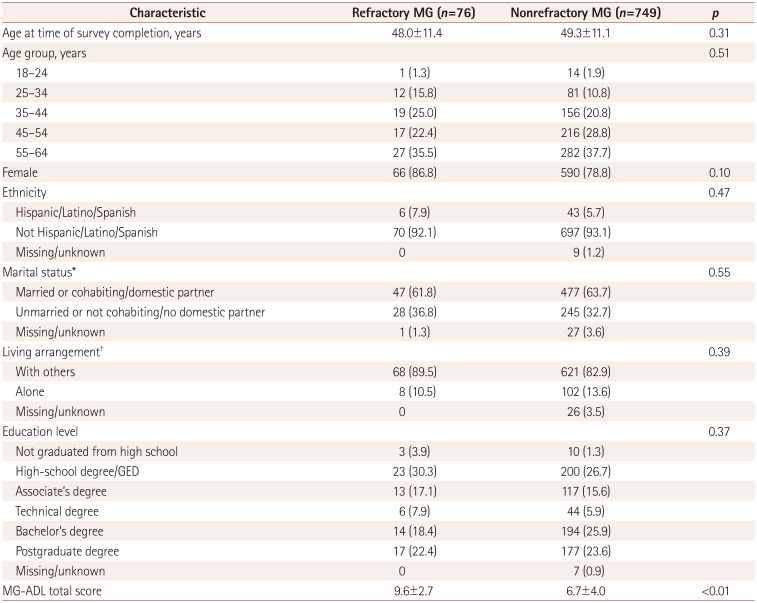
The flow of participants through the sample selection process is summarized in Fig. 2. The 2,341 participants in the MGFA Patient Registry included 825 participants who met the inclusion criteria of this study: 76 (9.2%) were classified as having refractory MG based on the criteria defined for this study, and 749 participants (90.8%) were classified as having nonrefractory MG (Table 2). The bivariate analyses revealed no statistically significant differences between the refractory and nonrefractory groups with regard to demographic data including age and gender (Table 2).
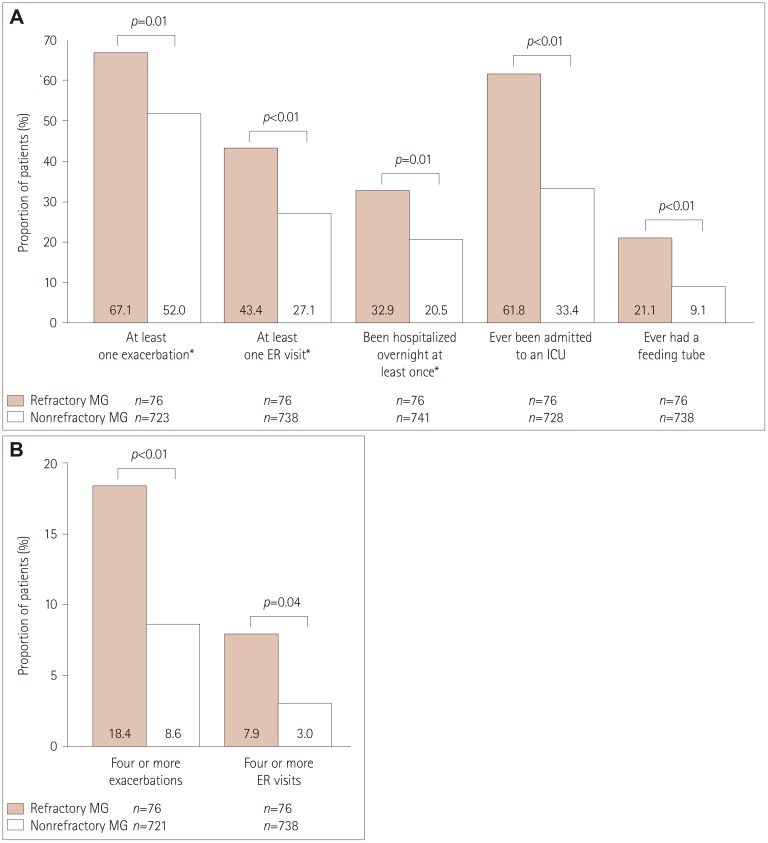
The bivariate analyses revealed statistically significant associations between refractory MG and the outcomes for exacerbations and HRU. During the 6 months before enrollment, a significantly higher proportion of participants with refractory MG than those with nonrefractory MG had experienced at least one MG exacerbation, had visited an ER at least once, or had been hospitalized at least once (Fig. 3A). Furthermore, a higher proportion of participants with refractory MG than those with nonrefractory MG had experienced at least four exacerbations or had visited an ER at least four times (Fig. 3B). Compared with participants with nonrefractory MG, a significantly higher proportion of participants with refractory MG had been admitted to an ICU at any time for reasons associated with MG or had previously required a feeding tube (Fig. 3A).
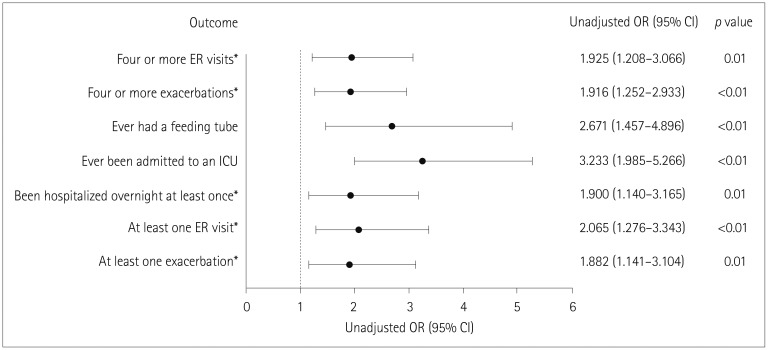
Unadjusted regression analyses confirmed that participants with refractory MG were significantly more likely than those with nonrefractory MG to have experienced at least one MG exacerbation, visited an ER at least once, been hospitalized at least once, been admitted to an ICU at any time for reasons associated with MG, or previously required a feeding tube (Fig. 4). Similarly, compared with participants with nonrefractory MG, participants with refractory MG were significantly more likely to have experienced at least four exacerbations or had visited an ER at least four times (Fig. 4). After adjusting for other demographic variables such as age, gender, ethnicity, marital status, and education level, the estimated odds ratios were similar to the unadjusted odds ratios across all outcome measures (data not shown).
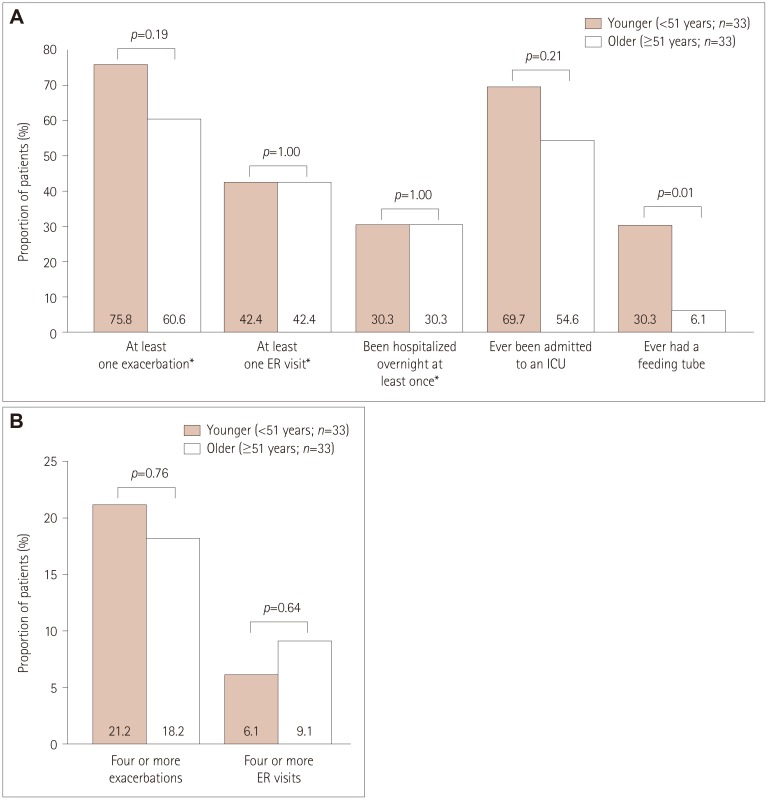
Among the 66 female participants with refractory MG, a significantly higher proportion of the younger ones (n=33) than older ones (n=33) had previously required a feeding tube (Fig. 5A). A total of 75.8% of younger female participants with refractory disease experienced at least one exacerbation and 69.7% had experienced an ICU admission (Fig. 5A). For older female participants with refractory disease, 60.6% and 54.6% had experienced at least one exacerbation or ICU admission, respectively (Fig. 5A). Just over a fifth of younger female participants (21.2%) experienced at least four exacerbations and 6.1% visited an ER at least four times (Fig. 5B). For older female participants, 18.2% experienced at least four exacerbations and 9.1% visited an ER at least four times (Fig. 5B). The between-group differences were not significant (Fig. 5).
DISCUSSION
This study was designed to examine the impact of refractory MG compared with nonrefractory MG on the number of exacerbations and HRU in the USA using patient-reported data extracted from the MGFA Patient Registry. Our findings from the bivariate and unadjusted regression analyses support the hypothesis that patients with refractory MG have more exacerbations and utilize more healthcare resources than those with nonrefractory MG.
There is currently no widely accepted definition of refractory MG.18 In the present study we considered a patient to have refractory MG if they experienced persistent symptoms after receiving at least two ISTs or at least one IST and repeated use of IVIg or PLEX in the past, and were currently receiving treatment and still had an MG-ADL total score of at least 6 (Fig. 1). This conservative definition is similar to those used in other studies.1824
Participants with refractory MG accounted for 9.2% of the individuals in this study, which is similar to the proportions included in other studies.1721 The participant demographics, including age and gender, were not significantly different between the refractory and nonrefractory MG groups. The high proportion of females in the study population (80%) may have resulted from excluding participants aged ≥65 years, because females have an earlier mean age at MG onset625 and so they will constitute a higher proportion of a young population than males.
Considering the study population as a whole, over half of the participants (53.4%) reported experiencing an exacerbation and almost one-third (28.6%) had visited an ER at least once during the 6 months before enrollment. The findings of this study highlight not only the burden of disease experienced by patients with refractory MG, but also the impact of MG on patients with nonrefractory MG. The current study corroborates the findings of previous studies that examined the impact of refractory MG on HRU based on claims databases and patient health records.2122 The present study found that more participants with MG refractory to conventional therapies had experienced exacerbations, ER visits, and overnight hospitalizations during the 6 months before enrollment. Additionally, participants with refractory-MG were more likely than those with nonrefractory MG to have ever been admitted to an ICU for reasons associated with MG, or to have required a feeding tube.
MG is associated with an increased risk of comorbidities including dysthyroidism, dyslipidemia, diabetes mellitus, and other autoimmune diseases (e.g., autoimmune thyroiditis, systemic lupus erythematosus, and rheumatoid arthritis), and the presence of a comorbid disease has been associated with more-frequent myasthenic crises and ER visits.262728 It might be expected that the occurrence of comorbidities—and therefore HRU—would increase with age. In the present study, the proportions of younger and older female participants with refractory MG who visited an ER at least four times were 6.1% and 9.1% respectively (p=0.64), although it should be noted that this result was not statistically significant and that participants in this study were aged <65 years. A total of 75.8% of younger female participants with refractory disease experienced at least one exacerbation, and 69.7% had experienced an ICU admission. For older female participants with refractory disease, 60.6% and 54.6% had experienced at least one exacerbation or ICU admission, respectively (between-group differences were not significant; p=0.19 and p=0.21, respectively). A significantly higher proportion of younger female participants had ever required a feeding tube (30.3% vs. 6.1%; p=0.01). In addition to age, gender has previously been shown to impact the clinical course of MG.625 However, the small number of male participants with refractory MG in this study made it impossible to analyze the effect of age on HRU in males with MG.
This study did not examine the costs associated with treating MG, or the cost implications of refractory MG compared with nonrefractory MG. A US medical claims database review of 1,288 patients with MG found that the cost of treating MG was much higher than the cost of treating diseases such as multiple sclerosis, migraine, and Alzheimer's disease.29 Although further research is needed into the difference in the costs of treating refractory and nonrefractory MG, the increased HRU of patients with refractory MG suggests higher associated costs.
Some limitations of the present analyses should be noted. The data collected in the MGFA Patient Registry are self-reported, and clinical diagnoses and documented therapies were not confirmed by a healthcare professional. Some participants with uncontrolled MG might not have met all of the study-specific criteria for having refractory disease. The inclusion of such participants in the nonrefractory-MG group would have reduced the magnitude of differences observed between the refractory- and nonrefractory-MG groups. Conversely, we acknowledge that some of the participants who met the criteria for refractory disease had uncontrolled disease for reasons such as inadequate treatment dose, short time receiving their current treatment, or poor treatment compliance.
Participants enrolled in the MGFA Patient Registry might constitute a self-selected sample of participants with MG who are more inclined to seek medical information, or who have a higher education level, higher socioeconomic status, and better Internet access, thereby facilitating their participation. This may be reflected in the characteristics of the participants in the MGFA Patient Registry, notably the high proportion of females, who are in general more likely than males to access healthcare,30 and the differing ethnicity distribution compared with the general MG population in the USA. It is also possible that patients with refractory MG are more motivated to participate in the registry, which may have resulted in the proportion of participants with refractory disease in this study being higher than that in the general MG population. Such self-selection may reduce the generalizability of these findings to the wider MG population.
Participants were asked to provide the total number of times that they had visited an ER during the 6 months before enrollment, with no instruction to include only ER visits for reasons relating to their MG. In addition, participants were given the option to select the reason for any overnight hospitalizations, which included exacerbation or worsening of MG, rehabilitation, other MG-related problem, or non-MG-related problems. The inclusion of ER visits and overnight hospitalizations not related to MG might confound the analyses. Although only exacerbations, ER visits, and overnight hospitalizations that had occurred during the 6 months before enrollment were recorded, no time restriction was applied to the history of ICU admission or feeding-tube requirement in the enrollment survey. Future studies should investigate all HRU using the same time frame. Because data regarding age in the refractory group were limited to female participants aged <65 years, these analyses might not be generalizable to the wider population of patients with refractory MG. However, this study builds on the growing evidence that patients with refractory MG suffer from a higher disease burden and negative impacts on their daily lives than patients with nonrefractory MG. Further research is required to assess the cost implications of increased HRU due to refractory MG.
In conclusion, this analysis of US participants in the MGFA Patient Registry has highlighted the burden of MG on both patients with refractory and patients with nonrefractory disease. More specifically, this study found that participants with MG that is refractory to traditional therapies experience more disease-related morbidities—which are associated with higher levels of HRU—than participants with nonrefractory MG. There remains a need for therapies that are effective against refractory MG, improve outcomes, and reduce the HRU by these patients.
 XML Download
XML Download