

 Citation
Citation Print
Print



INTRODUCTION
The comorbidity of panic disorder (PD) and major depressive disorder (MDD) is common in both clinical and general settings.12 According to a previous study,2 55.6% of patients with PD and 11.2% of those with MDD experience the other disorder in their life. Although this comorbidity is very prevalent, few researchers and clinicians have pay attention to this. Moreover, we may not consider the association of them since the symptomatic and biological profiles of these two disorders are quite different.34 However, the association between them is much stronger than any other comorbidities of psychiatirc disorders.15 In a recent study, 98% patients with PD had one or more lifetime comorbidities and MDD was also the most common comorbidity.6 Despite this strong relevance, clinicians may not be aware of this comorbidity due to the different symptom profiles and the lack of information about this comorbidity. Furthermore, in this context this common comorbidity can remain untreated, which result in serious consequences such as hospitalization and suicide.78 Patients with comorbidities of MDD and PD have poorer outcomes and higher suicidality than those with one of these conditions.291011 Therefore, it is crucial to focus on and understand the pattern of the co-occurrence of these disorders, which may facilitate the detection and management of this complicated condition in clinical settings.
Both PD and MDD may be present simultaneously or their onset may occur at a time interval. There are three possibilities of the occurrence of these comorbidities in a lifetime: first, PD precedes MDD; second, MDD precedes PD; third, PD and MDD are simultaneously present. Several studies have focused on a temporal priority between anxiety disorder and depressive disorder with respect to their onset order. The results revealed that anxiety disorder developed before depressive disorder.1213 Similar results were observed in case of PD and MDD.8 The results of these studies have reported unidirectionality in the comorbidity of anxiety and depressive disorders. However, in actual clinical settings, an opposite directionality has been reported.28 Notably, the most recent meta-analysis has suggested bidirectional associations between anxiety disorder and depressive disorders, except for social and specific phobia and depressive disorder.14 In addition to the above directionality, the pattern of intensity of the occurrence can be analyzed with respect to the time point. A previous study has shown that the risk of comorbidity is the highest in the same year and decreases over time.8
In this study, we analyze the association between PD and MDD, with respect to the time interval, and verify the bidirectionality. First, we will examine the cumulative occurrence of MDD and PD, depending on the presence or absence of the other disease. Second, the hazard ratios (HRs) of the occurrence of PD or MDD was calculated by the time interval after the other disorder developed first. While most of previous studies have only focused on comorbidity rate and temporal priority, we try to find a clinical implication by focusing on time lag of first onset between PD and MDD. In particular, our study has strengths in that we analyzed the comorbidity between PD and MDD for the first time in Asian.
METHODS
We extracted data from three nationwide epidemiological surveys: Korean Epidemiologic Catchment Area study (KECA),15 Korean Epidemiologic Catchment Area study replication (KECA-R),16 and 2011 Korean Epidemiologic Catchment Area study (KECA-2011).17 These three surveys investigated the prevalence of psychiatric disorders based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) in Korean adults aged 18 years and older. Each survey was conducted with the same design, but the sample of each was independent. Subjects were selected by multistage, cluster sampling of 18,807 adults across 12 catchment areas (6,275 in KECA; 6,510 in KECA-R; and 6,022 in KECA-2011). The subjects were interviewed using a full-structured diagnostic tool, the Korean version of the Composite International Diagnostic Interview (K-CIDI).1819 Data were pooled from all three surveys, and the respondents diagnosed with the onset of MDD and PD were examined.
KECA, KECA-R, and KECA-2011 diagnosed MDD and PD according to the mood and anxiety sections in the K-CIDI. In these sections, the subjects were retrospectively asked about the age of onset (AOO) according to the K-CIDI question series. The retrospective diagnostic AOO report in the CIDI has a limitation of acceptability, but revealed a good test-retest reliability.20
Statistical analysis
SAS Version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA) was used to complete all analyses. Survey weights were calculated for the participants and were used to adjust the data to approximate the national age and gender distributions according to the Statistics Korea census. We used the Kaplan-Meier method to estimate separate survival functions, using the AOO of MDD and PD as the outcome. For the survival analysis, in which MDD/PD was the outcome, the AOO of MDD/PD was the endpoint for patients who experienced an episode of MDD/PD. If the respondents did not report an episode of MDD/PD, that observation was considered censored and the age of the respondent at the time of interview was considered the endpoint. To understand the temporal effects of previous disorders, we used a Cox proportional hazard model to estimate HRs for the onset of MDD/PD with the comorbid disorder as a time-dependent covariate, after adjustment by previous onsets of all other disorders in CIDI except nicotine use disorder, alcohol use disorder, eating disorder, obsessive-compulsive disorder, post-traumatic stress disorder, psychotic disorder, bipolar disorder, dysthymic disorder, social phobia, generalized anxiety disorder, and specific phobia. A two-sided P-value of ≤ 0.05 was considered statistically significant.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of Seoul National University College of Medicine (IRB No. for KECA, C-0602-041-168; KECA-R, C-0607-009-177; and KECA-2011, C-1104-092-359). All subjects were fully informed about the aims and methods of the study, and they submitted written informed consent prior to participation.
RESULTS
Demographic and clinical characteristics of subjects
Sociodemographic and clinical characteristics of the subjects are summarized in Table 1 and Fig. 1. Among the 18,807 respondents, 1,415 and 118 were diagnosed as having at least one episode of MDD and PD, respectively. The lifetime prevalence of MDD and PD was 7.0% and 0.6%, respectively; the prevalence of these comorbidities was 0.3%.
Table 1
Sociodemographic characteristics and lifetime prevalence of PD and MDD in the participants (n = 18,807)

Effects of PD on the subsequent first onset of MDD
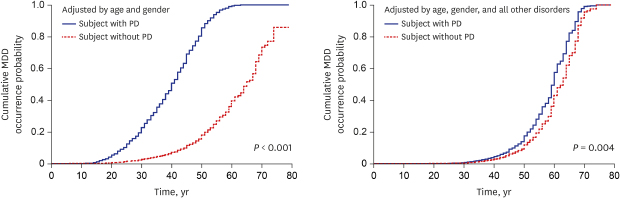
PD was significantly associated with the onset of MDD after adjustment for gender and age (P < 0.001) (Fig. 2). PD increased the risk of the subsequent onset of MDD (HR, 9.638; 95% confidence interval [CI], 7.203–12.896) (Table 2). Considering the time interval after the first onset of PD, the HR was the highest in the same year, and then gradually decreased (HR in the same year, 19.244, P < 0.001; HR at 1–2 years, 12.680, P < 0.001; and HR at 3–5 years, 4.439, P = 0.001). The effect was not significant at 6–10 years (HR, 2.699; P = 0.091), and it became significant again after 11 years (HR, 7.156; P < 0.001) (Table 2). After adjustment by the onset of all other disorders, the overall HR changed to 1.518 (95% CI, 1.147–2.009; P = 0.004) and the effects of panic disorder were only valid for up to 2 years (HR in the same year, 1.626; P = 0.035 and HR at 1–2 years, 2.248; P = 0.015).
Fig. 2
Cumulative occurrence of MDD over time in patients with and without PD (adjusted by age and gender).
All other disorders: alcohol use disorder, eating disorder, obsessive-compulsive disorder, post-traumatic stress disorder, psychotic disorder, bipolar disorder, dysthymic disorder, social phobia, generalized anxiety disorder, specific phobia.
PD = panic disorder, MDD = major depressive disorder.

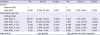
Table 2
HRs for the risk of MDD associated with PD
All other disorders: alcohol use disorder, eating disorder, obsessive-compulsive disorder, post-traumatic stress disorder, psychotic disorder, bipolar disorder, dysthymic disorder, social phobia, generalized anxiety disorder, specific phobia.
HR = hazard ratio, CI = confidence interval, MDD = major depressive disorder, PD = panic disorder.
Effects of MDD on the subsequent first onset of PD
MDD was significantly associated with the onset of PD after adjustment for gender and age (P < 0.001) (Fig. 3). MDD increased the risk of the subsequent onset of PD (HR, 14.728; 95% CI, 9.494–22.849) (Table 3). Considering the time interval after the first onset of MDD, the HR was the highest in the same year, and then gradually decreased (HR in the same year, 60.473, P < 0.001; HR at 1–2 years, 35.133, P < 0.001; HR at 3–5 years, 3.758, P = 0.014). The impact was only significant for up to 5 years, and thereafter was not statistically significant (Table 3). After adjustment by the onset of all other disorders, the overall HR changed to 3.872 (95% CI, 2.361–6.349; P < 0.001) and the effects of panic disorder was significant for up to 2 years (HR in the same year, 4.339; P < 0.001 and HR at 1–2 years, 7.758; P < 0.001, respectively).
Fig. 3
Cumulative occurrence of PD over time in patients with and without MDD (adjusted by age and gender).
All other disorders: alcohol use disorder, eating disorder, obsessive-compulsive disorder, post-traumatic stress disorder, psychotic disorder, bipolar disorder, dysthymic disorder, social phobia, generalized anxiety disorder, specific phobia.
PD = panic disorder, MDD = major depressive disorder.
Table 3
HRs for risk of PD associated with MDD
All other disorders: alcohol use disorder, eating disorder, obsessive-compulsive disorder, post-traumatic stress disorder, psychotic disorder, bipolar disorder, dysthymic disorder, social phobia, generalized anxiety disorder, specific phobia.
HR = hazard ratio, CI = confidence interval, MDD = major depressive disorder, PD = panic disorder.
DISCUSSION
The findings of the present study revealed that PD was significantly associated with an elevated risk of subsequent MDD. PD elevated the risk of subsequent MDD by 9.6-fold; after adjustment for the previous onset of all other disorders, this risk was reduced to 1.5-fold, but was still statistically significant. Previous studies have only shown that PD increased the risk of subsequent MDD, whereas our results show additional evidence that MDD increased the risk of subsequent PD. MDD elevated the risk of subsequent PD by 14.7-fold. After adjustment for the previous onset of all other disorders, the risk was decreased to 3.8-fold. The reasons for this difference in finding cannot apparently be explained in this study, but we may consider culture and ethnicity as influencing factors. Notably, the patterns of disease occurrence and prevalence rate of MDD and PD vary according to race, ethnicity, and country; their prevalence was actually lower in Asian countries than in Western countries.1521222324 Therefore, further research is needed to explain the difference in our results compared with those of previous studies. Nevertheless, in actual clinical settings, we could meet a substantial number of patients with PD having a previous history of depression. In addition, this type of patients have existed even in several studies that did not statistically present the directionality from MDD to PD. Therefore, it seems necessary to focus on this directional relationship. In fact, there have been studies showed the association between PD and MDD. Stein and Uhde25 argued that PD and MDD are non- identical disorders with a lot of neurobiological similarities. PD and MDD have several shared risk factors such as the exposure to childhood abuse2627 and information-processing bias.2829 Cox et al.30 showed that negative affectivity, neuroticism, low positive affect and anxious arousal could be worked as shared risk factors between PD and MDD based on the tripartite model. As an extension of this study, large-scale genetics studies were conducted afterward and found that PD and MDD shared genetic variation which was related with personality trait of neuroticism.3132 Although there have been studies supporting the bidirectional association, it is still difficult to confirm the pathogenesis of association between PD and MDD since the precise pathophysiology of each disorders are not even understood fully. These shared factors can be considered as acceptable to explain the comorbidity in that they make individuals vulnerable to stress or many psychopathologies. However, further and well-designed researches are needed on this issue because these may also be risk factors for other psychiatric disorders. To our knowledge, this study is the first to reveal the bidirectional relationship between MDD and PD by analyzing large epidemiological data.
The HR was higher for the effect of MDD on PD (HR, 3.872; P < 0.001) than for that of PD on MDD (HR, 1.518; P = 0.004). In other words, the strength of directionality from MDD to PD is stronger than the opposite. This result is not only different from those of previous research that MDD did not affect the occurrence of PD8 and also considerably challenging. However, we believe that these results reflect a more clinical reality and are consistent with those of the most recent study.14 Jacobson and Newman14 show that the odds ratio of depressive disorder predicting panic disorder was higher than the odds ratio of panic disorder predicting depressive disorder (6.126; 95% CI, 1.168–32.119 and 4.597; 95% CI, 3.026–6.982, respectively). Although it is not available to explain the different outcomes in detail at this stage of research, these new findings may represent the importance of the directionality of MDD to PD and suggest future clinical applications.
We also analyzed the HRs with respect to the time period. The impact of PD on MDD was most likely to occur in the same year and gradually decreased over 5 years. After that, it became nonsignificant from 6 to 10 years and increased again after 11 years. After adjustment for the previous onset of all other disorders, it only showed an effect up to 2 years of onset. This result is similar to that of a previous community-based study conducted in the United States.8 This study showed that the effect of PD on MDD was only relevant in the same year; however, our result revealed the effect to continue in the following year. Although there were differences between these two studies, with respect to race, sampling time, and adjustment factors, the HRs were similar (2.3 in the same year, United States; 1.518 in the same year and 2.248 in the following year, Korea).
The impact of MDD on PD was the strongest in the same year, gradually decreased over 5 years, and became nonsignificant thereafter. However, this result was changed after adjustment for the previous onset of all other disorders. The significant effect lasted for up to 2 years, similar to the effect of PD on MDD. The HR of 4.339 in the same year increased to 7.758 in the next year. This result suggests that careful observation is needed because when PD or MDD occurs, the other disorder may develop within 2 years.
In addition, we must emphasize the fact that HR are substantially decreased after adjustment by the previous onset of all other disorders, indicating that as other comorbidities exist, the duration of close monitoring may need to be suspended. Because this study focused on the association between MDD and PD, we did not show how each specific comorbidity influences the change in HR. In the analysis, alcohol use disorder, mania, and anxiety disorders were found to have significant effects on the change in HRs. Indeed, these disorders are established to be associated with MDD and PD.33343536 In the real world, MDD and PD are likely to have other anxiety disorder, mania, and alcohol use disorder as comorbid disorders. Therefore, when PD or MDD occurs, it may be necessary to monitor the other disorder for more than 2 years.
Our research findings have clinically significant implications in the treatment of MDD and PD. Although MDD and PD are very prevalent in clinical settings, it had not been usual to consider that PD and MDD are interrelated and can predict each other for a considerable duration. Understanding the pattern of co-occurrence of these two disorders can facilitate early-recognition and consequently, apply appropriate treatment immediately or prevent clinically significant symptoms.
This study has some limitations. First, the AOO of the disorders was retrospectively recorded, which may have caused recall bias. Second, the presence of non-respondents may have influenced the prevalence data and results, because in case of mental disorders, the rate of non-respondents could be higher than that of respondents.3738 With respect to non-respondents, cultural effects must also be considered. In fact, Asian countries have a lower prevalence of MDD and PD than do Western countries and it might be attributed to the difference in the symptom threshold and patterns.39
In conclusion, MDD and PD have a bidirectional association. Each disease represents a risk of the subsequent occurrence of the other disease for a considerable period of time. Therefore, we must be aware that one of these diseases can lead to the other and must consider this for the management of patients with MDD or PD.
 XML Download
XML Download