

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neisseria meningitidis is a leading cause of bacterial meningitis and sepsis worldwide.12 Permanent disability or death can occur within a few hours of symptom onset, and associated morbidity and mortality rates remain high.3 An estimated 500,000 annual cases of meningococcal disease occur worldwide with a case fatality rate of 10%–15%.4 The greatest burden of meningococcal disease occurs between the ages of 6 months and 2 years, but a second peak occurs among adolescents and young adults.2
Invasive meningococcal diseases are most commonly caused by serogroups A, B, C, W-135, and Y worldwide.5 Vaccines can offer protective immunity against these diseases, and therefore, various vaccines from killed whole cells to polysaccharide and conjugate vaccines have been developed. Further, meningococcal polysaccharide vaccines are being replaced by conjugate vaccines because of the immunologic superiority of the latter.
Quadrivalent (A, C, W-135, Y) meningococcal conjugate vaccines (MenACWY) have also been developed using various carrier proteins such as diphtheria toxoid (DT), a nontoxic mutant of diphtheria toxin (cross reactive material 197 [CRM]), and tetanus toxoid. The latter two vaccines were licensed through non-inferiority comparative immunogenicity studies with previous vaccines.678 In Korea, two quadrivalent meningococcal conjugate vaccines (CRM and DT) are available, and both are included in the national immunization program for military recruits.9 However, there have been no comparative immunogenicity studies for these vaccines in Korea.
Therefore, we performed an immunogenicity study using two licensed vaccines (MenACWY-CRM vs. MenACWY-DT) in healthy Korean adults.
METHODS
Study design and subjects
This study was conducted with healthy subjects 20 to 50 years of age to evaluate the immunogenicity and safety of two licensed meningococcal conjugated vaccines in Korea. The clinical trial registration number is KCT 0002460 (CRIS, https://cris.nih.go.kr/cris/en/).
Healthy subjects 20 to 50 years of age were eligible for inclusion in the study. Subject exclusion criteria included previous vaccination with a meningococcal vaccine, history of N. meningitidis infection, receipt of immunosuppressant or steroid within a period of 1 month prior to enrollment, receipt of immunoglobulin or blood products within the 3 previous months or planned administration during the study period, or serious acute or chronic illness. Because the meningococcal immunization program was introduced among military recruits in Korea since 2012, men who joined military service after 2012 were considered to be vaccinated and were also excluded from this study.
Subjects were randomly allocated 1:1 into one of two groups (MenACWY-DT or MenACWY-CRM). Participants were randomly assigned to one of two vaccine groups following a randomization sequence created using Stata 10.0 (StataCorp, College Station, TX, USA) statistical software with a 1:1 allocation using random block sizes of 2, 4, and 6.
MenACWY-DT contained 4 µg of capsular polysaccharide from each serogroup (A, C, W-135, and Y) covalently bound to DT protein in each 0.5 mL dose. Each dose of MenACWY-CRM consisted of two components as follows: one component contained 10 µg of lyophilized meningococcal serogroup A capsular polysaccharide conjugated to CRM197 (MenA) and the other contained 5 µg each of capsular polysaccharide of serogroups C, W-135, and Y conjugated with CRM197 in 0.5 mL of phosphate-buffered saline, which was used to reconstitute the lyophilized MenA component before injection. All subjects received a single dose (0.5 mL) of vaccine administered intramuscularly in the deltoid area. Subjects were observed for 30 minutes post-vaccination for any local or systemic reactions or for hypersensitivity reactions.
Blood samples were obtained before and 1 month after vaccination (range, 21–50 days). We confirmed that each subject was not taking antibiotics within 7 days before sampling.
Serum bactericidal assay to assess immunogenicity
Serum bactericidal assays using baby rabbit complement (rSBAs) were performed for four meningococcal serogroups (A, C, W-135, and Y) at the Ewha Center for Vaccine Evaluation and Study as recommended by the World Health Organization in the standardized assay.1011 The target strains used for the rSBAs were ATCC13077 for serogroup A, C11 for serogroup C, MOI-240070 for serogroup W-135, and S-1975 for serogroup Y. ATCC13077 was purchased from American Type Culture Collection (ATCC; Rockville, MD, USA) and MOI-240070 was purchased from National Collection of Type Cultures (Public Health England, Salisbury, UK). C11 was gifted by GlaxoSmithKline Biologicals (Rixensart, Belgium) and Novartis Vaccines and Diagnostics (Cambridge, MA, USA). S-1975 was kindly provided by the US Food and Drug Administration (Silver Spring, MD, USA).
All rSBA steps were performed in a class II biosafety cabinet. A frozen aliquot of N. meningitidis strain from each serogroup was thawed and diluted in HBSS-HS (Hanks thawed and diluted in Hank's Balanced Salt Solution [HBSS; Gibco, Carlsbad, CA, USA] containing 1% horse serum [HyClone, Logan, UT, USA]) to yield 800–1,000 CFUs in 20 µL of solution. Duplicate serum samples were serially diluted three-fold with buffer in 96-well U-bottom microtiter plates. Twenty microliters of meningococcal suspension was then added to serially-diluted serum. After 2 minutes of incubation at 25°C with shaking at 700 rpm, 20 µL of baby rabbit complement (Pelfreeze, Brown Deer, WI, USA) was added to each well. Plates were incubated for 90 minutes (serogroup A) or 60 minutes (serogroup C, W-135, and Y) in a tissue culture incubator (37°C, 5% CO2) with shaking at 700 rpm. After stopping the reaction by placing the plates on ice for 15 minutes, 10 µL of the final reaction mixture was spotted onto 1.5% of Brain-Heart-Infusion (BHI; Becton Dickinson and Company, Sparks, MD, USA) agar plates with 5% horse serum. After the fluid was absorbed into the agar, each plate was overlaid with molten BHI agar (0.75%) containing 5% horse serum and 2,3,5-triphenyltetrazolium chloride (Sigma, St. Louis, MO, USA). The plates were then incubated at 37°C in a 5% CO2 incubator. Surviving bacterial colonies in the plates were counted using colony counting software, National Institute of Standards and Technology, US's Integrated Colony Enumerator (Gaithersburg, MD, USA). The bactericidal index was defined as the serum dilution that killed 50% of the bacteria, which was determined by linear interpolation. For computational purposes, an rSBA index (rSBI) lower than the serum starting dilution of 8 was assigned a value of 4.
Correlates of protection
An rSBI value ≥ 8 was used for correlates of protection measurements since it is the putative protective titer that was shown to predict short-term clinical protection against disease in the UK.12 The more discriminatory rSBI value of ≥ 128, which reliably predicts an serum bactericidal assays using human complement (hSBA) index ≥ 4,13 was also used.
Statistical analysis
The planned sample size of 27 evaluable participants per group was calculated to provide 80% overall power in order to demonstrate consistency of the immune response to the two vaccines assuming a two-sided α = 0.05.
Geometric mean indices (GMIs) were calculated and two-sided 95% confidence intervals (CIs) were determined for each meningococcal serogroup for both groups. The seroresponse rate was defined as the proportion of subjects who had seroconversion (change of baseline rSBI < 8 or < 128 to a post-immune rSBI ≥ 8 or ≥ 128) after immunization, or who had a 4-fold increase in rSBI over baseline levels. The percentage of subjects and associated 95% Clopper-Pearson CIs were calculated for each serogroup. Differences in GMIs between pre- and post-vaccine sera were compared using a two-sample, paired t-test after logarithmic transformation. Comparisons between both groups were evaluated with the Mann-Whitney U test for continuous variables and the Pearson χ2 test or Fisher's exact test for categorical variables. Nonparametric correlations between the geometric mean fold increase (GMFI) and GMI at pre-immunization were calculated with the Spearman's correlation coefficient. Reverse cumulative distribution curves were used to represent the percentage of participants that achieved a different rSBI for each of the meningococcal serogroups. P values less than 0.05 were considered significant. Statistical analysis was performed using SPSS statistical software (version 23.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
The study was conducted in accordance with the Good Clinical Practice Guidelines and the Declaration of Helsinki. The protocol, informed consent, and assent form were reviewed and approved by the Institutional Review Board (IRB) of Ewha Womans University Mokdong Hospital (IRB No. EUMC 2016-01-027-001). Written informed consent was obtained before enrollment from all participants following a detailed explanation of the study. This study was registered at the Clinical Research Information Service (CRIS, http://cris.nih.go.kr), number KCT0002460.
RESULTS
Subject characteristics
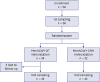
A total of 66 subjects (20–49 years of age) were enrolled at Ewha Womans University Mokdong Hospital in the Korea between March and July 2016. Subject characteristics were similar between the study groups (Table 1). Of the 66 subjects enrolled, 64 completed the study according to the protocol (Fig. 1). Two subjects from the MenACWY-DT group withdrew from the study because they were lost to follow-up.
Table 1
Patient demographic characteristics at baseline
Comparison of immunogenicity between groups
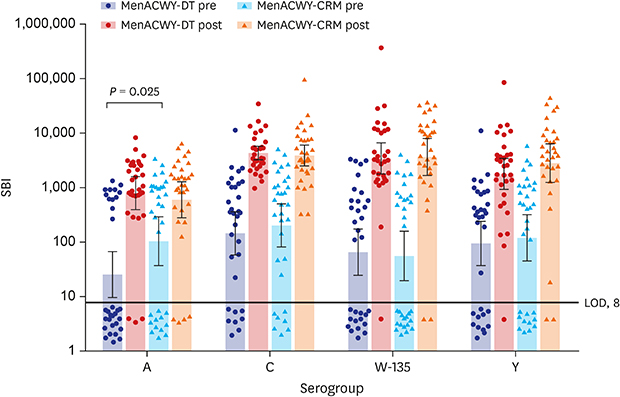
Immunogenicity results including GMIs, seropositive rates, GMFIs, and seroresponse rates are shown in Table 2. There were no significant differences between vaccine groups in terms of baseline GMIs except for serogroup A. Significant increases in GMIs were observed at 1 month after immunization for all four serogroups in both vaccine groups. After immunization, most subjects achieved rSBI values above the protective level (88%–100%) against vaccine serogroups (Table 2 and Fig. 2). Further, seropositive rates at 1 month after immunization were similar among all four serogroups across both vaccine groups.
Table 2
Immunogenicity against meningococcal serogroups A, C, W-135, and Y before and after immunization with meningococcal vaccines (MenACWY-DT group, n = 32; MenACWY-CRM group, n = 32)

MenACWY-DT = quadrivalent meningococcal diphtheria toxoid conjugate vaccine, MenACWY-CRM = quadrivalent meningococcal CRM197 conjugate vaccine, GMI = geometric mean index, CI = confidence interval, SBI = serum bactericidal index, GMFI = geometric mean fold-increase, DT = diphtheria toxoid, CRM = cross reactive material 197, NA = not available.
aSeroresponse rate was defined as the proportion of subjects who had seroconversion (change of baseline SBI < 8 or < 128 to a post-immune SBI ≥ 8 or ≥ 128) after immunization, or who had a 4-fold or more increase in SBI from pre- to post-immunization; bStatistically different between vaccine groups (P < 0.05).
Fig. 2
Scatter plot of serum bactericidal indices against serogroups A, C, W-135, and Y at baseline and post-immunization (1 month after). At baseline, MenACWY-DT group, open circle; 1 month after, MenACWY-DT group, closed circle; at baseline, MenACWY-CRM group, open triangle; 1 month after, MenACWY-CRM group, closed triangle; black line, limit of detection based on our assay format.
MenACWY-DT = quadrivalent meningococcal diphtheria toxoid conjugate vaccine, MenACWY-CRM = quadrivalent meningococcal CRM197 conjugate vaccine, LOD = limit of detection, SBI = serum bactericidal index.

Although the GMFI and seroresponse rate for serogroup A were significantly different, these for the other serogroups were not significantly different between vaccine groups. Based on post hoc analyses restricted to those subjects who were seronegative (rSBI < 8) at baseline, the GMFI in the MenACWY-DT group for serogroup A was not significantly different than that in the MenACWY-CRM group (120 for MenACWY-DT group vs. 34 for MenACWY-CRM group, P = 0.16). The seroresponse rate for serogroup A was increased to 67% (6/12) in the MenACWY-CRM group and 85% (17/20) in MenACWY-DT group; however, there was no significant difference between these values (P = 0.379). The correlation between the serum bactericidal indices (SBIs) in pre-immunized sera and the GMFI were then further analyzed (Fig. 3). Moreover, the SBIs of pre-immunized sera were significantly negatively correlated (Spearman's rho = −0.65; P < 0.001) with the GMFI, especially in serogroup C (Spearman's rho = −0.91). Among seropositive subjects at baseline, seroresponse rates for all serogroups in total subjects were low (74/134, 45%). For serogroup A, the seroresponse rate was 22%.
Fig. 3
Scatter plots for the serum bactericidal indices at pre-immunization and fold-increases from pre- to post-immunization. Horizontal black line, cut-off of immune response (4-fold increases in serum bactericidal indices from pre- to post-immunization); vertical black line, cut-off of seropositivity for serum bactericidal indices.
MenACWY-DT = quadrivalent meningococcal diphtheria toxoid conjugate vaccine, MenACWY-CRM = quadrivalent meningococcal CRM197 conjugate vaccine, SBI = serum bactericidal index, rho = Spearman correlation coefficient.

Finally, a reverse cumulative distribution curve showed the responses to the four serogroups at baseline and 1 month after immunization in the two vaccine groups (Fig. 4). After immunization, the curves shifted to the right compared to those before immunization in both groups and for all four serogroups. The curve for the MenACWY-CRM group at pre-immunization in serogroup A was farther to the right than that for the MenACWY-DT group, indicating that the subjects in the MenACWY-CRM group showed higher rSBIs than those in the MenACWY-DT group. However, this gap disappeared after immunization.
Fig. 4
Reverse cumulative distribution curve of serum bactericidal indices against serogroup A, C, W-135, and Y at baseline and post-immunization (1 month after). At baseline, MenACWY-DT group, open circle; 1 month after, DT group, closed circle; at baseline, MenACWY-CRM group, open triangle; 1 month after, closed triangle; vertical black line, limit of detection (8).
MenACWY-DT = quadrivalent meningococcal diphtheria toxoid conjugate vaccine, DT = diphtheria toxoid, MenACWY-CRM = quadrivalent meningococcal CRM197 conjugate vaccine, SBI = serum bactericidal index.

DISCUSSION
The purpose of this study was to assess the immunogenicity of two meningococcal vaccines approved in Korea using healthy adults. MenACWY-CRM and MenACWY-DT vaccination induced an immune response against all four serogroups, as evidenced by the proportions of subjects with rSBIs ≥ 128 (88% to 100%) and increases in the GMFI (5 to 63). No unexpected or otherwise clinically significant adverse events related to the administration of the vaccines were reported (data not shown).
For the licensure of MenACWY-CRM and MenACWY-DT vaccines in Korea, immunogenicity and safety studies (phase III trials) were conducted in 201014 and 2012,15 respectively, and the results showed that they were well tolerated and immunogenic. Both have consequently been used for high-risk populations. They were also sequentially included in a national immunization program for new military recruits without performing comparative studies between them.
The immunogenicity of these vaccines in this study is consistent with the previous data in Korea,1415 although the interpretation of historical comparisons is difficult because of differences in study populations and serum bactericidal assay (SBA) procedures. However, a higher seropositive rate (88%) of pre-immunization sera and a lower seroresponse rate (28%) for serogroup W-135 were observed in an immunogenicity study using hSBA of MenACWY-CRM conducted using a population similar to ours.14 The high seropositive rates in the pre-immunization group for serogroup W-135 were also observed in studies using hSBA for a different population.1617 However, this pattern was not observed in this study by measuring the rSBA. Further, a previous immunogenicity15 study using the rSBA of MenACWY-DT in the same population showed different results compared not only to hSBA results but also ours. Although the seroresponse rates for all four serogroups were higher than 60% of participants with a single dose of MenACYW-DT, similar to that observed in other studies, high seropositive rates before immunization were only observed for serogroup A and Y.
The causes of the naturally high levels of acquired (pre-vaccination) bactericidal antibodies cannot be attributed only to antibodies specific for capsular polysaccharide antigens. Antibody priming with cross-reactive antigens such as subcapsular protein antigens can occur during environmental exposure to Neisseria species or certain types of enteric bacteria.1819 An analysis of other strains with the same serogroup and different subcapsular antigens could have also provided additional bactericidal data to clarify the high levels of naturally acquired antibodies in this population. A carriage study of the same population would also be helpful to elucidate this, but insufficient epidemiological data exist in Korea.
In the MenACWY-CRM group, GMI at baseline and GMFI for serogroup A were significantly lower than those in the MenACWY-DT group. The high SBIs of pre-immunized sera were significantly correlated with low immune responses, especially in serogroup C. Among seropositive subjects at baseline, seroresponse rates for all serogroups in all subjects were low. These findings do not necessarily mean that vaccine immunogenicity is poor. SBA reflects various bactericidal antibodies, not only antibodies induced by capsular antigens. Many previous studies have shown insignificant correlations between anti-capsular immunoglobulin G concentrations and SBI.202122 Though SBA values are likely to reflect clinical immunity more accurately than those obtained by enzyme-linked immunosorbent assay, pre-existing anti-meningococcal antibodies other than anti-capsular antibodies could mask the immunogenicity of vaccines.1422 Previous Korean studies on MenACWY-CRM showed this by measuring antibody concentrations.14 Even if immunogenicity is sufficient, it is thus necessary to reconsider immunization in these individuals who show high seropositive rates at baseline and low increases in SBIs after immunization. Though accurate epidemiologic data are scarce, the incidence of meningococcal invasive diseases in Korea (0.012–0.08/100,000) is lower than that in Europe, North America, and Africa.23 The relatively low incidence of meningococcal diseases and our results could support the current policy that meningococcal immunization is recommended only for high-risk groups and not for the general population. Monitoring circulating meningococcal strains and seroepidemiology in Korea should be conducted to provide additional evidence for this.
Immune response differences between MenACWY-CRM and MenACWY-DT might be related to differences in the carrier proteins used in each vaccine. As CRM197 is a nontoxic mutant of the diphtheria toxin, it does not require detoxification using formaldehyde or glutaraldehyde, a process employed during the preparation of DTs that can cause extensive crosslinking of the carrier protein to accessory antigens, with epitope modifications.24 Comparative studies between two vaccines were conducted for the licensure of MenACWY-CRM, which was developed later. In comparative trials, noninferior criteria were met for most serogroups except serogroup A, based on a study using children.67 Moreover, differences favoring MenACWY-CRM were observed in most trials. However, our results showed no significant differences. Although there was a difference in GMFI and seroresponse rate for serogroup A, even this difference disappeared after restricting the results to seronegative subjects. Further studies on a larger Korean population might clarify this difference from previous studies.
In Korea, meningococcal outbreaks in the army have often occurred despite the relatively low annual incidence among the general population. Thus, an effective immunization policy for military recruits based on evidence should be established for prevention. However, reliable data regarding the incidence, serogroup distribution, and seroepidemiology were not previously available. Moreover, recent carriage studies for adolescents and young adults indicated a high proportion of serogroup B meningococcus, which is not covered by MenACWY.2526 Another issue is that DT vaccines, which are concomitantly or sequentially administrated with MenACWY for military recruits, might result in immunologic interference for the anti-meningococcal response, due to the immunological cross-reactivity between them.9 Immunization with a carrier protein alone might suppress the immune response to a hapten linked to the carrier protein. This suppression could occur when the carrier is overloaded.27 Immune interferences between the tetanus-DT-containing vaccines and meningococcal conjugate vaccines have been evaluated previously,28293031 but the results were not concordant. Therefore, the data for the Korean population and the actual immunization policy in Korea should be evaluated further.
In conclusion, both licensed meningococcal vaccines in Korea were found to be immunogenic for all vaccine serogroups. Further investigations of the serotype distribution of circulating meningococci and the immune interference from other diphtheria toxin-containing vaccines concomitantly used for military recruits are needed to optimize immunization policies.
 XML Download
XML Download