

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes is one of chronic diseases and the mortality rate caused by diabetes has increased every year worldwide [1]. Diabetes is a major risk factor for cardiocerebrovascular disease, which is a major cause of death in diabetic patients [2]. When HbA1c (6.5% and over) was included in the diagnostic criteria for diabetes, the prevalence of diabetes has increased in both men and women in Korea recently [3].
Only strict glycemic control can prevent complications of diabetes [4]. According to the guidelines for diabetes by the American Diabetes Association (ADA), controlling BMI, HbA1c, blood pressure and cholesterol is recommended [5]. Based on the Korean diabetes management guidelines, HbA1c < 6.5%, blood pressure ≤ 140/80 mmHg, LDL-cholesterol ≤ 100 mg/dL, TG ≤ 150 mg/dL and HDL-cholesterol ≥ 40 mg/dL for men and ≥ 50 mg/dL for women are recommended [6].
Pharmacotherapy, dietary therapy and exercise therapy are commonly used to manage diabetes. Dietary therapy plays an important role in delaying the development of diabetic complications during the course of treatment and progression of diabetes. Proper dietary therapy improves metabolic abnormalities and blood lipid profiles [78]. Studies on nutrient intakes in Korean diabetic patients showed that the intake of carbohydrates was more than 60% and even higher in women than in men [910]. The increased carbohydrate intake causes hyperglycemia, which can develop oxidative stress in the body and finally cause tissue damage [11]. In addition, excessive insulin secretion can increase body fat to induce obesity [12].
Among diabetic complications, microvascular complications are increased along with an increased duration of diabetes, while macrovascular complications are affected by the risk factors for cardiovascular diseases (CVDs) [8]. In addition, the prevalence of CVDs is more than 2–4 times higher in diabetic patients compared to non-diabetic patients [1314]. The awareness of diabetes in Korea tends to be higher in women than in men. In particular, the awareness rate was the lowest in men in their 30 s and 40 s [3].
According to a study by the American Medical Care System, the onset of diabetes, on average, is up to 10–12 years before clinical diagnosis [15]. Complications such as diabetic retinopathy or diabetic neuropathy are commonly found at the time of diagnosis [16] and CVDs such as peripheral arterial disease and coronary heart disease are co-diagnosed in many cases [17]. Therefore, early diagnosis is very important to prevent complications and comorbidities of diabetes, yet associations among patients' awareness of diabetes, its clinical indicators, and nutrient intakes have not been well investigated in the Korean population, especially using nationally representative data.
The purpose of this study was to examine clinical indices and nutrient intakes based on diabetes awareness among adults aged 19–64 years, using nationally representative data from the 2012–2013 Korea National Health and Nutrition Examination Survey (KNHANES).
SUBJECTS AND METHODS
Study design and participants
A cross-sectional secondary analysis was conducted using the 2012–2013 KNHANES data. Participants who were 19–64 years old and diagnosed with diabetes at the time of the measurement were included. For diabetes indicators, fasting blood glucose and HbA1c were used from the hematology section of the KNHANES. A total of 523 participants were divided into two groups: (1) the aware group (297; 148 men and 149 women), defined as individuals who were diagnosed by medical doctors; and (2) the non-aware group (226; 103 men and 123 women), defined as individuals who were not clinically diagnosed at the time of the measurement but had 8-h fasting plasma glucose over 126 mg/dL or HbA1c over 6.5%. The Institutional Review Board (IRB) of the Korea Center for Disease Control and Prevention approved the KNHANES (IRB. 2012-01EXP-01-2C and 2013-07CON-03-4C).
General characteristics
Information on gender, age, income level, education level, exercise, drinking and smoking patterns was obtained from the KNHANES data. The exercise patterns were classified into two levels: moderate/walking was classified as more than 10 minutes per session and more than 20 minutes of daily exercise for at least 3 days a week and vigorous exercise was classified as more than 10 minutes per session and more than 30 minutes of daily exercise for at least 5 days a week. Drinking pattern was classified into a binary variable: either equal to greater vs. fewer than once a month during the past one year. Height, weight and waist circumference data were extracted from the anthropometric measurement section of the KNHANES.
Prevalence and diagnosis of hypertension and dyslipidemia
The prevalence of hypertension was defined as systolic pressure ≥ 140 mmHg or diastolic pressure ≥ 90 mmHg. The prevalence of dyslipidemia was defined as total cholesterol ≥ 240 mg/dL or triglyceride ≥ 200 mg/dL or HDL-cholesterol < 40 mg/dL or LDL-cholesterol ≥ 160 mg/dL. The diagnosis rate for each of hypertension and dyslipidemia was defined as individuals who were diagnosed by a medical doctor. LDL-cholesterol was calculated with the Friedewald equation for those with serum triglyceride level ≤ 400 mg/dL [18].
Clinical indices
The following data were obtained from the health examination survey: systolic pressure, diastolic pressure, total-cholesterol, HDL-cholesterol, triglyceride, hemoglobin, hematocrit, blood urea nitrogen (BUN) and blood creatinine.
Nutrient intakes
The intake of nutrients was analyzed through the type and amount of food consumed the day before the survey using the 24h recall method. The ratio of intakes of protein, fat and carbohydrates was calculated using the presented nutrient values. For the analysis of the intake ratio by nutrients, the Dietary Reference Intakes for Koreans (2010) was used for different age groups.
Statistical analysis
Statistical analysis was performed after adjusting for the KNHANES sample weights, strata and clusters. Clinical indices and nutrient intakes were analyzed after controlling for age. Group comparisons were performed based on the aware vs. non-aware groups. Independent samples t-tests were performed for continuous data and χ2-tests were performed for nominal data. General linear models were used to examine differences in biochemical indices, energy and nutrient intakes by group, after controlling for age. To analyze the proper ratio of protein, fat and carbohydrates intake by group, logistic regressions were performed. Odds ratio (OR) and 95% confidence interval (CI) are presented. All data in the study were analyzed using SPSS 19.0 (SPSS Inc., Chicago, USA) and the statistical significances were tested at P < 0.05.
RESULTS
General characteristics
The general characteristics of the participants by gender and diabetes awareness are shown in Table 1. The average ages of men and women were significantly higher at 53.2 and 53.6 years in the aware group compared to 48.8 and 49.3 years in the non-aware group (P = 0.002 and P = 0.004), respectively. There were significant differences in the distribution of age categories between the aware and the non-aware groups. A large percentage of men and women in the non-aware group was in their 50 s (41.6%) and 60 s or older (23.5%), while 43.1% of the aware group was in their 60 s or older (P = 0.001). The average BMI in men was significantly higher at 25.8 kg/m2 in the non-aware group compared to 24.7 kg/m2 in the aware group (P = 0.031). The average BMI in women was not significantly different between two groups, but the distribution of BMI was significantly different (P = 0.026). The obesity rate was 50.3% in the female aware group and 64.2% in the female non-aware group.
Prevalence and diagnosis of hypertension and dyslipidemia
The comorbidity status of hypertension and dyslipidemia is shown in Table 2. The prevalence of hypertension in women was significantly higher in the aware group (55.0%) compared to 35.8% in the non-aware group (P = 0.013) and also more women in the aware group were clinically diagnosed with hypertension (53.0%) compared to the non-aware group (30.1%; P = 0.008). For men, there was no significant difference in prevalence but a significantly higher percentage of men in the aware group (44.6%) had been clinically diagnosed with hypertension compared to the non-aware group (25.2%; P = 0.024). The prevalence of dyslipidemia was not significantly different between the two groups. However, there were significant differences in the rate of clinical diagnosis of dyslipidemia in both men and women: in men, it was significantly higher in the aware group (31.1%) compared to the non-aware group (11.7%; P = 0.001); and in women, it was 47.0% in the aware group and 17.1% in the non-aware group (P < 0.001).
Clinical indices
The clinical indices of the subjects are shown in Table 3. Total cholesterol and LDL-cholesterol were significantly higher in the non-aware group compared to the aware group in both men and women (P < 0.001). In men, triglyceride was significantly higher at 199.3 mg/dL in the non-aware group compared to 153.8 mg/dL in the aware group (P < 0.001). Hemoglobin was 14.9 g/dL in the aware group and 15.5 g/dL in the non-aware group (P = 0.002). In women, hemoglobin was significantly lower in the aware group (P = 0.019). Hematocrit was significantly lower in the aware group compared to the non-aware group in both men (P = 0.002) and women (P = 0.006).
Nutrient intakes
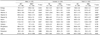
Daily calorie and nutrient intakes are shown in Table 4. There was no significant difference between the aware and the non-aware groups among men. In women, calorie intake was 1,665 kcal in the aware group and 1,891 kcal in the non-aware group (P = 0.033). Carbohydrate intake was significantly higher in the non-aware group (319.2 g) compared to the aware group (280.7 g; P = 0.048). Vitamin B2 intake was significantly higher in the non-aware group (1.3 mg) compared to the aware group (1.1 mg; P = 0.042) In total, calorie intake was 1,990 kcal in the aware group and 2,218 kcal in the non-aware group (P = 0.025). Protein intake was significantly higher in the non-aware group (81.5 g) compared to the aware group (70.9 g; P = 0.038). Carbohydrate intake was significantly higher in the non-aware group (344.6 g) compared to the aware group (314.3 g; P = 0.044).
The results of nutrient intake of Korean Reference Nutrient Intake (RNI) of the subjects are shown in Table 5. The ratio of calorie intake to RNI was significantly higher at 106.3% in the non-aware group compared to 94.0% in the aware group (P = 0.013), and both men and women in the non-aware group had an intake higher than Korean RNI. In men, protein intake was significantly higher at 177.8% in the non-aware group than 148.8% in the aware group (P = 0.043). In men, vitamin B1 intake was significantly higher in the non-aware group compared to the aware group (P = 0.024). In women, vitamin B2 intake was significantly higher in the non-aware group compared to the aware group (P = 0.014).
The degree of risk exerted by diabetes awareness on clinical indices and nutrient intakes is shown in Table 6. The crude risk for abnormal values was significantly higher for waist circumference, diastolic blood pressure, total cholesterol, LDL-cholesterol and triglycerides in the non-aware group. After controlling for gender, age, income, education level, and the duration of diabetes, the risk for abnormal values was significantly higher for waist circumference, total cholesterol, LDL-cholesterol and triglycerides in the non-aware group. After additional correction for smoking, drinking, exercise and BMI, the risk for waist circumference over 90cm in men and over 85cm in women was 2.64 times (95% CI: 1.18–5.88) higher in the non-aware group (P = 0.018); and the risk for total cholesterol over 240 mg/dL was 3.44 times (95% CI: 1.58–7.52) higher in the non-aware group (P = 0.002). The risk for LDL-cholesterol over 160 mg/dL was 4.59 times (95% CI: 2.07–10.17) higher in the non-aware group (P < 0.001). Among nutrient intakes, abnormal intake ratios of protein, fat and carbohydrates were not significantly different.
DISCUSSION
This is the first study analyzing the health-related habits, clinical indices and nutrient intakes based on the diabetes awareness in the Korean adult population using nationally representative data (2012–2013 KNHANES) [3]. Early diagnosis and treatment of diabetes significantly reduces the risks for CVDs [19]. Therefore, providing men in their 30s with diabetes education would benefit the population health in Korea by reducing the prevalence and enhancing early treatment of diabetes in young men.
BMI was significantly higher in the non-aware group compared to the aware group and the ratio of BMI over 25 kg/m2 was 45.5% and 62.4% in the aware and non-aware groups, respectively. Obesity is a major preceding factor of diabetes and a factor for preventing and delaying diabetes in individuals with the possibility of progressing diabetes. Weight control for obesity is needed in both the aware and non-aware groups.
Hypertension is a common comorbidity in diabetic patients and a major risk factor for CVDs [2021]. Strict blood pressure control can reduce the mortality and delay complications such as diabetic retinopathy and reduced vision [22]. The study results indicated that the non-aware group was unaware of not only diabetes but also accompanying diseases such as hypertension and dyslipidemia. The diagnosis rate for hypertension and dyslipidemia was lower than the prevalence rate, demonstrating uncontrolled blood pressure and blood lipid profiles in the aware group. Screening and strict management of blood pressure, LDL-cholesterol, triglycerides and HDL-cholesterol are recommended for diabetic individuals. The results of this study were consistent with those in the studies on diabetic patients by Kwon et al. [23] and on diabetes awareness by Kim et al. [5]. Cardiocerebrovascular diseases rank as the 2nd and 3rdcauses of death in Korea and individuals with diabetes have higher risks for CVDs [24]. Because the prevalence of CVD is 2–4 times higher in diabetic patients than in non-diabetic patients, early diagnosis in the non-aware group can promote the regulation of risk factors for CVDs through glycemic control and blood lipid control [2526].
Park et al. [27] showed a significant relationship between carbohydrate intake and waist circumference after controlling for total energy intake and BMI. The ADA recommends that the total amount rather than the type of carbohydrates is important in the intake of carbohydrates. Thus, education on carbohydrate control is highly recommended.
Limitations of the study include that the definition of the non-aware group was based on either fasting blood glucose or HbA1c data from the KNHANES. Because it relied on one measurement for each individual, it is possible that some participants might have been miss-categorized as diabetic.
Although the currently recommended target for diabetes screening is individuals over 40 years or over 30 years in case of having diabetic risk factors, this study suggested that diabetes screening before 40 years of age through regular health check-up would be beneficial. In the aware group, continuous and systematic management and education are necessary to prevent diabetic complications. Careful self-monitoring for glycemic control is also recommended for diabetic patients. To increase overall diabetes awareness, not only individual-level education but also social marketing or other community-level education strategies will be beneficial. Further studies determining effective strategies to increase diabetes awareness and screening as well as rigorous diabetes management programs are needed.





 XML Download
XML Download