

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The size of elderly population is increasing rapidly worldwide, and according to data from Statistics Korea in 2016, people aged 65 years and older accounted for 13.6% of the entire Korean population. Cardiovascular (CV) diseases are a leading cause of death in elderly people, and it presents various challenges in both diagnosis and treatment.1 The management of elderly patients with CV diseases differs from the management of younger patients with the same diseases.2 In order to better define treatment and predict prognosis, it is more important to determine the exercise capacity in elderly patients than that in younger patients.
Cardiopulmonary exercise testing (CPET) is an exercise stress test with concomitant expired gas analysis, which provides objective parameters of functional capacity. Since CPET can assess integrated exercise responses of cardiopulmonary, vascular, and skeletomuscular systems,3 it can reveal abnormalities that are not apparent in a resting state. Current clinical indications of CPET are used to define the cause of dyspnea/exercise intolerance, establish the severity of advanced cardiac disease, determine cardiac intervention in valvular/congenital heart disease, and precisely evaluate the functional response to an intervention.4 CPET is also useful in the assessment of preoperative risk and prediction of postoperative CV outcomes.5 Therefore, risk assessment using CPET in elderly patients with CV diseases is becoming more important.
Nonetheless, many Korean physicians are unwilling to perform exercise stress testing, especially in elderly patients with CV diseases. Their reasons include: 1) concerns regarding the risk of an adverse event during CPET; 2) unavailability of CPET equipment; 3) lack of awareness about the importance of evaluating exercise capacity; and 4) preference for evaluating cardiac function over performing exercise capacity assessment.
Previous studies demonstrated the safety of CPET for people with CV diseases such as heart failure (HF), coronary artery disease, and cardiac transplantation. The 2002 American Heart Association exercise testing guidelines cite an adverse event rate of up to 0.04% or 1 per 2500 tests.6 CPET has been shown to be safe in HF patients with severe systolic dysfunction.7 Even in patients with underlying high-risk CV diseases, CPET is generally a safe procedure with a 0.16% total adverse event rate.8 CV disease in the elderly population has been considered a contraindication to exercise testing, albeit with a lack of data about CPET safety.
As cardiac rehabilitation becomes more common, demand for CPET has increased in Korea. However, large-scale data on CPET values for Koreans with CV disease are lacking. Therefore, we examined the characteristics and safety of CPET in a large, heterogeneous population of elderly Korean patients with underlying CV diseases.
MATERIALS AND METHODS
Study population
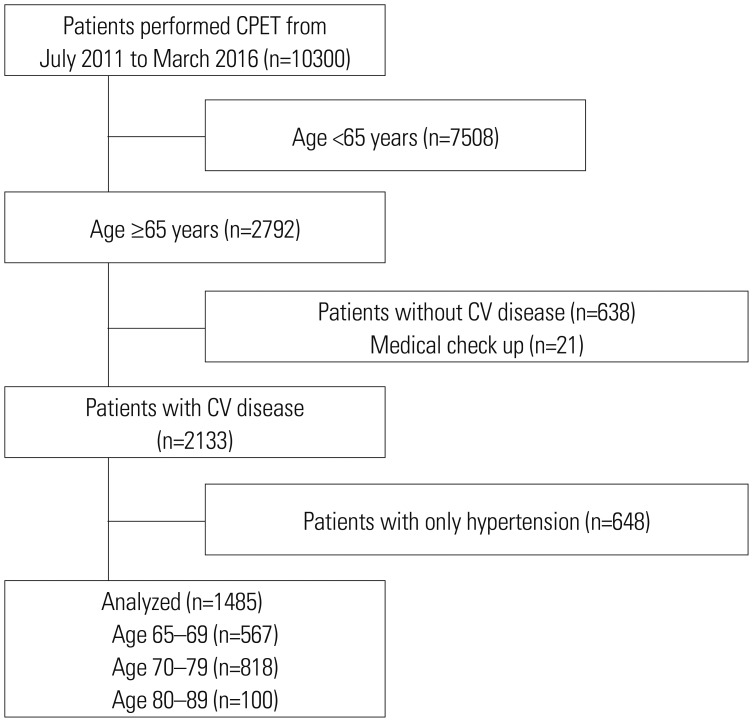
This was a cross-sectional, observational, single-center cohort study. We reviewed records of 10300 patients who underwent CPET between July 2011 and March 2016 at the Cardiac Wellness Center of Severance Cardiovascular Hospital. We defined older patients as being 65 years in age or older, excluding those aged <65 years (n=7508). Patients without definite CV disease (n=638) and those who underwent CPET for routine medical check-up (n=21) were excluded. We also excluded patients who only had hypertension (HTN) without other CV disease (n=648). A total of 1485 patients ≥65 years with CV disease who underwent CPET were identified. We included data on patients who underwent CPET multiple times during the study period. Demographic characteristics including age, sex, body mass index, and medical history including HTN, diabetes mellitus, chronic kidney disease, dyslipidemia, and cerebrovascular attack were reviewed. HTN was defined as previous diagnosis or systolic blood pressure (BP) >140 mm Hg or diastolic BP >90 mm Hg by repeated BP measurements. CV diseases were categorized as: ischemic heart disease (IHD), HF, valvular heart disease (VHD), hypertrophic cardiomyopathy (HCMP), and congenital heart disease. IHD was defined as myocardial infarction, unstable angina, and stable angina that had significant coronary artery stenosis (luminal narrowing ≥70%) with or without coronary artery bypass graft or percutaneous coronary intervention. HF was identified by reviewing medical records for patients with B-type natriuretic peptide (BNP) greater than 35 pg/mL or N-terminal pro-BNP levels greater than 125 pg/mL and echocardiography favorable for HF.9 VHD was diagnosed and graded through echocardiogram according to 2014 AHA/ACC guidelines.10 Diagnosis of HCMP was determined by echocardiography based on presence of myocardial hypertrophy without local or systemic etiologies.11 Obstructive HCMP was defined as left ventricular outflow tract (LVOT) peak instantaneous Doppler gradient ≥30 mm Hg upon resting or when provoked with the Valsalva maneuver. Non-obstructive HCMP was defined as both a resting and provoked gradient of <30 mm Hg.12 This study was approved by the ethics committee of Severance Hospital, Seoul, South Korea (IRB No. 4-2016-1087), and written informed consent was waived due to the retrospective nature of this study.
Cardiopulmonary exercise testing
All CPET was performed by specialist nurses certified by the American College of Sports Medicine and supervised by a single cardiologist. Before tests, patients were assessed for resting BP, heart rate (HR), and echocardiographic results, including left ventricular ejection fraction. Patients with ongoing chest pain at rest, pulmonary edema on chest X-ray, hypotension, significant bradycardia/tachycardia, or significant ST changes >0.05 mV at resting electrocardiography (ECG) were prohibited from undergoing the test. All patients underwent CPET according to the modified Bruce ramp protocol using two motordriven treadmills (Exercise Testing System®, GE Healthcare, Chicago, IL, USA). For expired gas collection and analysis, the Quark CPET (COSMED, Rome, Italy) was used. CPET was performed by monitoring 12-lead ECG, manual BP measurements, and HR at every stage. Total test time was 16 minutes 40 seconds, and recovery time was at least 5 minutes. Speed and grade were increased every 20 seconds. All patients were encouraged to perform a submaximal, symptom-limited test. Termination criteria were patient request, ventricular arrhythmia [ventricular tachycardia (VT) or ventricular fibrillation], or horizontal or downsloping ST depression of ≥1 mm Hg during exercise. Peak respiratory exchange ratio (RER), exercise duration, lactate threshold (LT) time, peak oxygen uptake (peak VO2), metabolic equivalents of task (METs), dead space/tidal volume (VD/VT) ratio, partial pressure of end-tidal carbon dioxide, minute ventilation-carbon dioxide output relationship (VE/VCO2 slope), peak systolic BP, peak HR, HR reserve, and HR recovery were measured automatically. Peak VO2 was defined as the highest VO2 value achieved during exercise.
Interpretation and adverse events of cardiopulmonary exercise testing
All CPET results with exercise ECG were interpreted by the supervising cardiologist. A 1.0-mm horizontal or downsloping ST-segment depression 0.08 seconds after J-point in the absence of significant resting ST-T abnormalities, pre-excitation, ventricular pacing, digitalis, or left bundle branch block was considered a positive finding for ischemia. Exercise effort quality was assessed by RER, which was calculated using the formula VCO2/VO2.
According to a previous study on CPET safety,8 we defined adverse events for CPET as: 1) death during the stress test, 2) external defibrillation or implantable cardioverter-defibrillator discharge, 3) sustained VT (wide complex tachycardia lasting longer than 30 seconds), 4) myocardial infarction, 5) syncope, 6) administration of advanced cardiac life support medications, 7) referral for direct hospital admission, or 8) referral to emergency department.
Statistical analysis
Statistical analyses were performed with SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Data normality was tested using the Kolmogorov-Smirnov test. Values are expressed as means (±SD) for numerical variables or as number of participants and their percentages for categorical variables. Continuous variables were compared using the Student's t-test and ANOVA test. Analysis of categorical data was performed using the chi-square test. Two-tailed p<0.05 was considered statistically significant.
RESULTS
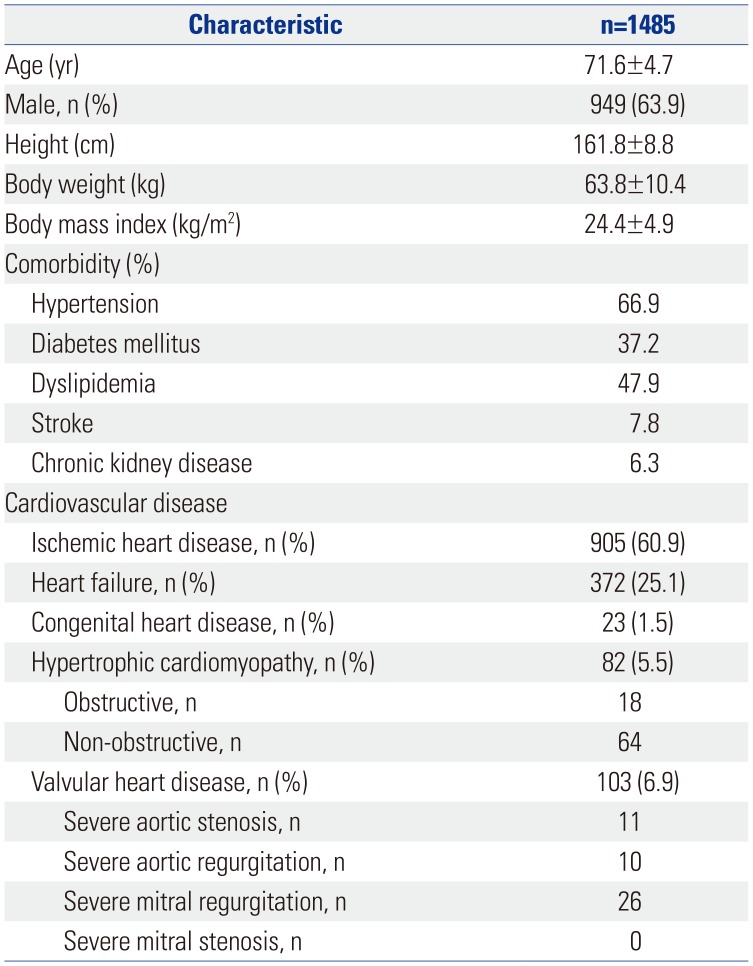
We analyzed CPET data on 1485 patients. The mean age was 71.6±4.7 years, with 567 patients aged 60–65 years, 818 patients aged 70–79 years, and 100 patients aged 80–89 years (Fig. 1). Among them, 154 patients underwent CPET multiple times (two times: 129 patients; three times: 21 patients; four times: 4 patients). Baseline clinical characteristics and categories of CV diseases are presented in Table 1. In the categories of CV diseases, IHD was the most common (60.9%), followed by HF (25.1%). Among 82 patients with HCMP, 18 had hemodynamically LVOT obstruction. Among patients with VHD, 47 had severe VHD and mitral regurgitation was most common.
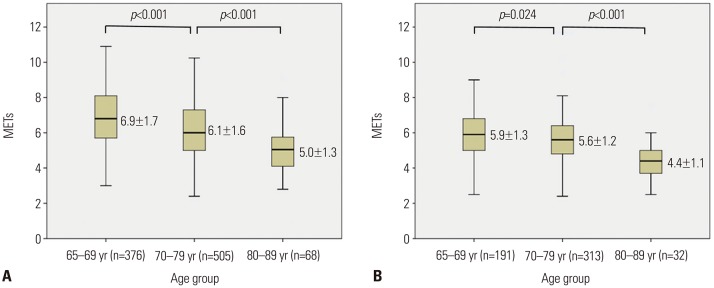
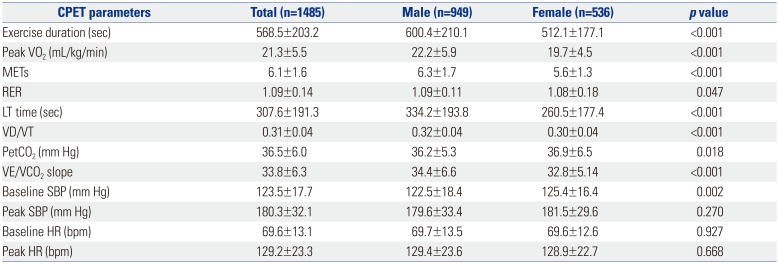
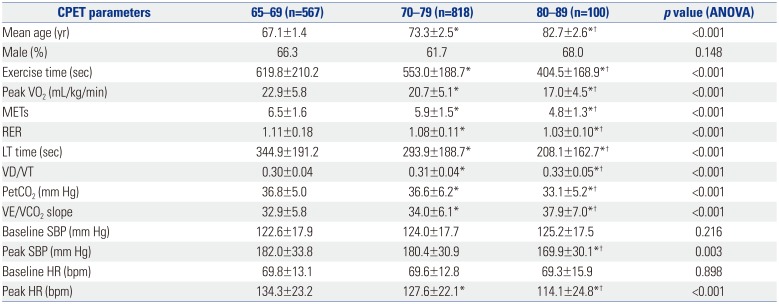
CPET results are shown in Table 2. For overall patients, mean RER was 1.09±0.14 with 268 (18.0%) with RER <1.0. Mean peak VO2 was 21.35±5.5 mL/kg/min, mean METs was 6.1±1.6 and mean exercise duration was 568.5±203.2 seconds. Men showed better exercise capacity than women (peak VO2, 22.5±5.9 vs. 19.7±4.5 mL/kg/min, p<0.001; exercise time 600.4±210.1 vs. 512.1±177.1 sec, p<0.001). Comparing CPET results by age group showed a significant difference in exercise capacity (65–69 vs. 70–79 vs. 80–89: peak VO2, 22.9±5.8 vs. 20.7±5.1 vs. 17.0±4.5 mL/kg/min, p<0.001; VE/VCO2 slope, 32.9±5.8 vs. 34.0±6.1 vs. 37.9±7.0, p<0.001) (Table 3). When we analyzed exercise capacity according to age grouped by sex, METs were significantly reduced as age increased in both men and women (Fig. 2). CPET results for patients of all ages who underwent CPET at our center during the same period are in Supplementary Table 1 (only online).
A total of three adverse cardiovascular events were noted during CPET for all patients. All events were sustained VT with spontaneous recovery to sinus rhythm without electrical cardioversion. Among the patients, two had dilated cardiomyopathy and one had IHD (Table 4).
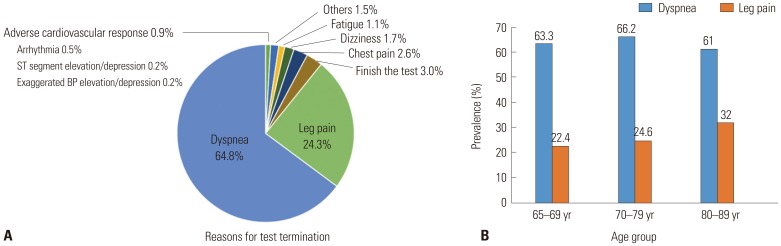
Reasons for termination of CPET are shown in Fig. 3A. Only 45 patients (3.0%) completed CPET according to the protocol with no patients aged ≥80 years. Dyspnea was the most common cause, and leg discomfort was the second most common cause, accounting for 64.8% and 24.3%, respectively. Leg pain was significantly higher in octogenarians than other groups (65–69 vs. 70–79 vs. 80–89: 22.4% vs. 24.6% vs. 32.0%, p<0.001) (Fig. 3B).
DISCUSSION
This study found a lower adverse event rate (0.20%) in a large, elderly population. Previously, the Mayo Clinic reported 0.16% adverse events in high-risk CV patients and patients older than 65 years showed similar event rate (0.16%).8 We had fewer high-risk patients than in the Mayo Clinic study, but our population contained some high-risk patients with severe VHD (n=46), HCMP (n=82), severely reduced LVEF (<30%) (n=71), and severely reduced functional capacity by peak VO2 <14 mL/kg/min (n=142). Based on the statistics maintained at our center, among all age groups of 13031 patients who underwent CPET, a total of eight adverse events occurred (total adverse event rate 0.061%: seven cases were sustained VT, all self-terminated the test, and one case was syncope followed by cardiac arrest during the recovery phase). All eight patients were aged under 70 years, suggesting that older age was not an absolute risk factor for CPET. Although there is a limit to present safety of CPET by statistically low values, it seems to be meaningful considering the number of patients in our data.
Bicycle ergometers are widely used in CPET due to their lower cost, compact space requirements, and reduced noise level compared to a treadmill.13 A standard bicycle exercise ramp protocol is relatively safe for elderly patients with chronic HF.14 However, bicycles have the limitation that leg fatigue can induce early termination of a test, and peak VO2 is 10–20% lower in individuals not accustomed to cycling.15 In exercise protocols using a treadmill, the Bruce protocol is most commonly used; however, it has the disadvantage of a large interstage workload increment between stages that can make estimation of peak VO2 less accurate.13 Our center performed exercise tests using only the Bruce ramp protocol. This protocol is better able to overcome sudden and rapid work rate changes, and can more accurately assess exercise capacity than other exercise protocols.15 In particular, for HF reduced systolic function or IHD with large myocardial fibrosis, a sudden increment in workload may be associated with increased risk of sudden hypotension or ventricular arrhythmia. Although few studies compared risks of the Bruce ramp protocol with other exercise protocols, we believe that using the Bruce ramp protocol was a potential factor contributing to the lower incidence of adverse events observed in our population.
Percutaneous valvular procedures, such as transcatheter aortic valve replacement (TAVR) or percutaneous mitral balloon valvuloplasty, have been performed in even very old patients. In particular, TAVR procedure use has increased exponentially in elderly patients with severe aortic stenosis, with technical advancement of the procedure and improvements in performance.16 Evaluating functional capacity precisely is important for determining if surgery is feasible in elderly patients with VHD. The tendency has been increasingly aggressive treatment for elderly patients with VHD. Our findings support that CPET should be implemented in elderly patients with moderate to severe VHD for assessment of functional capacity. Physicians are also concerned about adverse events of CPET for people with HCMP. In HCMP with hemodynamic LVOT obstruction, exercise testing especially poses a risk of arrhythmia or hemodynamic collapse.6 However, previous studies showed the safety of CPET in HCMP1718 and our data support this safety, with no adverse events occurring in people with HCMP. As CPET can provide important prognostic information about patients with HCMP,17 it is considered a feasible test for elderly patients.
In Korea, there is a lack of standard data on the exercise capacity of elderly population with CV diseases. Our results showed that elderly Korean patients with CV diseases had an exercise capacity of about 6.1 METs, decreasing proportionally with increasing age. Women had significantly poorer exercise capacity than men. Several parameters such as the mean age, peak VO2, and METs were comparable in our study with previous studies19 or were higher than in other studies performed in older patients with CV diseases.814 Octogenarian men in our population had 5.0±1.3 METs of exercise capacity, similar to American men older than 80 years without major CV disease.20 Considering our population had definite CV diseases compared to American patients in the abovementioned study, we suggest that our population had a relatively good exercise capacity. Therefore, our results meaningfully support that elderly Korean patients with CV diseases can perform active cardiac rehabilitation.
We found that leg pain was the second most common cause for termination of tests with increasing proportions according to age. Another report also showed that leg fatigue was the second most common cause of termination in elderly Korean people with coronary artery disease.21 Musculoskeletal factors, such as sarcopenia or joint disorders, are commonly associated with the elderly patients, and sarcopenia is closely associated with cardiorespiratory fitness in community-dwelling elderly Koreans.22 In patients with CV diseases, especially in those with HF, most show dyspnea on exercise. The tended to refrain from physical activity that worsens sarcopenia; therefore, sarcopenia may have a greater effect on exercise capacity or quality of life than in elderly people without CV diseases. In addition, joint problems or back pain, and a deteriorating sense of balance can limit the accurate assessment of functional capacity and possibly increase the risk of falling in elderly patients.23 Although musculoskeletal or autonomic function deficiencies due to aging are unavoidable, additional efforts are required to ensure exercise tests can be performed safely in elderly patients with limitations on physical activity. Novel equipment such as bicycles tailored specifically to this population that allow exercising in a recumbent or supine position may be a useful modality to reduce these limitations.24
Our study had several limitations. First, it was a retrospective, single, tertiary referral center study. Second, we did not quantitatively assess pulmonary function. Deteriorated pulmonary function may have affected the CPET results. Third, generalizing CPET values is difficult due to variations in CV disease and its severity. Fourth, since all patients had CPET using only the Bruce ramp protocol, there was a limitation in representing the safety of all CPET modalities. Fifth, we could not evaluate the daily physical activity of patients, including leg muscle strength or power, which may have affected exercise capacity. Sixth, we did not analyze safety of CPET according to each CV disease.
However, to our knowledge, this is the first large-scale study to assess the safety and characteristics of CPET in elderly Korean patients with CV diseases. Considering our sample size, this study presents meaningful characteristics of CPET in elderly Korean patients with CV diseases.
In conclusion, CPET is a relatively safe and useful modality to assess exercise capacity in elderly Korean patients with CV diseases. Further studies are warranted to validate the application of CPET in this population.

 XML Download
XML Download