

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent evidence has demonstrated the beneficial effect of exercise based cardiac rehabilitation (CR) in improving clinical outcomes and secondary prevention for acute myocardial infarction.123 Thus, current practical guidelines recommend referral to CR with exercise training for patients with myocardial infarction or chronic stable angina. However, very little research has been conducted to clarify the impact of exercise training on clinical outcomes in patients with ST-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) with drug-eluting stents (DESs) implantation on the infarct-related artery. Moreover, several studies have reported that only 22–30% of patients with myocardial infarction participate in CR programs.456 Since guidelines recommend that patient counseling to maximize adherence to evidence-based post-STEMI treatment should begin during the early phase of hospitalization, occur intensively at discharge, and continue at follow-up visits, underutilization of exercise-based CR, especially in patients with myocardial infarction, may deprive an important therapy in these high-risk patients. Thus, it is important to determine who can benefit from CR with ET in patients with myocardial infarction.
In the present study, we aimed 1) to evaluate whether exercise-based CR improves major adverse cardiovascular events (MACEs) in patients with STEMI undergoing primary PCI in the current DES era and 2) to find subsets of patients that would benefit most from exercise-based CR.
MATERIALS AND METHODS
A total of 265 patients who underwent primary PCI for STEMI between 2009 and 2014 were screened. All patients were encouraged to participate in CR with an exercise program unless they had third degree atrioventricular block, severe aortic stenosis, systolic blood pressure above 200 mm Hg at rest, diastolic blood pressure above 110 mm Hg at rest, pericarditis, uncontrolled tachycardia, exercise induced malignant ventricular arrhythmia, acute systemic illness, skeletal vascular disease, or acute metabolic disorders. The patients who were unwilling to provide informed consent to the exercise training program were also excluded. Finally, a total of 254 STEMI patients were enrolled in this study, and 76 of 254 STEMI patients (30%) participated in the exercise-based CR program. Of 178 nonparticipants, 120 patients refused to participate in the CR program, and 58 patients did not complete the planned CR program. The Institutional Review Board of Sanggye Paik Hospital approved this study. The requirement for informed consent was waived because of the retrospective nature of the study (IRB number: 2019-01-003-001, IRB institution: Sanggye Paik hospital, Inje University).
Participation in the CR program was defined as commencement of a CR session starting within 4 weeks of the index PCI and completion of phase 2 supervised exercise in the hospital for a period of 6–8 weeks and maintenance of community-based self-managed exercise over 9 months.7 Cardiorespiratory capacity was measured twice by a symptom-limited treadmill exercise test under the protocol of modified Bruce before the commencement and at the end of the phase 2 supervised exercise training. Maximal oxygen uptake (VO2max) was defined as the highest valuce or the plaeteau of directly measured oxygen consumption using a respiratory gas analyzer (QMC, Quinton Intrument CO., Boston, MA, USA). The exercise test was supervised by experienced physicians and ECG monitoring was conducted throughout the test. The exercise program included a 10-minute warm-up, a 40-minute aerobic exercise on a treadmill, and a 10-minute cool-down phase. Exercise intensity in the first stage was gradually increased from 50% to 80% of VO2max determined by the exercise test. After the 6 weeks of supervised exercise, community-based and self-managed exercise was performed according to the reassessed cardiorespiratory capacity. Patients were required to exercise at a local fitness center and maintain aerobic exercise on a treadmill in a same manner. Every exercise training session should be composed of 1 hour, and patients were required to exercise three times a week. Adherence to exercise was monitored every month at an outpatient clinic.7
MACE was defined as the composite of death, myocardial infarction, and revascularization. Clinical events were defined according to the Academic Research Consortium and an expert consensus document that defined the third universal definition for myocardial infarction.89 All deaths were considered cardiac related unless an unequivocal non-cardiac cause could be established.8 During follow up, myocardial infarction was defined by the following parameters: the presence of clinical symptoms, ECG changes, or abnormal imaging findings indicative of myocardial infarction and an increase in creatine kinase myocardial band fraction above the upper normal limits or an increase in troponin-T/troponin-I above the 99th percentile of the upper normal limit. Any revascularization was defined as a repeat PCI or bypass surgery.9
Statistical analyses were performed using IBM SPSS, version 19.0 (IBM Corp., Armonk, NY, USA). Categorical variables are reported as numbers and percentages. Continuous variables are reported as a mean and SD. Cumulative MACEs at 1 year and 3 year were calculated using Kaplan-Meier estimates and compared using the log-rank test. Although patients could experience more than one MACE component, each patient was assessed until the occurrence of the first event during analysis. Also, factors associated with MACE were determined by performing a univariable analysis using Cox proportional hazards regression with all variables listed in Tables 1 and 2. All variables achieving a p value <0.10 in univariate analysis were entered using the enter method into a multivariate analysis model. Subgroup analyses were performed according to clinical and angiographic subgroups. All tests were two-sided, and a p value <0.05 was considered statistically significant.
RESULTS
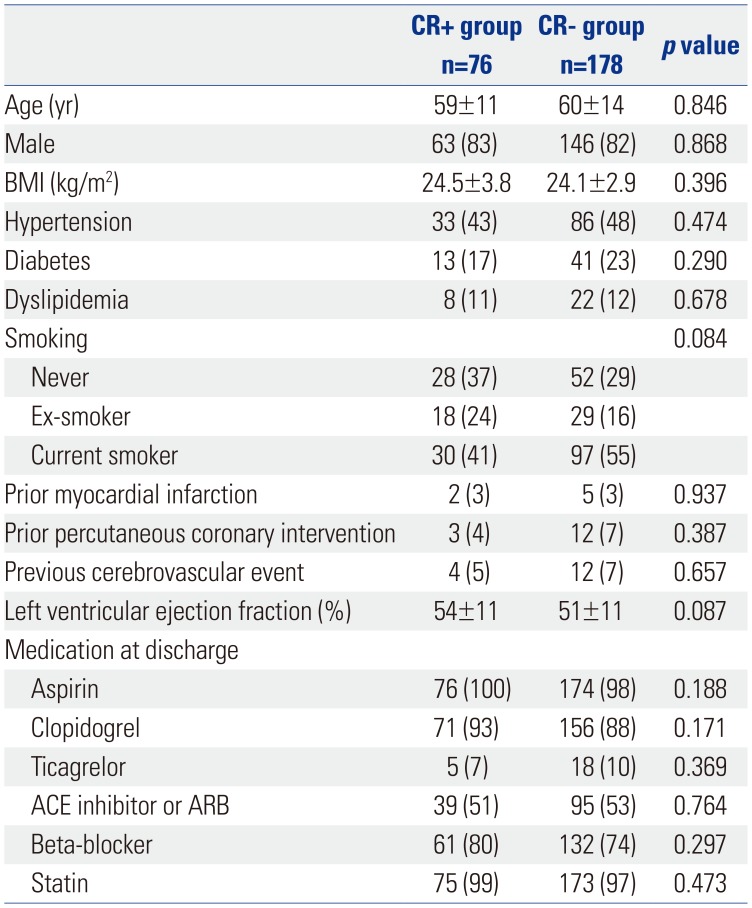
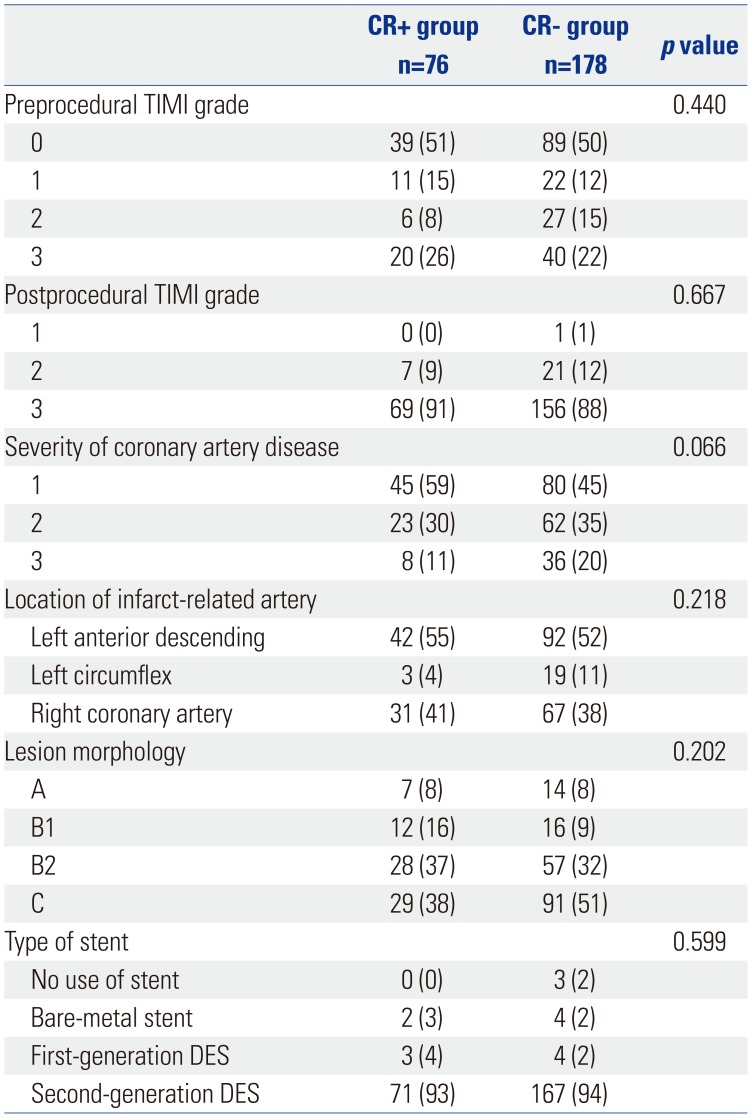
Of 254 STEMI patients who were eligible for the exercise program, 76 patients (30%) participated in CR with an exercise program the during study period (CR+ group). Nonparticipants to CR (178 of 254 STEMI patients, CR− group) comprised those who were under standard medical care for myocardial infarction, including medication, abstinence from smoking, and diet modification during study period. Baseline clinical characteristics according to the CR group are presented in Table 1. There were no significant differences in baseline characteristics, including age, sex, body mass index, diabetes, hypertension, and left ventricular ejection fraction. Angiographic characteristics are presented in Table 2. There were no significant differences in initial thrombolysis in myocardial infarction (TIMI) grade, severity of coronary artery disease, location of infarct-related artery, and lesion morphology. Among 254 patients, 238 (94%) patients received second-generation DESs.
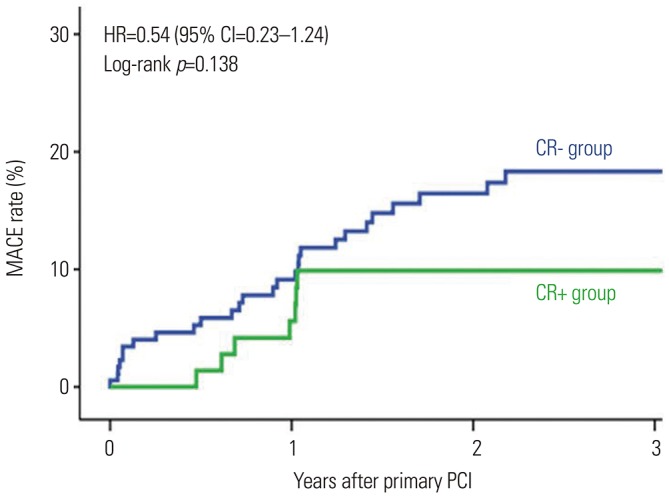
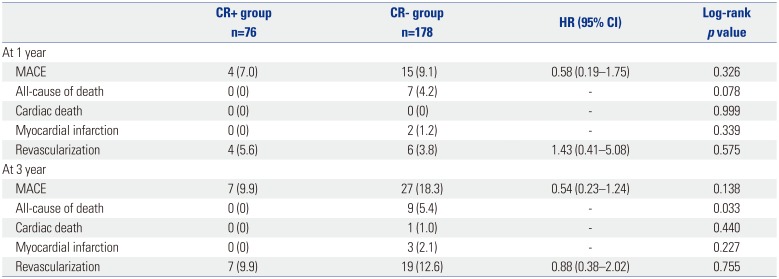
Clinical outcomes are presented in Table 3. During a median follow up of 943 days (interquartile range: 514–1096 days), MACEs occurred in 37 patients. At 1 year, the MACEs did not differ between groups [7.0% vs. 9.1%, hazard ratio (HR)=0.58, 95% confidence interval (CI)=0.19–1.75, p=0.326]. At 3 years, although not statistically significant, the CR+ group had fewer MACEs than the CR− group, (9.9% vs. 18.3%, HR=0.54, 95% CI=0.23–1.24, p=0.138) (Fig. 1). As for clinical outcomes, all-cause death at 3 years was significantly lower in the CR+ group than in the CR− group (0% vs. 5.4%, p=0.033). Cardiac death, myocardial infarction, and any revascularization were not different between groups. Univariable and multivariable analyses for MACE are also presented in Supplementary Table 1 (only online).
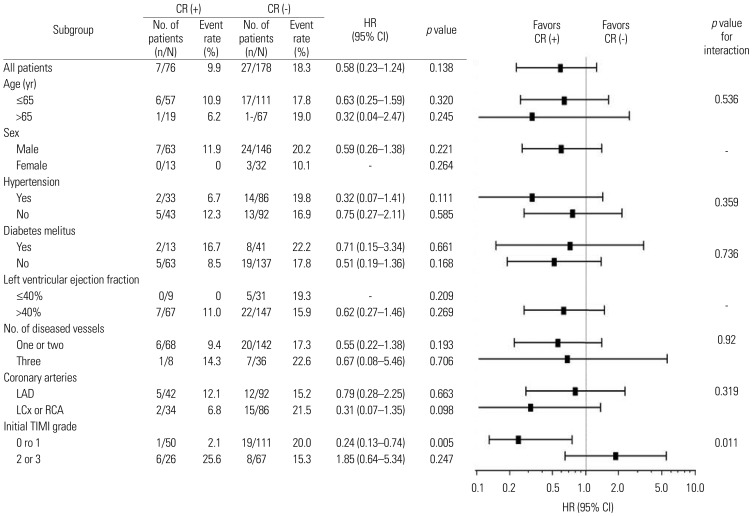
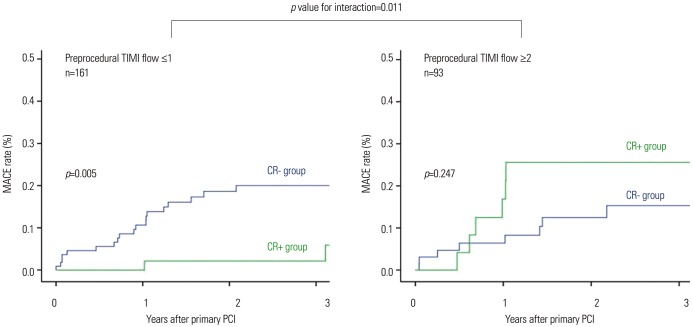
In subgroup analysis to identify patients who would benefit from CR, we found a significant interaction between the CR group and preprocedural TIMI flow (Fig. 2). The CR+ group had significantly fewer MACEs in the subgroup of patients with lower TIMI flow (TIMI flow ≤1, n=161) than in the subgroup of patients with higher TIMI flow (TIMI flow ≥2, n=93) (p-value for interaction=0.011). Also, among patients with low TIMI flow (TIMI flow ≤1), the CR+ group had significantly fewer MACEs than the CR− group (p=0.005) (Fig. 3). However, among patients with higher TIMI flow (TIMI flow ≥2), MACEs were not different between groups (p=0.247) (Fig. 3). There were no significant differences in baseline characteristics according to preprocedural TIMI flow (Supplementary Table 2, only online).
DISCUSSION
The main findings of the present study are that, although the CR+ group only exhibited a lower tendency for MACEs than the CR− group after 3 years, there was a significant interaction in subgroup analysis according to the CR group and preprocedural TIMI flow. The CR+ group had significantly lower MACE than the CR− group, particularly in patients with low TIMI flow, during primary PCI, whereas MACE was not different between groups among patients with higher TIMI flow, suggesting that CR with exercise training would be most clinically beneficial to patients with low preprocedural TIMI flow during primary PCI for STEMI in the current DES era.
Much evidence has demonstrated the beneficial effect of CR including regular exercise on the improvement of clinical outcomes in patients with coronary heart disease.123 In 2004, Taylor, et al.1 reported that CR was associated with a 20% reduction in all-cause mortality and a 25% reduction in cardiac death from a meta-analysis of randomized trials of ischemic heart disease. Also, in 2004, Hambrecht, et al.3 reported that a 12-month program of regular physical exercise in patients with stable coronary artery disease showed superior event-free survival and exercise capacity at lower costs to those who were treated with PCI. Also, recent data have demonstrated an inverse relationship between CR program participation and adverse cardiovascular events in an analysis of Medicare claims data, including 30161 patients with coronary artery disease who attended at least one CR session. After 4 years of follow up, patients who attended 36 sessions had a 14% lower risk of death and a 12% lower risk of myocardial infarction than those who attended 24 sessions; a 22% lower risk of death and a 23% lower risk of myocardial infarction than those who attended 12 sessions; and a 47% lower risk of death and a 31% lower risk of myocardial infarction than those who attended one session.10 Therefore, recent major guidelines from the American Heart Association and the American College of Cardiology Foundation regarding the management and prevention of coronary heart disease provide a class 1 level recommendation (i.e., procedure/treatment should be performed/administered) for referral to a CR program for patients with recent myocardial infarction or acute coronary syndrome, chronic stable angina, or heart failure or for patients following coronary artery bypass surgery or percutaneous coronary intervention.1112 In line with previous findings, the CR+ group had fewer MACEs than the CR− group at 3 years, although the difference was not statistically significant (9.9% vs. 18.3%, HR=0.54, p=0.122). However, different from previous studies, which were mainly performed in the bare-metal stents era, the majority of the patients analyzed in our study was treated with second-generation DESs: of note, 94% of the patients received a second-generation DES. Although the advent of DES significantly lowered rates of in-stent restenosis and the need of target-lesion revascularization, compared to bare-metal stents, increased rates of stent thrombosis emerged as another concern, particularly for first-generation DESs. However, even in patients with STEMI, steady improvements in outcomes have been realized with the evolution from bare-metal stent to first-generation and now second-generation DES, with the most favorable safety and efficacy profile.131415 Thus, these significant reductions in device-related MACEs with the use of second-generation DES might mitigate the clinical benefit of CR in the present study. Also, the small number of patients with a relatively short-term follow up in the present study may account for the lack of statistical significance.
Despite the importance of participation in a CR program after myocardial infarction, participation rates have been reported as only 22–30% according to recent studies.456 In the present study, among 254 STEMI patients who were discharged after primary PCI, 76 patients (30%) participated in the CR program including exercise training. The major reasons of the nonparticipants were refusal to enroll the program. Therefore, it may be important to identify patients who would benefit from CR in patients with myocardial infarction. Although other clinical or procedural characteristics did not show a significant interaction in subgroup analysis, we found that there was a significant interaction in subgroup analysis according to CR group and preprocedural TIMI flow. According to a recent study, during primary PCI, low preprocedural TIMI flow was reversely associated with myocardial injury and was an independent predictor of myocardial damage assessed by cardiac magnetic resonance.16 Also, patients undergoing primary PCI in whom TIMI-3 flow is present before angioplasty present with greater clinical and angiographic evidence of myocardial salvage, are less likely to develop complications related to left ventricular failure, and have improved early and late survival.17 In this sense, for patients with low preprocedural TIMI flow, CR could be more beneficial, compared to those with high preprocedural TIMI flow.
This study has several limitations. First, this study was a retrospective study of single-center data from a relatively small group of patients. Notwithstanding, we included patients with STEMI undergoing primary PCI in the current DES era, and second-generation DESs were used in 94%. Second, our study might be under-powered because of low event rates. Third, a longer follow up is needed.
In conclusion, CR including exercise training was associated with fewer MACEs, particularly among patients with lower preprocedural TIMI flow, during primary PCI for STEMI in the current DES era.
 XML Download
XML Download