

 PDF
PDF Citation
Citation Print
Print



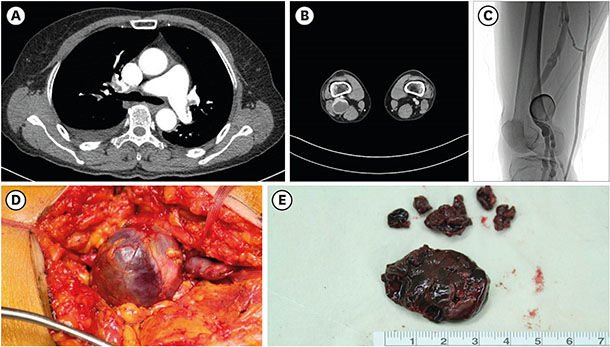
A 67-year-old woman presented with chest pain with shortness of breath on walking in July 2014. The coronary angiogram and echocardiogram revealed no significant finding. On the night of admission, recurrent syncope with transient shock was observed so we checked the computed tomography (CT) angiogram for evaluation of pulmonary embolism (PE). A CT angiogram revealed multiple, bilateral filling defects diagnostic of multiple bilateral pulmonary emboli (Fig. 1A) and enlargement of right popliteal vein (Fig. 1B). A lower extremity venogram revealed a right saccular popliteal venous aneurysm (PVA) that measured 3.5 cm in diameter and was filled with floating thrombus (Fig. 1C). Laboratory tests revealed no evidence of hypercoagulable state. A preoperative inferior vena cava filter was inserted into infrarenal inferior vena cava and the patient was anticoagulated with heparin and warfarin for the preoperative period. Two months later, a lateral tangential aneurysmectomy was performed to prevent a recurrence of PE on posterior approach via an S-shaped incision to the popliteal fossa (Fig. 1D). The lateral venorrhaphy was primarily repaired. The opened aneurysm sac was filled with organizing thrombi and observed intima necrosis with medial hypertrophy (Fig. 1E). The patient was anticoagulated for 1 year. The patient has been asymptomatic for 1 year with no sign of deep venous insufficiency. A CT angiogram revealed patent repair with no evidence of deep venous thrombosis. PVAs are extremely rare but can make PE. Common symptoms of PE are chest pain and dyspnea. Syncope is an unusual symptom for PE and PVA.12 Despite the small size of the PVA, the high risk of thromboembolic complication associated with the symptomatic nature of PVA requires strong consideration for surgical management.3 We report an extremely rare case of large PVA successfully treated with surgical and anticoagulant therapy in a patient with the non-specific symptom of syncope. The images are published under agreement of the patient.

 XML Download
XML Download