

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since Blackwood first described atlanto-occipital dislocation (AOD) in 1908,3) it was long held to be a rare entity in comparison with other cervical spine injuries.1) The initial trauma is commonly the result of a high-speed motor vehicle or pedestrian collision.1) Many of the patients with traumatic AOD will die immediately or within the first hours after injury due to vascular lesion mainly at the level of the vertebral artery17) or cervical medullary injury with asphyxia secondary to phrenic or bulbar nerve palsy.17) Nowadays AOD is being increasingly recognized as a potentially survivable injury as a result of improved prehospital management, increased awareness, and more aggressive and quick management.211) The purpose of this fatal case report is to review the current concepts about AOD ranging from subtle to fatal condition.
CASE REPORT
A 48-year-old male was hit by a dump truck. On arrival of the rescue team, he did not respond the light reflex with 5 mm dilated both pupil. He had no respiration and no carotid pulsation. He had a Glasgow Coma Scale (GCS) of 3 points. He had external 2 cm laceration at right forehead and 5 cm laceration at left parietal convexity. Submental contusion, diffuse facial and neck swelling, oral bleeding and both ear bleeding were detected. At the scene, his neck was immobilized and his airway was kept by laryngeal mask airway device. He received nonstop cardiopulmonary resuscitation throughout pre-hospital transport. Following successful resuscitation and intubation, the blood pressure and heart rate recovered by inotropic and vasopressor agents but self-respiration failed to recover. His body temperature was 35°C and the GCS and papillary light reflex did not improve. After radiological work-up, we found AOD with mixed type I and II according to Traynelis et al.20) (FIGURE 1). There was not any severe injury in his internal organs within thoracic and abdomino-pelvic cavity. He had also deep laceration at his left foot. Initial lateral cervical X-ray overtly revealed AOD. Mandibular fracture was also detected. Brain computed tomography (CT) showed subarachnoid hemorrhage within right Sylvian fissure, interpeduncular cisterns, quadrigeminal cisterns and craniovertebral junction, and intraventricular hemorrhage in both lateral ventricles. Brain and neck 3 dimensional (3D) CT angiography well visualized AOD as well as neurovascular injury (FIGURES 2, 3, 4). He was then transferred to the intensive care unit, where he died of severe lesion in the transition from medulla oblongata to spinal cord and left vertebral artery dissection 26 hours after the fatal pedestrian collision.
FIGURE 1
Initial (A) and 8 hours follow-up (B) cervical X-ray lateral views show atlanto-occipital dislocation and instability. These images (A, B) show mixed type I and II according to Traynelis et al.20)
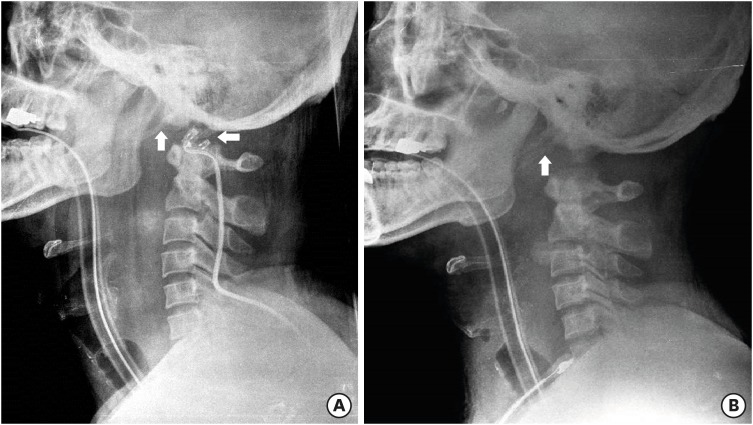
FIGURE 2
Three dimensional computed tomography angiography of axial (C1) and midsagittal reconstruction view show atlanto-occipital dislocation and associated lesion of medulla oblongata and upper cervical cord. (A) Axial view shows double contour of occipital condyles in front of anterior arch of atlas. Axial view shows the level of midsagittal view (B). (B) Midsagittal view shows the huge hematoma at retropharyngeal and retropharyngeal space, around medullar oblongata and upper cervical cord, thinning of medulla and anterior dislocation of foramen magnum.
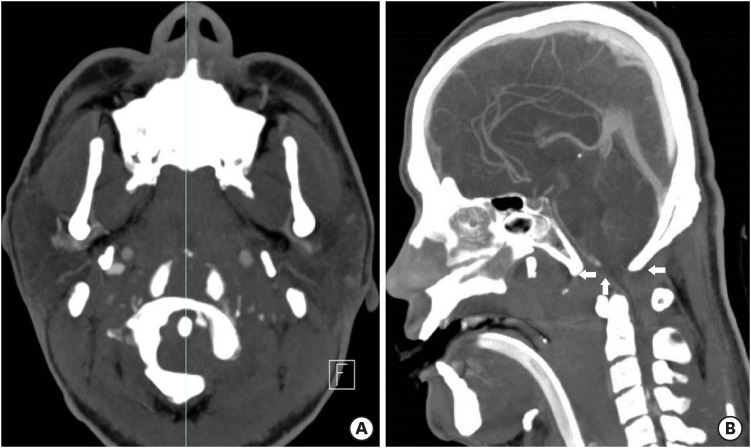
FIGURE 3
Sagittally reformatted computed tomography images show dislocation of the right (A) and left (B) atlanto-occipital joints.
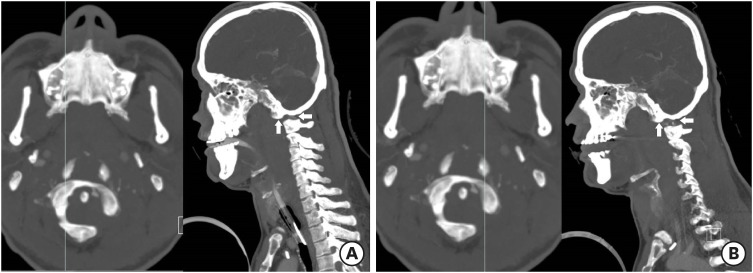
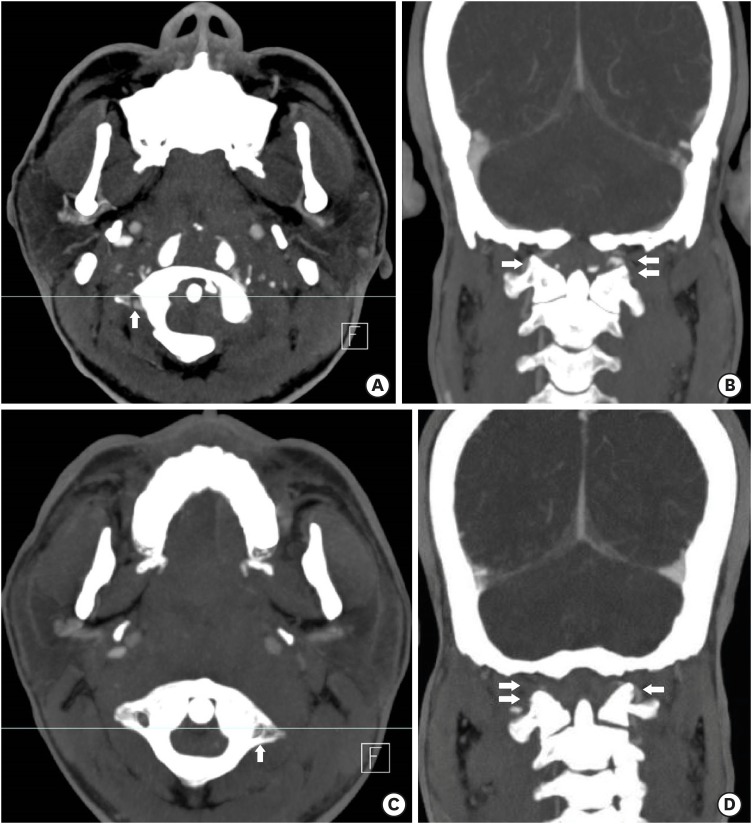
FIGURE 4
Three dimensional computed tomography angiography of axial (C1) and sagittal reconstruction views show atlanto-occipital dislocation and associated lesion of left vertebral artery at C1 level. (A) Axial view showing the level of coronal section (B) at right transverse foramen of atalas. Axial view shows double contour of occipital condyles in front of anterior arch of atlas due to anterior dislocation. (B) Coronal reconstruction view at right transverse foramen of atlas shows the continuity of right vertebral artery at C1 level. (C) Axial view showing the level of coronal section (D) at left transverse foramen of atalas. (D) Coronal reconstruction view at left transverse foramen of atlas shows the loss of continuity of left vertebral artery at C1 level revealing dissection of left vertebral artery.
DISCUSSION
AOD has been identified in 6–10% of fatal cervical spine injuries from any mechanism.16) AOD is now estimated to cause 8% to 35% of motor vehicle fatalities.156)Although AOD may be overtly obvious on plain films with severe dislocation, in survivors the radiographic diagnosis is often more subtle.1314) AOD should be suspected in any patient involved in a high speed motor vehicle or pedestrian collision.12561819) Once suspected, proper imaging and appropriate management of these once fatal injuries can improve survival and neurologic outcome.2610111219)
AOD is a highly unstable craniocervical injury, resulting from damage to ligaments and/or bony structures connecting the skull to the cervical spine.318) Brainstem and upper cervical spinal cord injury affects significant neurological morbidity and mortality. Modern case reports, however, have documented improved neurological outcomes, likely as a result of improved prehospital management, earlier diagnosis and surgical stabilization.2101116)
Airway management is one of the major concerns of AOD. During airway intervention and positioning at the scene, there is a potential risk of neurovascular injury due to near-full extension of the atlanto-occipital joint. Either it kills or it saves. The clinical relevance of this is unknown despite many studies in alive and cadaveric models of normal and injured cervical spines.9) There is neither general consensus nor clinical practice guideline to manage the airway in patients with cervical spine instability. In spite of these, clinicians should do their best efforts to keep airway without any additional neurovascular injury in patients with cervical spine instability.
Over the years, many different methods have been developed to diagnose AOD. All methods seek to assess for the instability of the craniovertebral junction. These include the Traynelis et al.20) classification (FIGURE 5), Powers' ratio,17) X-line method,12) basion-dens interval and basion-axis interval (i.e., Harris lines),78) occipital condyle-C1 interval41314) and the range of motion measured by the hard palate.15)
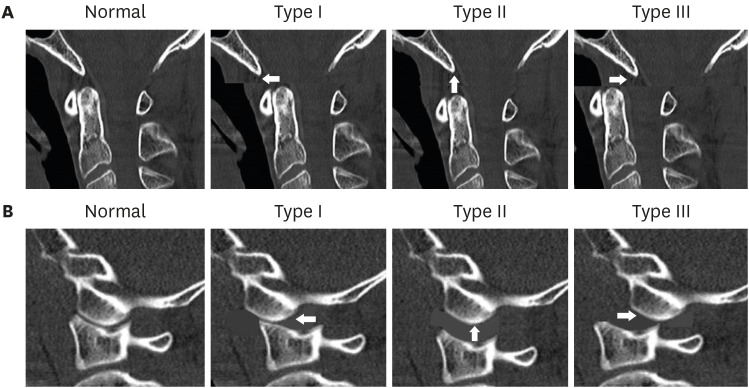
FIGURE 5
The Traynelis et al.20) classification. type I (anterior dislocation), type II (longitudinal separation), and type III (posterior dislocation). (A) Midsagittal plane views show the relation of the basion, the posterior arch of C1, the opisthion and the anterior arch of the atlas. (B) Parasagittal plane views show the relation of the occipital condyle and the superior articular surface of lateral mass for occipital condyle.
The diversity of these methods and measurement techniques may cause confusion among clinicians. There is still no gold standard technique to diagnose AOD and clinicians are prone to misdiagnose AOD in a subtle clinical presentation. Hall et al.6) recommend utilizing at least 2 complementary methods to help compensate for the shortcomings of any single method.6) Also, it is important to diagnose AOD correctly that the patient's clinical presentation and suspected mechanism of injury should be considered, since no radiographic measures can completely rule out the diagnosis.5619)
Treatment of AOD begins at the scene.619) Fatal AOD is now transported to the emergency room alive. It is due to increased sophistication in on-scene resuscitation and rapid transportation by an advanced emergency rescue system. Nonstop cardiopulmonary resuscitation throughout pre-hospital transport is essential. Following successful resuscitation and intubation is mandatory. Cervical immobilization should be started at the trauma scene with cardiorespiratory management.19) In the emergency department, early diagnosis is essential with early clinical suspicion for AOD in high speed trauma patients. Proper knowledge of 3D CT angiography is essential to detect the fatal arterial dissection and the subtle patients with AOD which are most likely unstable and need surgical fixation.
There is a general consensus on AOD management in adults. In the absence of any medullary compression, 2 stage occipitocervical fixation is recommended. Halo vest immobilization should be performed, followed by internal occipitocervical fixation and fusion.5619) Cervical traction is contraindicated, since it is associated with a 10% risk of neurological deterioration.19) In children, early occipitocervical fusion is recommended.2) Halo immobilization and cervical traction are contraindicated in the management of AOD in children because of the risk of displacement of the injured occipitocervical joint.2)
CONCLUSION
This report reminds us that AOD patients have been more open transported to the emergency room alive by the improved prehospital emergency rescue system. The diagnosis is difficult if AOD is subtle. Clinicians should keep in mind that thorough radiologic studies with early clinical suspicion could save AOD alive without neurologic deterioration.
 XML Download
XML Download