

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Resident working hours are closely related to patient safety [1]. Long working hours and overtime are known to be associated with increased medical errors from residents [23]. Following the Libby Zion accident in New York State in 1984, interest in the working environment of residents has increased [4]. Currently, many countries have exerted limitations in resident working hours by law. In the United States, the Accreditation Council for Graduate Medical Education (ACGME) is leading the improvement in resident working environment [5]. Europe and Canada have also implemented resident working hour restrictions [6].
Until recently, there were no guidelines on working hours for residents in Korea, and many residents worked more than 100 hours a week [7]. With the adoption of resident regulations in the US and Europe, interest in resident work environment also increased in Korea. The “resident special law” (resident training environment improvement program) started in 2015 as an autonomous recommendation and became a system that included legal regulations in 2017. According to this system, residents cannot work more than 88 hours a week for an average of four weeks, including educational training time. Residents are also banned from night duties for more than 3 days a week or for more than 36 consecutive hours of work. Various resident work schedules have been introduced by different institutions to comply with these working hour regulations, but many have been found to be impractical, and the best working model has not been agreed or standardized.
A night float (NF) system involves a separate team of residents that work on night duties only for a certain period of time and then rotate with other residents on day duties. This system is commonly used in other countries to tackle the issue of restricted working hours as well as limited resident numbers, and this system was temporarily adopted by the Department of Surgery at Seoul National University Bundang Hospital. In this study, we evaluate the superiority of this NF system in comparison to the pre-existing traditional night on-call (NO) system in terms of safety and efficacy, and the preference of this system by the associated medical staff. To our knowledge, this is the first report of the NF system experience in Korea.
METHODS
Patients
We collected patient data from March to September 2016 for the NO system and from March to September 2017 for the NF system at Seoul National University Bundang Hospital. All patients admitted for surgery and patients contacted for surgical consultation from the emergency room (ER) were included. Approximately 150,000 clinical patient data were obtained from electronic medical records and big data analysis was performed. For ward patients, we investigated several parameters including age, sex, vital signs (systolic and diastolic blood pressures, heart rate, respiratory rate), nonintended transfers to the intensive care unit (ICU), major postoperative complications (postoperative bleeding, anastomosis site leakage, wound evisceration, small bowel injury, postoperative foreign body removal), and mortality rate. For ER patients, age, sex, and the time to response by residents for calls from the ER were collected. The time to response was defined as the time taken from contact to input of either medical orders or contact notes in the electronic medical record. The time taken was divided into 2-hour intervals and analyzed in detail. This retrospective cohort study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (B-1712-441-106) and exempted from the informed consent.
NO system
Under the traditional NO system, all residents worked on regular day duties from 7:00 AM to 7:00 PM, and around 30% continued to work on night duty from 7:00 PM to 7:00 AM the next day (Fig. 1). These residents continued to work immediately on the next day for their full day duty without any break (36 hours of continuous work). This was the traditional working system used until 2016.
NF system
On March 2017, a new system of NF was introduced in an attempt to systematically match the 88-hour working regulations for residents implemented by the Korean government. Under this system, only 70% of the residents worked on day duty (Fig. 1), while the remaining 30% of residents worked on night duty. Residents on night duty worked for 12 hours at night for 5 days a week (on weekdays only) and for a total of 1 month. Rotations were done on a monthly basis so that no resident would be on night duty for 2 consecutive months. Residents in the NF system had the advantage of shortened working hours per week as well as reduction in continuous working hours.
Questionnaire
A survey was performed in June 2018 to physicians (residents and staffs) and nurses who had directly experienced both the NO and NF systems. A questionnaire was distributed in paper form which included questions related to satisfaction and safety/efficacy parameters under both system and were finally asked to choose between both systems if it were to be permanently implemented in the future.
Statistical analysis
Continuous variables were expressed as means ± standard deviations. Categorical variables were expressed as number and percentage. Both groups were compared in terms of continuous and categorical variables using Student t-test and Pearson chi-square test, respectively. Differences were considered significant at P-values of <0.05. All statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Ward patients
Under the NO and NF systems, a total of 3,900 and 3,726 patients, respectively were admitted to the department of surgery. The mean age of the patients was 54.7 ± 17.5 and 55.2 ± 17.9 years (P = 0.204), and the male ratio was 47.8% and 49.3%, respectively (P = 0.181). Table 1 shows the changes in vital signs, transfers to the ICU, morbidity rates, and mortality rates in ward patients under the NO and NF systems. There were no differences in blood pressure change and ICU transfers between the 2 groups. Postoperative bleeding was significantly higher in the NO system compared to the NF system (0.5% vs. 0.2%, P = 0.031). Other major complications such as anastomosis site leakage (P = 0.575), wound evisceration (P = 0.283), small bowel injury (P = 0.197), and postoperative foreign body removal (P = 0.306) were not statistically significant between the two systems. There was also no significant difference in the mortality rate between the 2 systems (P = 0.402).
ER patients
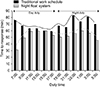
Under the NO and NF systems, a total of 1,462 and 1,354 patients respectively, visited the ER and were contacted for surgical consultation. The mean age of the patients was 50.8 ± 22.1 and 52.8 ± 22.1 years (P = 0.016), and the proportion of male patients was 59.2% and 56.4%, respectively (P = 0.141). Table 2 shows the time required for ER patients to receive surgical attention under the NO and NF systems. The overall time taken was significantly shorter in the NF system (54.5 ± 70.7 minutes) than the NO system (66.8 ± 83.8 minutes) (P ≤ 0.001). This difference was mostly noticed during the night duties, where the time interval was significantly shorter in the NF system (53.1 ± 70.5 minutes) compared to the NO system (72.2 ± 80.0 minutes) (P < 0.001), while during the day duty the time interval was not so different (55.5 ± 70.9 minutes vs. 62.8 ± 86.3, minutes respectively, P = 0.064). Fig. 2 shows a visual representation of the time required for surgical care from the initial time of contact for both NO and NF systems. When analyzed on a 2-hour interval basis, it can be visualized that the response by the NF team was significantly faster than the NO team for all time-points at night, as well as the early morning (7 AM) period.
Questionnaire
The results of the questionnaire-based medical staff survey are shown in Fig. 3. The physicians' subjective preferences were the NF system (78.6%), NO system (7.1%), or both (14.3%), and the response as to which system was more beneficial to the hospital was the NF system (90.4%), NO system (4.8%), or both (4.8%). The details of the 42 physicians participating in the questionnaire were as follows: 19 residents and 23 board-certified staff. Of the 3 respondents who answered that the NO system would be beneficial, there were 2 residents and one staff. The 2 residents that supported the NO system expressed their concern that the proportion of resident education would decrease if the system was changed. The nurses' subjective preferences were the NF system (85.7%), NO system (5.7%), or both (8.6%), while their opinion in terms of hospital benefit was the NF system (91.4%), NO system (2.9%), both (4.3%) and none (1.4%).
DISCUSSION
The 1984 death of patient Libby Zion in the United States was an incident that led to increased public awareness about the working conditions of residents, and thereafter a law on resident working hours was put into effect [4]. Studies have reported the association between cumulative fatigue and poor cognitive function [89], and sleep deprivation has been found to negatively affect management in emergent situations [10]. To reflect this, in 2003, the ACGME already set an 80-hour workweek limit for 4 weeks, and the same agency added a 16-hour continuous work restriction in 2011 [11]. Accordingly, many institutions have introduced a NF system in order to comply with the working hours of residents [1213].
In Korea, a 9-year-old child treated with chemotherapy for leukemia in 2010 died from a medical error [14]. Intravenous vincristine was accidentally injected into the child's spinal canal and died 10 days later. Since then, medical accidents and patient safety have been extensively investigated. During the course of the investigation, similar events in the past were also discovered, leading to an increased interest in patient safety [15]. Subsequently, the so-called ‘Jonghyun law’ for patient safety came into force in 2016. In addition, resident working time restrictions were also discussed, and from 2017 onwards, residents in Korea are not allowed by law to work for more than 88 hours a week, including educational training hours. Our institution discussed the introduction of a NF system with the aim of changing the work schedule of residents in a systematic way. Until 2017, there had been no reports of any surgical department having implemented a NF system in Korea, and therefore a NF system was designed and temporarily implemented.
Under a traditional NO system, our surgical residents worked an average of more than 100 hours per week. However, with the introduction of the NF system in 2017, the average working time was maintained at 70–80 hours per week. A reduction in working hours has been shown to not only improve quality of life [16], but also allows more time for studying and publishing research papers [17], as well as more time to spend with their families [18]. Regarding concerns related to resident training quality, reports have shown that the number of surgical cases experienced by surgical residents has not changed after implementation of working hour restrictions [19]. The NF system seems to have a positive effect on interns who desire general surgery residents. In fact, preliminary volunteers who wanted to become general surgery residents have decreased by a third since the NF system was discontinued.
Our analysis of patients admitted to the ward in the NO and NF systems have shown no difference in mortality. In addition, morbidity was significantly reduced in terms of postoperative bleeding. This is similar to a previous study in which working restrictions did not affect the morbidity or mortality of severely-ill patients [20]. Additionally, it has been reported that introduction of a NF system does not increase medical errors [21]. Analysis of patients visiting the emergency room showed that the response time was similar during the day time, but under the NF system response was much faster at night, leading to more rapid decision making and treatment. Under the NO system, residents are exposed to sleep deprivation, which has been shown to affect cognitive function [22], but residents working on night duties in the NF system are much more alert and in better physical and mental conditions. We have observed that the response time is shortest during the dawn, when there is little activity in the wards, and response to ER calls can be done more rapidly. This can only be achieved under a NF system, since all residents are awake and alert.
In our medical staff survey, both physicians and nurses preferred the NF system, showing a positive perception about the NF system. Residents were satisfied with the NF system since it relates to an increase in their quality of life [23], while other physicians (nonresidents) and nurses were satisfied with the NF system since it improves resident performance, leading to improvement in their working conditions [24]. Our medical staff also replied that the NF system is benefical for the hospital, since improved resident performance at all times is probably related to better patient management in the wards and the ER. Response to notifications by nurses was more effective under the NF system, leading to rapid action, and there were no concerns regarding confusion during the process of notifications due to a newly implemented system. Two of our residents did express concerns that a change to the NF system might reduce the quality of their education. Further in-depth studies are required to evaluate this, but the quality of education for residents is one of the priorities of their training program and continuous efforts should be made to efficiently improve resident education in a qualitative way.
Despite the positive effects of a NF system in achieving the goal of maintaining resident working hours below 88 hours per week, with improvement in resident performance and probably improved patient safety, we have not been able to implement this system permanently due to legislative issues regarding resident training. The current interpretation of the law does not consider night duty work as resident training and therefore under a NF system, residents may not be able to match their training requirements for board certification. However, the resident working hour restrictions in Korea is currently in effect, and many institutions are having difficulties in achieving this goal. Fellows and junior staffs are compensating by working more hours, but this leads to another population at risk of burnout, and the consequences can be more devastating especially in surgical patients where optimal surgical performance is mostly required by this new at-risk population. Therefore this issue should be approached systematically, and we consider that a NF system is a good way to tackle the problem. More prospective studies may be needed, but our experience has shown a clear benefit of a NF system and we hope that our experience will serve as a good example for legislative modifications and implementation by different institutions in the near future.
In conclusion, our temporary experience of a NF system has shown that resident working hour restrictions can be matched systematically without compromising patient safety. On the contrary, the NF system showed beneficial outcomes in terms of reduced postoperative bleeding for ward patients and faster response to patients in the emergency room leading to prompt management. Associated medical staff were also more satisfied with the NF system and considered this system to be beneficial overall for the hospital.




 XML Download
XML Download