

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Over the past 20 years, considerable progress has been made in the diagnosis and treatment of hepatocellular carcinoma (HCC). Hepatic resection, liver transplantation, radiofrequency ablation, and transcatheter arterial chemoembolization (TACE) have all been used to treat HCC according to clinicopathologic characteristics and hepatic function reserve. Notwithstanding, the optimal management for these patients remains controversial.
Staging systems subdivide patients with cancer into cohorts based on the extent and severity of the disease and predict survival at each level of severity.1 This subdivision enables assignment of a prognosis to the cohort that matches the staging criteria, and it allows clinicians to select the primary and adjuvant therapy. Although many staging and scoring systems have been proposed, there is currently no globally accepted system for assessing HCC due to the extreme heterogeneity of the disease.12 The prognosis and treatment of HCC depend on the patient's underlying liver disease and liver function reserve, in addition to the tumor biology. There are many useful staging systems, such as those of the American Joint Committee on Cancer (AJCC), Okuda, Barcelona Clinic Liver Cancer (BCLC), Cancer of Liver Italian Program (CLIP), modified Union of International Cancer Control (mUICC), Chinese University Prognostic Index (CUPI), and French.34 The Korean Liver Cancer Group has recently adopted the mUICC as the main staging classification system for HCC,45 and they insist that the BCLC and the AJCC systems should also be considered as additional inclusions. Our institute has used the AJCC, the mUICC, and the BCLC staging systems for HCC. In this study, we compared the AJCC and the mUICC systems, assessing data on patients who underwent surgical resection. Here, we present the results of the AJCC (7th and 8th) and the mUICC staging systems applied to patients with HCC, comparing their homogeneity, discriminatory ability, and predictive power for 792 patients who underwent hepatic resection at Ajou University Medical Center in South Korea.
MATERIALS AND METHODS
This study was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and was approved by Ajou University Hospital Institutional Review Board (approval code: AJIRB-MED-MDB-17-204). Between April 1994 and December 2013, 792 consecutive patients were included, and they were followed until June 2017. All patients included in this study underwent surgical resection (liver transplantation excluded). The variables for the demographics of the HCC cohort were sex, age, hepatitis B surface antigen (HBsAg), hepatitis C antibody (Anti-HCV), serum total bilirubin, serum albumin, ICG-R15 (indocyanine green retention rate at 15 minutes), prothrombin time, and alpha-fetoprotein. We added calculated hepatic venous pressure gradient (cHVPG) as a preoperative variable for reserve function of the liver, which we developed recently.6 Peri-operative characteristics included major/minor resection, operative time, bleeding and transfusion during surgery, post-operative complication, in-hospital mortality (within 1 month after surgery), and length of stay after surgery. The pathologic factors were tumor size, number of tumor, portal vein invasion, hepatic vein invasion, bile duct invasion, histologic grade, degree of fibrosis of background liver, and macroscopic intrahepatic metastasis. Tumor size was based on the largest dimension of the tumor specimen. The number of HCCs was defined by the total number of nodules, including intrahepatic metastasis, in the resected specimen. Microvascular invasion and minor vascular invasion were considered vascular invasion of T2 in the 7th and 8th AJCC, and invasion of a major branch (1st order) to a portal vein/ hepatic vein/ hepatic artery was considered major vascular invasion of T3b in the 7th and T4 in the 8th. For the mUICC, major and minor vascular invasion of portal vein, hepatic vein, and bile duct were considered in staging, and microvascular invasion was excluded in staging.
Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) version 23.0 (IBM Corp., Armonk, NY, USA) for most of the analyses. All deaths were counted as events, and living patients were censored to the date of the last follow-up. Disease-free survival was measured from the time of hepatic resection, and recurrence was the endpoint. Overall survival was measured from the time of hepatic resection, and death was the endpoint. Survival curves were constructed using the Kaplan-Meier method and compared using a log-rank test with the Bonferroni correction. In order to identify significant prognostic factors of HCC, univariable and multivariable Cox's regression analyses were performed. The overall survival and disease-free survival models were tested for appropriateness of proportional hazard assumption.
To evaluate homogeneity (smaller differences in survival among patients of the same stage) within each staging system, ‘-2 log likelihood’ was calculated using Cox proportional hazards regression.7 To measure the discriminatory ability (greater differences in survival between each of the stages) of each staging system, the linear trend chi method was used.7 We also applied the Cochran-Armitage test for trend to evaluate linear trends; this was performed with the Statistical Analysis System (SAS), version 9.4 (SAS Institute Inc., Cary, NC, USA).
The ability of the AJCC classification and the mUICC classification to accurately predict survival was verified and compared by cross-validation analysis.89 Patients were randomly divided into a test sample group and a validation sample group. We obtained Pearson's correlation coefficient ‘r’ in the test sample and validation sample, respectively. We compared the predictive accuracy in terms of ‘z’ between the three staging systems, using the Fisher r-to-z transformation method.
We also used SAS for cross-validation analysis. Although this was a similar method to the cross-validation analysis using SPSS, we applied it using SAS for further confirmation of the predictive accuracy. Statistical significance was defined as a p value <0.05.
Selection of surgical resection for patients with HCC
Child-Turcotte-Pugh (CTP) classification is conventionally used to pre-operatively assess the safety of hepatic resection. In general, only as a class of A or B is an indication for surgical resection. An Eastern Cooperative Oncology Group (ECOG) performance status 0–2 and American Society of Anesthesiologists (ASA) class 1–3 are also generally accepted indications. For assessment of reservoir function after surgery, we used ICG-R15 and Y-value to decide resection volume after measuring liver volume.1011 A remnant liver volume of 40% or more is generally recommended in cirrhotic patients for safety.12 We recommend surgery in cases of less than 20% of ICG-R15 and a Y-value less than 45. We have recently added cHVPG, and we recommend surgery in cases of where cHVPG is less than 10 mm Hg.6 For preoperative staging in our multidisciplinary team meeting, we use BCLC, Okuda stage, AJCC, and mUICC. In the case of surgery, we created a follow-up plan for the patient and collected data prospectively using the AJCC and mUICC staging systems. Curative resection was defined as that in which the entire tumor could be removed macroscopically. Lymph node involvement and distant metastasis were based on macroscopic inspection and palpation at the time of surgery, in addition to imaging study pre-operatively. We did not routinely perform lymph node dissection during hepatic resection for HCC unless preoperative imaging showed lymph node metastasis or we found lymph node enlargement in the operative field. For stage IVA of the AJCC and one type of stage IVA (anyTN1M0) of the mUICC, we aimed to perform surgery with curative intention according to reports from other authors,131415 and we also actively performed follow-up for treatment after common recurrence. For stage IVB, we rarely recommended surgery after a multidisciplinary team discussion of each case.16
RESULTS
We have included many tables throughout this study, and we have placed many of them into the supplementary information. We believe these tables are necessary for fully understanding our data related to staging systems, allowing the readers to follow our paper more easily.
The pre- and peri-operative characteristics of the patients are shown in Supplementary Table 1 (only online). The median age was 53 years, and 609 patients (76.9%) were male. HBsAg was positive in 599 cases (75.6%), and anti-HCV was positive in 45 cases (5.7%). The median platelet count was 153000/µL, and the median serum total bilirubin was 0.7 mg/dL. The serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were 41 U/L and 39 U/L on average, respectively. The median serum albumin was 4.0 g/dL, and the median international normalized ratio of prothrombin time was 1.06. The median alpha-fetoprotein was 43.7 ng/mL. CTP class A comprised 742 cases (93.7%), with class B totaling 36 cases (4.5%) and class C 14 cases (1.8%). ICG-R15 was 13.5% on average, and cHVPG was 5.1 mm Hg on average. Pre-operative TACE was done in 252 cases (31.8%). Major resection was undertaken in 308 cases (38.9%), which was defined as resection of the liver more than two Couinaud's segments. Operative time was 195 minutes on average. Bleeding during surgery was 700 mL on average. The median size of tumor was 4.0 cm, and tumor number was 1.0 on average. Post-operative complication happened in 80 cases (10.1%). The median length of hospital stay after surgery was 14 days. In-hospital mortality was recorded in 8 cases (1.0%).
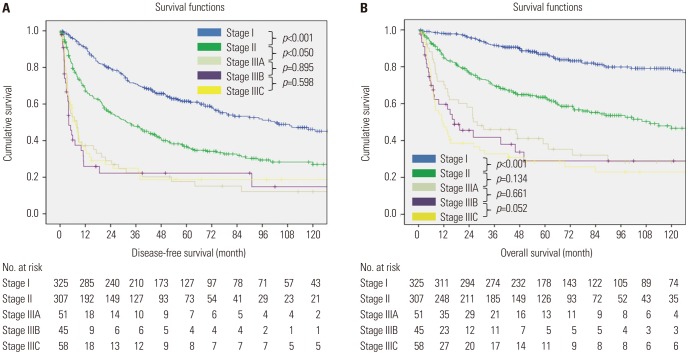
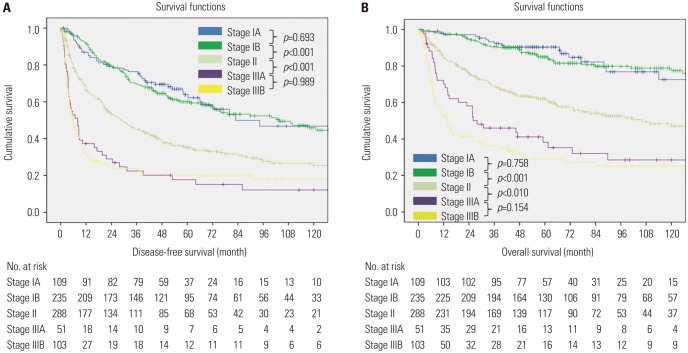
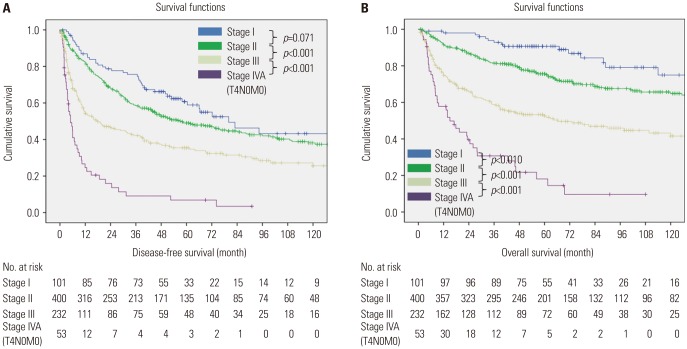
The distribution of patients and survival rate according to the three staging systems are shown in Supplementary Table 2 (only online). The total recurrence was 452 out of 792 (57.1%) cases during the follow-up period. For the 7th AJCC, 325 of 792 (41.0%) cases were stage I, 307 (38.8%) were stage II, 51 (6.4%) were stage IIIA, 45 (5.7%) were stage IIIB, and 58 (7.3%) were stage IIIC. For the mUICC, 101 of 792 (12.8%) cases were stage I, 400 (50.5%) were stage II, 232 (29.3%) were stage III, and 53 (6.7%) were stage IVA (T4N0M0). For the 8th AJCC, 109 of 792 (13.8%) cases were stage IA, 235 (29.7%) were stage IB, 288 (36.4%) were stage II, 51 (6.4%) were stage IIIA, and 103 (13.0%) were stage IIIB. The number of cases with an advanced stage, such as stage IVA and stage IVB, was very low for all three staging systems because we only enrolled patients who underwent surgical treatment. Based on the 7th AJCC, the 5-year disease-free survival rate of stage I was 61.5%, stage II was 36.8%, stage IIIA was 17.7%, stage IIIB was 14.8%, and stage IIIC was 18.7%. For 5-year overall survival rate, stage I was 86.8%, stage II was 63.5%, stage IIIA was 38.2%, stage IIIB was 28.9%, and stage IIIC was 28.6%. Based on mUICC, 5-year disease-free survival rate of stage I was 60.8%, stage II was 49.0%, stage III was 35.5%, and stage IVA (T4N0M0) was 6.8%. For 5-year overall survival rate, stage I was 90.7%, stage II was 75.6%, stage III was 52.6%, and stage IVA (T4N0M0) was 18.1%. Based on the 8th AJCC, 5-year disease-survival rate of stage IA was 63.9%, stage IB was 60.0%, stage II was 35.3%, stage IIIA was 17.7%, and stage IIIB was 19.8%. For 5-year overall survival rate, stage IA was 90.4%, stage IB was 85.0%, stage II was 62.0%, stage IIIA was 38.2%, and stage IIIB was 29.1%.
Univariable and multivariable analyses in relation to disease-free survival and overall survival for HCC patients are shown in Supplementary Tables 3 and 4 (only online). Multivariable analyses of the disease-free survival and overall survival models were tested for appropriateness of the proportional hazard assumption. The test based on Schoenfeld residuals showed that the variables met the proportional hazard assumption (Global p=0.143 for disease-free survival and p=0.468 for overall survival) when we excluded variables, like ‘intrahepatic metastasis (IM)’ that did not meet the proportional hazard assumption. For disease-free survival (Supplementary Table 3, only online), multivariable Cox regression showed hepatic vein invasion had the greatest impact, followed by serum albumin level (<3 g/dL), tumor size (>2 cm), and positive margin. For overall survival (Supplementary Table 4, only online), multivariable Cox regression showed CTP class C and B had the greatest significance, followed by tumor number (multiple), microvascular invasion, and positive margin.
Six cases of stage IVA and IVB (one type of IVA in mUICC, anyTN1M0) were excluded in the Kaplan-Meier curve. A similar percentage and patterns of censored cases were shown in each stage of 7th AJCC, 8th AJCC, and mUICC. Therefore, we believe the assumption that censoring is reasonably similar in all groups was fulfilled. Fig. 1 shows the Kaplan-Meier curve with disease-free survival and overall survival of patients with 95% confidence interval according to the 7th AJCC staging system. For disease-free survival, there were no significant differences among stage IIIA, stage IIIB, and stage IIIC, although there were significant differences among stage I, stage II, and stage IIIA. For overall survival, there was a significant difference between stage I and stage II, but there were no significant differences among other stages. Fig. 2 shows disease-free survival and overall survival of the 8th AJCC staging system. For disease-free survival, there were significant differences among stage IB, stage II, and stage IIIA. For overall survival, there were significant differences among stage IB, stage II, and stage IIIA. Fig. 3 shows disease-free survival and overall survival of the mUICC staging system. For disease-free survival, there were significant differences among stage II, stage III, and stage IVA (T4N0M0). For overall survival, all stages had significant differences among their stages. We then performed Bonferroni correction for log-rank test (Supplementary Tables 5, 6, 7, 8, 9, 10, only online). To summarize, Kaplan-Meier curves for disease-free survival and overall survival showed that the mUICC was superior to the 7th and 8th AJCC.
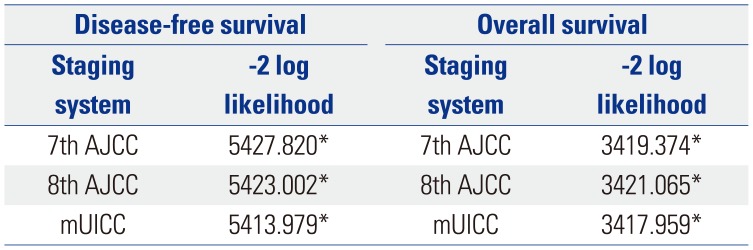
The homogeneity test results are shown in Table 1. Generally, more accurate stages showed lower ‘-2 log likelihoods’.7 For disease-free survival, mUICC was the best because the ‘-2 log likelihood’ had the lowest value. For overall survival, mUICC was also the best because of its lowest ‘-2 log likelihood’ among the three staging systems.
The discriminatory ability test is shown in Table 2. Generally, a higher linear trend chi-square value indicates better discriminatory ability.7 For disease-free survival, the Pearson chi-square value was the highest in the mUICC, followed by the 8th AJCC and 7th AJCC. For overall survival, the 7th AJCC had the highest Pearson chi-square value, followed by mUICC and the 8th AJCC. In Cochran-Armitage test for linear trend, the value of the Cochran-Armitage test was the highest in 8th AJCC, followed by mUICC and 7th AJCC, for disease-free survival. For overall survival, the mUICC had the highest value of Cochran-Armitage test, followed by the 8th AJCC and the 7th AJCC.
The results of cross-validation analysis using SPSS are shown in Table 3. For disease-free survival, all three stages had significant predictive power. The ‘z’ value in the Fisher r-to-z transformation between the test sample and validation sample was the lowest in 8th AJCC, followed by 7th AJCC and mUICC. For overall survival, all three stages had significant predictive power. The 7th AJCC had the lowest ‘z’ value, followed by mUICC and 8th AJCC, although the ‘z’ value of 8th AJCC was much higher than the others.
The second trial of the cross-validation analysis using SAS is shown in Supplementary Tables 11, 12, 13, 14 (only online).
For disease-free survival, the mUICC was better than the 7th AJCC, because p values (for ‘Pr>ChiSq’ in Supplementary Table 11, only online) of mUICC in both the test and validation samples had more significant ones. The mUICC was also better than the 8th AJCC based on the same reason.
For overall survival, the mUICC and the 7th AJCC had significant predictive power, and were comparable with each other in the test sample and validation sample. For mUICC and the 8th AJCC, we could not conclude which is better between mUICC and the 8th AJCC because the results of test sample and validation sample did not show consistent p values.
DISCUSSION
Although the BCLC has long been the dominant system for treatment-guided staging of HCC, some other authors do not fully agree with its underlying principles.45 One of the weaknesses of the BCLC is that it was not developed from a cohort of HCC patients based on multivariable analysis; therefore, it is difficult to predict the mortality of HCC patients.41718 BCLC is the only staging system that assigns treatment strategies based on specific prognostic subclasses stratified according to the patient's tumor characteristics, baseline liver function, and overall health status.19 Most physicians agree that these concepts are important, but some would maintain that BCLC increases the complexity of immediate clinical staging.119
Both the AJCC and the mUICC staging systems were developed based on survival analysis of patients who underwent hepatic resection. The AJCC developed the TNM staging system, and it has been updated regularly since the first edition was published in 1977.2021 Vauthey, et al.22 developed a simplified staging system for HCC, which was adopted as the TNM staging system of the AJCC after minor changes. Several reports have shown that the prognostic ability of the 7th TNM system is poorer than that of BCLC classification, particularly in patients with advanced-stage HCC.72324 The mUICC staging system originated from the Liver Cancer Study Group of Japan (LCSGJ), and Minagawa, et al.8 reported evidence for the development of the TNM system, validated the system, and compared its discriminatory ability and predictive power to those of the AJCC staging system in 13772 patients who underwent curative hepatic resection. They insisted that mUICC staging may be more appropriate for stratifying patients with earlystage HCC.
There are two types of staging systems for HCC. One is clinical staging, such as BCLC, Japanese Integrated System score (JIS), and CLIP, which can be applied in both operable and non-operable patients: these have been described as ‘medical staging’.18 The other type of staging system is based on pathologic staging, such as AJCC and mUICC, which can be applied in patients eligible for surgery: these have been described as ‘surgical staging’.18 We think multiple staging systems complicate the daily practice and academic activities of liver surgeons, and they keep clinicians from carefully using the currently available staging systems or treatment algorithms and from becoming familiar with their features and limitations.3 For instance, Kudo, et al.2526 developed the new staging of JIS score based on LCSGJ, and other authors sought to modify it with some significant prognostic variables.272829 One of the reasons why they developed a new staging system was that the LCSGJ required 12 groups (three liver disease stages multiplied by four tumor stages), which could be complicated in clinical practice. We tried applying the JIS score to our patient cohort; however, we did not find a difference in the survival curves from the mUICC in this study (Supplementary Fig. 1, only online). This result would suggest that the mUICC is sufficient without adding other variables for staging HCC patients who have undergone surgical resection. One reason for the sufficiency of mUICC is that most patients who underwent surgery have relatively good liver function, compared with inoperable patients.
As a whole, mUICC seemed to be superior to AJCC in this study. First, we suggest it may be related to the management problem with our data. However, we consecutively and prospectively collected the data of the patients, and this is the same as extracting routinely collected data from existing sources, such as electronic health record or registries.30 This approach does not interfere with routine practice nor require additional data collection. Second, bias or systematic error may be present, which is found in almost all scientific papers. The term ‘bias’ describes the systematic tendency of any factors associated with the design, implementation, analysis and interpretation of the results of the studies to estimate how the treatment derivates from its true value. We did our best to reduce the bias as much as possible. The mUICC and the AJCC were applied to the same clinical data, and we introduced significantly more statistical methods compared with other prior articles for HCC staging systems. Third, ‘by chance’, bias could happen within p values, called ‘random error’. More studies of other datasets from multiple centers are needed to solve this problem. Last, the mUICC should be more powerful than AJCC from academic and scientific perspectives after analyzing the data of our center, although the geographic heterogeneity observed in HCC might result in differences between mUICC and AJCC. Vauthey, et al.22 proposed a simplification of the TNM staging system and identified independent prognostic factors. They recommended that the T-component focus on vascular invasion, tumor number, and tumor size, which corresponded almost completely with those that were introduced in the mUICC staging system as significant prognostic variables.
The results of this study support the use of the mUICC staging system over the AJCC staging system. While both staging systems allow for the clear stratification of patients into prognostic groups, we believe the mUICC staging system may be more appropriate for stratifying patients with HCC. In addition, we suggest that it may be sufficient to use a surgical/pathologic staging system, such as the mUICC or the AJCC, when surgical resection is performed in patients with HCC.


 XML Download
XML Download