

 Citation
Citation Print
Print



INTRODUCTION
Severe asthma accounts for 5%–10% of asthma cases, but it is responsible for most asthma-related morbidities and health care costs.12 In accordance with the need for better therapeutic options for patients with severe asthma, several biologic agents have been developed during the past few years.345 The guidelines recommend add-on treatment with anti-immunoglobulin E (IgE) or anti-interleukin 5 agents for patients whose asthma remains uncontrolled despite the use of high-dose inhaled corticosteroids (ICS).6 However, these biologic agents are indicated only in patients with high IgE levels or eosinophil counts. Furthermore, the high cost burden is a challenge to maintaining the therapy for a long period of time.
Bronchial thermoplasty is an innovative nonpharmacological treatment that delivers radiofrequency current to the bronchial wall, resulting in a reduction of hypertrophied airway smooth muscle.7 Improvement in quality of life and decrease in acute exacerbations following the procedure have been demonstrated in clinical trials.8910 The first bronchial thermoplasty in Korea was performed in 2014; 4 patients have undergone the procedure so far. Here we share our experience of these patients, the only bronchial thermoplasty cases in Korea.
CASE DESCRIPTION
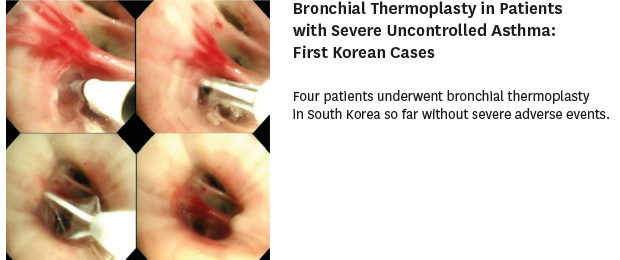
Four patients underwent bronchial thermoplasty due to severe uncontrolled asthma from 2014 to 2018 at Asan Medical Center in Seoul, Korea. Table 1 describes characteristics of the 4 patients. All procedures were carried out using the Alair Bronchial Thermoplasty system (Boston Scientific Corporation, Marlborough, MA, USA). The sequence of the procedures was right lower lobe, left lower lobe, followed by both upper lobes at 3-week intervals. All procedures were performed with the patient under general anesthesia. The number of radiofrequency energy delivery (activation) was recorded for each session. Fig. 1 shows the relevant images of the procedure. A laparoscopic trocar fused to a catheter mount designed by our anesthesiologists was used to prevent air leakage during the procedure.11 Oral prednisolone 50 mg was started 3 days before and maintained until the day after the procedure, followed by tapered doses over 2 weeks. All patients provided written informed consent before the procedure. The images are published under agreement of the patient.
Table 1
Characteristics of case patients

FEV1 = forced expiratory volume at 1 second, BDR = bronchodilator reversibility, ICS = inhaled corticosteroid, OCS = oral corticosteroid, IgE = immunoglobulin E, RLL = right lower lobe, LLL = left lower lobe, BUL = both upper lobes, AE = acute exacerbation.
aFluticasone or equivalent; bPrednisolone or equivalent.
Fig. 1
Bronchial thermoplasty procedure. (A) Performing bronchial thermoplasty under general anesthesia; (B) bronchoscopy images of the bronchial thermoplasty procedure; (C) the number of activations counted on a sheet; (D) laparoscopic trocar used as a bronchoscopy introducer.

Case 1
A 61-year-old woman patient with severe uncontrolled asthma underwent the first bronchial thermoplasty procedure in Korea. Since being diagnosed with asthma 12 years previously, she had experienced frequent exacerbations and had visited the emergency room almost once a week, despite treatment with a high-dose inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA; budesonide/formoterol 640/18 µg twice daily), a long-acting muscarinic antagonist (LAMA), and a leukotriene receptor antagonist; oral corticosteroids (prednisolone 20 mg/day) were prescribed to control exacerbations. She had developed steroid-induced osteoporosis and iatrogenic Cushing syndrome. Omalizumab provided a slight reduction in the number of exacerbations, but maintaining the treatment was challenging due to its high cost.
She underwent the first bronchial thermoplasty on May 27, 2014. Before the procedure, the spirometry results showed a forced expiratory volume at 1 second (FEV1) of 1.48 L (64% of predicted). The Asthma Control Test (ACT) score improved from 6 to 21 by 5 months after bronchial thermoplasty. The frequency of acute exacerbation requiring an emergency room visit was significantly reduced to once a year even after the step-down of ICS treatment. The oral corticosteroid dose was reduced to prednisolone 5 mg/day, which is being maintained as a physiologic dose due to iatrogenic adrenal insufficiency.
Case 2
A 40-year-old man patient with asthma visited our hospital complaining of dyspnea that prevented him from performing ordinary activities of daily living. He had experienced 3 episodes of acute exacerbation, each requiring hospitalization, in the preceding year. Omalizumab initiated at another hospital had failed to improve asthma control. At presentation he was receiving a high-dose ICS (fluticasone 750 µg twice daily), LABA (vilanterol 25 µg/day), LAMA, and a leukotriene receptor antagonist. He underwent 3 sessions of bronchial thermoplasty, starting from October 28, 2014. After the second bronchial thermoplasty to the left lower lobe, he was readmitted due to fever and chest pain. A chest radiograph and computed tomography scan showed left lower lobe collapse and consolidation, which completely resolved with 2 weeks of fluoroquinolone treatment. The third session was performed on schedule. He reported that the number of asthma attacks was slightly reduced after the procedures. However, it was not possible for him to decrease the doses of inhaled and oral corticosteroids. He is still steroid dependent and is currently participating in a clinical trial.
Case 3
A 49-year-old woman patient with asthma was referred for bronchial thermoplasty on August 6, 2014. She had been taking systemic corticosteroids for 7 years due to severe uncontrolled asthma. She complained of dyspnea and wheezing despite treatment with a moderate-dose ICS/LABA (budesonide/formoterol 320/9 µg twice daily), LAMA, doxofylline, and deflazacort 18 mg/day. She was suffering from osteoporosis and was suspected of having iatrogenic Cushing syndrome. Her FEV1 before bronchial thermoplasty was 1.99 L (72% of predicted). Bronchial thermoplasty was performed without any complications; however, her symptoms remained unchanged, and the doses of systemic and inhaled corticosteroids could not be reduced after the procedure. She is still receiving the same maintenance medication.
Case 4
A 50-year-old man patient presented to our hospital due to severe uncontrolled asthma. He had a history of respiratory arrest due to asthma exacerbation 20 years previously. He had been receiving a high-dose ICS/LABA (fluticasone propionate/salmeterol 500/50 µg twice daily) and an oral corticosteroid (methylprednisolone 4 mg/day). In addition, he had required daily ipratropium and salbutamol nebulizer to control his symptoms. Despite the treatment, he had had at least 1 or 2 episodes of severe exacerbations per month. Before bronchial thermoplasty, his FEV1 was 2.03 L (49% of predicted), and the ACT score was 6. The patient underwent bronchial thermoplasty starting from July 24, 2018, without experiencing any complications. Eight weeks after the last session, he reported much improved quality of life, and his ACT score was 23. Even with a decreased dose of ICS, he has had no exacerbation episodes for 3 months so far.
DISCUSSION
Bronchial thermoplasty delivers thermal energy at 65°C to the airway walls via a bronchoscope. It reduces airway smooth muscle mass and attenuates bronchoconstriction.12 Its safety and efficacy have been shown in 3 large randomized trials; in the AIR2 study, a multicenter, randomized, sham-controlled trial, decrease in severe exacerbations and improvement of asthma-specific quality of life were demonstrated, with tolerable side effects.10 This case series presents 4 patients who underwent bronchial thermoplasty in Korea. Among them, 2 patients showed significant reductions in respiratory symptoms and number of exacerbations; 1 patient reported a mild reduction of exacerbations, but the oral corticosteroid requirement could not be reduced; and 1 patient did not show any change in symptoms or exacerbation rate. One patient developed fever, chest pain, and left lower lobe collapse requiring antibiotic treatment; no other significant adverse events were observed.
Although bronchial thermoplasty is a promising therapeutic modality, there are several issues that should be resolved. First, criteria that can categorize patients who can safely undergo bronchial thermoplasty have not yet been established. Randomized trials that evaluated the safety and efficacy of bronchial thermoplasty included patients with FEV1 greater than 50% or 60% of predicted.8910 However, bronchial thermoplasty successfully performed in patients with lower FEV1 has been reported.1314 The last patient in the present case series had FEV1 less than 50% of predicted but safely underwent the procedure, with favorable clinical results. Therefore, low FEV1 may not be an absolute contraindication. More studies are needed to establish the criteria for appropriate patient inclusion.
Another unresolved issue of bronchial thermoplasty is that there is no known predictor of which patients will respond to the procedure. Although it seems reasonable to expect that patients with greater airway hyperreactivity would show a better response, the presence or absence of airway hyperreactivity does not appear to predict the outcome of bronchial thermoplasty.15 Similarly, the presence of allergies does not seem to be associated with the outcome.16 Interestingly, a recent study reported that the number of activations could predict the response to bronchial thermoplasty.17 Further research with a focus on outcome predictors of bronchial thermoplasty will help physicians to identify patients who are likely to benefit.
The long-term effect of bronchial thermoplasty is another concern that should be addressed. According to a study that assessed approximately 85% of patients who participated in the AIR2 study, favorable effects of bronchial thermoplasty were sustained at 5 years after the procedure.16 A similar result was shown by the first patient in the present case series; during the 4-year follow up, her asthma has been under control, with an extremely reduced exacerbation rate and improved quality of life. However, because this procedure is still novel, efficacy data beyond 5 years are scarce.
In conclusion, we performed bronchial thermoplasty in 4 patients with severe uncontrolled asthma for the first time in Korea, without serious adverse events. According to a systematic review, bronchial thermoplasty provided lower exacerbation rates rather than improving quality of life18; two of our study patients experienced significantly lower rates of acute exacerbation. Although it remains as a limitation that outcome predictors are not clear yet, bronchial thermoplasty can be considered as an important treatment option for patients with severe uncontrolled asthma. Discussion with experts about its feasibility and necessity will ensure the best possible care to the patients.
 XML Download
XML Download