

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Palpable lesions of the head and neck are common in clinical practice. Many different lesions may be observed from the scalp to the face and neck, and may be classified into various categories according to their location and histological characteristics. According to the World Health Organization classifications, published in 2017, head and neck tumors are grouped into 10 major categories based on location (1). Some of these tumors may present as palpable lesions, but they may also manifest signs other than palpable lesions depending on their locations. Palpable lesions are often recognized early and may motivate patients to seek medical help. Many studies have focused on head and neck masses; however, there are few studies focusing on scalp or face masses, which are frequently encountered in clinical settings.
Radiologic evaluation is essential for the diagnosis and treatment of tumors. Ultrasonography (US) is often used as the primary imaging modality for palpable lesions and may help characterize cystic or vascular masses. CT is useful for the evaluation of calcified lesions, tissue discrimination, spatial resolution, staging, mass effect, and treatment planning. MRI is superior in discriminating between tumor and normal tissue (2). It is important for the radiologist to be familiar with various types of lesions and their findings on imaging.
The purpose of this article is to illustrate the various lesions of the scalp and face that may present as palpable lesions. The lesions described here were selected according to frequency of occurrence, which was determined by analyzing lesions in patients who underwent radiologic evaluation for superficially palpable masses in our hospital. The lesions have been described in the following order according to their origin: cutaneous layer, subcutaneous layer, muscle layer, bone layer, and the parotid gland.
CUTANEOUS AND SUBCUTANEOUS LAYER
EPIDERMAL CYST
Epidermal cysts, also known as epidermoid cysts or epidermal inclusion cysts, are benign cutaneous or subcutaneous lesions lined with stratified squamous epithelium and filled with keratin debris (345). Epidermal cysts may form when hair follicles become obstructed. They may also arise from traumatic or surgical implantation of the epidermis resulting in lesions of non-follicular areas, hence the synonym epidermal inclusion cyst. They grow slowly and may reach several centimeters in diameter. Cutaneous dermoid cysts are different lesions from epidermal cysts in that they contain normal cutaneous structures such as hair, sebaceous lobules, eccrine glands, apocrine glands, and/or smooth muscle. The sebaceous gland content is responsible for the fatty element of the lesions. They are usually 1–4 cm in diameter and commonly located around the eyes (56789). On US, with or without through transmission, epidermal cysts appear as well-circumscribed, oval, hypo- or hyperechoic masses (Fig. 1A) (41011121314). They also show a lack of internal vascularity, which can differentiate them from other solid masses (14). On CT, these lesions have attenuation similar to that of skeletal muscle (Fig. 1B) (3). On MRI, they appear as well-defined masses with high T2 signal intensity and high or iso T1 signal intensity compared to underlying muscle (Fig. 1C, D) (8131415).
PILOMATRICOMA
A pilomatricoma, or calcifying epithelioma of Malherbe, is a tumor arising from primitive cells that differentiate into the hair matrix. They usually occur as solitary lesions; the most common sites are the head, neck, and upper extremities. Tumors vary in diameter from 0.5–3.0 cm. They frequently present as firm, deep-seated nodules located in the lower dermis (31617). Early lesions are usually cystic, consisting of basaloid cells lining the cystic cavity which are contiguous with eosinophilic shadow cells admixed with keratin in the center of the lesion. Older pilomatricoma lesions become solid, with prominent shadow cells, keratin debris, secondary multinucleated giant cells, and dystrophic calcifications (16). Calcifications are seen in about 85% of lesions (317). On US, the lesions appear as subcutaneous hypoechoic masses, with internal echogenic foci, hypoechoic rims, or posterior acoustic shadowing from internal calcifications (Fig. 2A). They may show mild to moderate vascularity on color Doppler imaging (1819). CT imaging shows a calcified nodule in the subcutaneous layer (Fig. 2B).
HEMANGIOMA
Hemangiomas are benign vascular neoplasms which grow by endothelial cell hyperplasia. They should be differentiated from vascular malformations, which are localized defects of vascular morphogenesis (202122). Up to 70% of hemangiomas are visible at birth and 87% are diagnosed by 1 month of age (23). They occur most frequently in the head and neck region (60%), followed by the trunk (25%) and the extremities (15%) (2122). Hemangiomas are classified as either infantile or congenital hemangiomas (20212224). Infantile hemangiomas develop shortly after birth and undergo a rapid proliferative phase during the first 6–12 months of life followed by spontaneous regression. The lesions usually resolve between 5 and 9 years of age. Congenital hemangiomas present as fully developed lesions at birth which may rapidly involute during the first year of life; some lesions may never involute. On US, hemangiomas show either poorly defined or well-defined hypoechoic masses with heterogeneous echotexture from multiple cystic spaces. They may display high vascular flow on color Doppler imaging, particularly in the proliferative phase (Fig. 3). On CT, they are isoattenuating relative to muscle on non-contrast scans and show avid enhancement on contrast-enhanced scans, particularly in the proliferative phase. On MRI, they are isointense to slightly hyperintense on T1-weight imaging, hyperintense on T2-weighted imaging, and demonstrate avid contrast enhancement (2324).
BRANCHIAL CLEFT CYST
Branchial cleft anomalies arise from the incomplete obliteration of a branchial tract, resulting in a cyst, sinus, or fistulous track (25). They are the second common congenital head and neck lesions in children (2627). Second branchial cleft anomalies account for 95% of all branchial cleft lesions and typically result in cyst formation. They are often located close to the anterior border of the sternocleidomastoid muscle. First branchial cleft anomalies are relatively less common and are located close to the parotid gland. US of a typical branchial cleft cyst shows a well-defined, unilocular, anechoic lesion without internal debris or vascularity. Infection or hemorrhage may result in thick walls, internal debris, and septa (Fig. 4A). CT imaging shows sharp margins, fluid density, and thin walls (Fig. 4B, C). Cyst wall thickness and enhancement vary with the degree of inflammation. MRI demonstrates the cystic property of high signal intensity on T2-weighted imaging, but T1 signal intensity may range from low to high with variation in the proteinaceous contents of the cyst (2627).
SUBCUTANEOUS AND MUSCLE LAYER
LIPOMA
Lipomas are the most common mesenchymal neoplasms and consist of mature fat cells. Approximately 25% of lipomas occur in the head and neck, primarily in the subcutaneous layer of the posterior neck (28). Most are well-defined encapsulated masses found in the subcutaneous layer or between muscles and other connective tissue structures. There are a number of lipoma variants. Fibrolipomas are rich in fibrous connective tissue, while angiolipomas are characterized by prominent thin-walled blood vessels. Non-adipose areas show low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. They show a variable enhancement pattern following intravenous contrast administration. Myxolipomas are lipomas with degenerative changes and a prominent mucoid area. Myolipomas contain variable amounts of benign smooth muscle and mature adipose tissue (2829). On US, lipomas are typically homogeneous and hyperechoic relative to the adjacent soft tissue. They may contain echogenic lines parallel to the skin surface (Fig. 5A, B). They show characteristic low attenuation on CT (Fig. 5C) and T1 high signal intensity on MRI.
BONE LAYER
OSTEOMA
Osteomas are the most common benign neoplasms of the skull and are composed of variable proportions of compact and trabecular bone (30313233). They tend to grow along the outer table of the skull, primarily in the frontal or parietal bones, and are either sessile or pedunculated (31). Osteomas are benign, painless, slow-growing tumors (32). On US, bony protrusion can be identified with shadowing (Fig. 6A). Osteomas are typically juxtacortical, well-defined, round or oval sclerotic lesions on CT (Fig. 6B). They do not have soft tissue components and do not show enhancement. On MRI, these lesions are hypointense on T1-weighted imaging and have variable signal intensity on T2-weighted imaging, depending on the proportions of compact and cancellous bone (303132).
PAROTID GLAND
PLEOMORPHIC ADENOMAS
Pleomorphic adenomas are the most common benign salivary gland tumors in adults. They predominantly affect the superficial lobe of the parotid gland. Pleomorphic adenomas originate from epithelial and connective tissue (343536). On US, pleomorphic adenomas appear as heterogeneous solid masses (Fig. 7A). On CT and MRI, smaller tumors are more homogeneous and well-defined with strong enhancement, whereas larger tumors tend to show a lobulated contour and are more heterogeneous, including necrotic and hemorrhagic areas (Fig. 7B-E) (343536).
WARTHIN'S TUMOR
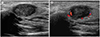
Warthin's tumors are the second most common benign salivary gland tumors and are located primarily on the lower pole of the parotid gland. They usually present as asymptomatic, slow growing, and well-encapsulated masses. These tumors consist of an oncocytic epithelial cell component, which develops cysts and papillary projections, and a variable amount of lymphoid tissue (343536). Warthin's tumors present as well-circumscribed partly cystic and partly solid lesions. US images of Warthin's tumors show heterogeneous solid masses or complex cystic lesions. They may show variable vascularity on a color Doppler study (Fig. 8A, B). They tend to show isoattenuation on pre-contrast CT images and strong early enhancement patterns after contrast injection (Fig. 8C, D) (343536).
MUCOEPIDERMOID CARCINOMA
Mucoepidermoid carcinomas are malignant salivary gland neoplasms arising from ductal epithelium; 50% of these tumors arise from the parotid gland. They are pathologically classified as low, intermediate, or high-grade and imaging features depend on the histological type. Low-grade lesions are well circumscribed, whereas high-grade lesions tend to have poorly defined margins and infiltrate surrounding tissues. Low to intermediate signal intensity may be observed on T1- and T2-weighted images (34353637). On US, mucoepidermoid carcinomas show an ill-defined, irregular, complex echoic mass (Fig. 9).
CARCINOMA EX PLEOMORPHIC ADENOMA
Carcinoma ex pleomorphic adenomas arise from malignant changes of a benign pleomorphic adenoma or as a malignant tumor in a patient with a surgical history of a pleomorphic adenoma. The rapid growth of a pre-existing tumor with associated pain, facial nerve paralysis, and skin fixation are suggestive of malignant transformation. An irregular shape, infiltrative margin, and low T2 signal intensity may be observed in carcinoma ex pleomorphic adenomas (34353638). On MRI, it shows intermediate signal intensity on T1-weighted imaging, low to high signal intensity on T2-weighted imaging, and heterogeneous enhancement on the post-contrast study (Fig. 10).
CONCLUSION
Various lesions of the scalp and face can occur from the skin to the skull with superficially palpable symptoms. Superficially palpable lesions of the scalp and face tend to be benign and small in size, but malignant lesions may be fast-growing large masses. Of the imaging modalities, US is especially useful for identifying the origin of lesions and for the evaluation of small and superficial lesions. CT and MRI studies provide superior soft tissue resolution and reveal characteristic soft tissue features. A knowledge of the common lesions of the scalp and face and use of the appropriate imaging examinations will be helpful in the diagnosis and treatment.









 XML Download
XML Download