

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mixed-species malaria infections are often unrecognized or underestimated.1 Such infections accounted for 2.1% of the 1,140 cases of malaria logged by the GeoSentinel Surveillance Network based on treating physician diagnoses between 1997 and 2002.2 We hereby report the first described case of mixed infection with Plasmodium falciparum and Plasmodium ovale in a returned traveller in Korea.
CASE DESCRIPTION
A 25-year-old man of Korean origin, presented to the emergency department of the National Medical Center in August 2016. He travelled Cameroon and the Democratic Republic of the Congo for sixteen days, arriving Korea on 20th July 2016. He did not take malarial chemoprophylaxis. On 2nd August he had fever, headache and vomiting and visited National Medical Center on 5th August. Laboratory tests showed normal values for hemoglobin (Hb) and white blood cells, but the patient had a low platelet count of 16,000/μL (normal, 130,000–400,000/μL). Both aspartate transaminase (AST) and alanine transaminase (ALT) were elevated, with levels of 57 U/L (normal, < 40 U/L) and 58 U/L (normal, < 45 U/L), respectively. A peripheral blood smear revealed the presence of malarial parasites at a concentration of 459,448/μL (parasite density, 10.1%) (Fig. 1). The malarial parasites exhibited ring forms with occasional double chromatic dots. The Pf/Pan immunochromatographic test (ICT; SD BIOLINE Malaria Ag Pf/Pan™; Standard Diagnostics, Inc., Suwon, Korea) was positive for both P. falciparum-specific histidine-rich protein-2 and lactate dehydrogenase of Plasmodium species (P. falciparum, Plasmodium vivax, Plasmodium malariae, and P. ovale). Plasmodium species-specific polymerase chain reaction (PCR) assays confirmed the presence of P. falciparum and were negative for P. vivax, P. malariae, and P. ovale. For the PCR assays, nucleic acids were extracted from peripheral blood using MagnaPure 96 automated nucleic acid extractor and DNA and Viral NA SV Kit according to the manufacturer's instructions (Roche Diagnostics, Mannheim, Germany). A nested PCR for Plasmodium spp. 18s rRNA (490 bp amplicon), P. vivax (470 bp), and P. falciparum (340 bp) was performed according to the modified protocols from previous report.3
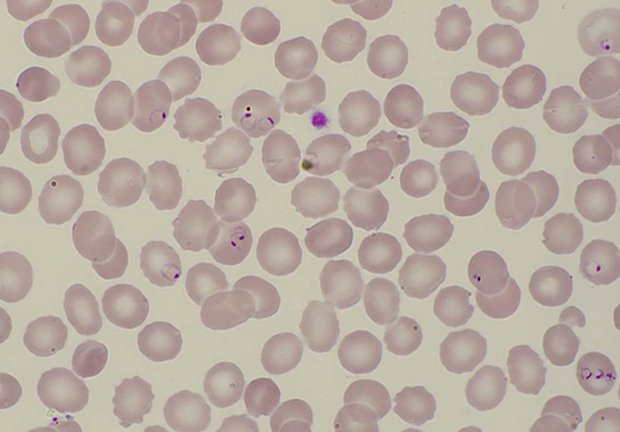
Fig. 1
Peripheral blood smear (5th August 2016). Microscopic examination was performed by two independent clinical pathologists. Microscopic examination of Wright-Giemsa stained peripheral blood smear revealed that many ring forms of Plasmodium parasites with occasional double chromatin dots (459,448/µL). Multiply-infected red blood cells were frequent.
Upon being diagnosed with falciparum malaria, the patient was admitted and treated with intravenous artesunate (2.4 mg/kg body weight/dose at 0, 12, 24, and 48 hours), followed by atovaquone/proguanil at a dose of 1,000/400 mg per day for 3 days. Fever subsided on the 3rd day after the initial examination, and the patient remained afebrile until the day of discharge. Based on peripheral blood smear, the number of malarial parasites in the bloodstream had decreased to 386,579/μL (parasite density, 9.2%) at the 12-hour follow-up, and malarial parasites were not observed at the 24-hour follow-up. Both AST and ALT continuously increased until they reached maximum levels of 231 U/L and 233 U/L, respectively, on the 3rd day after the initial examination and decreased thereafter. The patient's platelet count continuously increased after the initial examination and was 184,000/μL on the 12th day after the initial examination. The patient's condition improved, and he was discharged on 10th August.
On 14th September 2016, which was 36 days after completing artesunate treatment, and 33 days after completing atovaquone/proguanil treatment, the patient developed fever with a body temperature of 40°C. He visited Daegu Catholic University Hospital on 19th September. A peripheral blood smear revealed no malarial parasites. The Plasmodium species-specific PCR assays were performed. For the PCR assays, nucleic acids were extracted from peripheral blood using Chemagic 360 according to the manufacturer's instructions (PerkinElmer, Waltham, MA, USA). Plasmodium-screening PCR and Plasmodium species-typing PCR were performed according to the modified protocols from previous reports.4,5 These assays produced positive result for P. ovale and negative results for P. falciparum, P. vivax, and P. malariae. Laboratory tests showed Hb of 7.0 d/dL (haematocrit of 21.1%) and a platelet count of 106,000/μL. Chloroquine was given, but the patient did not take the drug. He visited the National Medical Center on 6th October. He was afebrile and in good general condition. The PCR assays performed at National Medical Center showed positive result for Plasmodium spp., but the involved species could not be determined due to the low parasite concentration. The ICT was negative for both Pan and Pf column. A peripheral blood smear revealed no malarial parasites. Chloroquine 600 mg base was given and followed by at a dose of 300 mg base at 6, 24, and 48 hours for the P. ovale treatment, and fourteen days of primaquine (30 mg base/day) were administered for the eradication of possible hypnozoites. PCR tests were performed on 26th October and produced negative results for P. falciparum, P. ovale, P. vivax, and P. malariae. The patient has remained symptom-free.
DISCUSSION
Among mixed malaria infections, mixed P. falciparum and P. ovale infections are particularly rare, accounting for only 0.3% of total malaria infections in the afore mentioned GeoSentinel study.2 The rarity of P. ovale infection is the primary reason for the extremely low incidence of such mixed infections. P. ovale occurs in Africa and in foci within Asia and Oceania and is often present with other Plasmodium species in the context of mixed infections. The natural distribution of P. ovale is in sub-Saharan Africa and the islands of the western Pacific.6 In the Manyemen forest region of Cameroon, the prevalence of P. ovale was 10.5%.7 Of 198 malaria-positive samples of children under 5 years old, 17.2% were positive for P. ovale in Democratic Republic of Congo.8 The other reason for the rarity of P. falciparum and P. ovale mixed infection is that P. ovale tends to be missed in mixed infections because of its low parasite density.9 To our knowledge, there have been four case reports to date that have described mixed-species malaria infections in Korea, all of which involved P. falciparum and P. vivax mixed infections10-13; thus, the case described here is the first reported case of P. falciparum and P. ovale mixed infection in Korea.
The delayed clinical presentation of P. ovale malaria could be attributable to its different life cycle compared with that of P. falciparum. P. ovale has a dormant liver stage during which parasites exist as hypnozoites and can remain silent for years. In our case, the patient had no history of prior travel to endemic area for P. falciparum or P. ovale other than Cameroon and the Democratic Republic of the Congo. And he did not travel outside of Korea during the period between the two episodes of Plasmodium infection. Since Korea is free of those two Plasmodium species, it is likely that the patient was infected with both Plasmodium species during his trip to Cameroon and the Democratic Republic of the Congo. At the first presentation of Plasmodium infection, the PCR assays were positive only for P. falciparum and negative for P. ovale. The mean prepatent period of P. ovale infection is 12–20 days, with a median of 14.5 days.14 The symptom onset of second presentation took place on the 52nd day after leaving Cameroon and the republic of Congo. It is likely that P. ovale remained dormant in hepatocytes as hypnozoites at the time of initial presentation, rather than in the prepatent period, since 52 days are longer than typical prepatent period of P. ovale.
In an entomological survey that investigated 2,485 Anopheles mosquito specimens in Cameroon from October 2004 to September 2005, the annual average sporozoite rate was 5.8%, and no specimens with P. falciparum and P. ovale mixed infection were found.15 In Papua New Guinea, 2.3% of infected mosquitoes were found to carry a mix of P. falciparum and P. vivax malarial organisms, whereas the prevalence of mixed infections in humans was 69.3%.16 Given the relatively low prevalence of mixed infections in mosquitoes, it is plausible that mixed infections result from separate inoculations of sporozoites from mosquitoes infected with a single species rather than the simultaneous inoculation of sporozoites from mosquitoes infected with multiple species.
The ICT, which permits immediate diagnosis, is known to have suboptimal sensitivity for P. ovale (approximately 60%).17 Expert blood film microscopy is the standard diagnostic method for malaria, but young ring forms of three malarial species may be difficult to distinguish in thick blood films during co-infections.18 At re-presentation, the ICT and microscopic examinations of our patient did not reveal P. ovale. Compared with microscopy and the ICT, PCR testing has the highest sensitivity for detecting parasites at low levels.19 In a meta-analysis that included 42 articles, the prevalence of infection detected using microscopy was 50.8% of detected using PCR.20 PCR testing should be considered when a low level of parasitaemia is suspected, such as mixed-species malaria infections.
This case highlights the importance of considering malaria infection even in persons who have previously received malaria treatment. It also shows the usefulness of PCR testing for diagnosing P. ovale infections, which often present with a low level of parasitaemia.
 XML Download
XML Download