

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Cutaneous carcinosarcoma is an exceedingly rare biphasic tumor that histologically comprises an intimate admixture of epithelial and mesenchymal elements, both of which are malignant.1 The term carcinosarcoma was first used by Virchow in 1864.2 Carcinosarcomas can occur in diverse organs, such as the skin, lungs, esophagus, colon, and uterus.3456 Dawson7 is credited with describing the first cutaneous carcinosarcoma in 1972. Cutaneous carcinosarcoma typically arises on sun-damaged skin as a nodular lesion and often showing ulceration. The most commonly affected sites include the face and scalp. Although cutaneous carcinosarcoma is presented by patients of a wide age range, it is predominantly a tumor of the elderly. Clinically, no distinguishing characteristics have been identified and differential diagnosis varies extensively.8
Detailed data on the clinical and histopathologic features of Korean patients with cutaneous carcinosarcomas are not available. Herein, we analyzed 11 patients with histopathologically proven cutaneous carcinosarcomas at Chonbuk National University Hospital. The aim of this study was to evaluate the clinicopathologic and immunohistochemical characteristics of cutaneous carcinosarcomas in the Korean population.
METHODS
Between January 2006 and March 2016, 11 patients were histologically diagnosed with cutaneous carcinosarcoma at Chonbuk National University Hospital. Their medical records were reviewed, and all pathologic slides were retrieved from the medical database for diagnostic verification.
Clinical features
The following demographic and clinical features were obtained: age, gender, location, duration, tumor size and ulceration, lymph node (LN) and distant metastasis, clinical impression, treatment modalities, follow-up period, and recurrence.
Histopathologic and immunohistochemical features
All of the samples were fixed in 10% formalin, routinely processed and embedded in paraffin wax. Then, 4-mm thick sections were stained with hematoxylin and eosin. Furthermore, sections from each case were subjected to appropriately controlled immunohistochemical reactions employing cytokeratin AE1/AE3 (Dako, Glostrup, Denmark), epithelial membrane antigen (EMA; Dako), p53 protein (Dako), p63 protein (Dako), vimentin (Dako), desmin (Dako), and S-100 protein (Dako). All cutaneous carcinosarcomas specimens were evaluated by two dermatopathologists.
RESULTS
Demographic and clinical findings
The mean age at presentation was 71.5 ± 18.2 (range, 43–96) years. Cutaneous carcinosarcoma primarily occurred in patients aged > 60 years and predominantly in men (men-to-women ratio of 1.75:1).
The clinical data for all 11 cases are shown in Table 1. The mean duration of the disease was 11.2 (range, 1–24) months. Clinically, lesions were commonly presented as ulcerated nodules (Fig. 1), ranging from 7 to 50 mm in size with a mean diameter of 15.9 mm. The most common site of cutaneous carcinosarcoma was the head and neck (8/11, 72.7%), followed by the lower extremities (2/11, 18.2%), and penis (1/11, 9.1%). Of the eight cutaneous carcinosarcomas developing on the head and neck, four were present on the cheek, two on the scalp, one on the neck, and one on the ear.
Table 1
Clinical characteristics in 11 patients with cutaneous carcinosarcoma
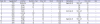

The most common clinical diagnosis was squamous cell carcinoma (SCC) (7/11, 63.6%), followed by basal cell carcinoma (BCC) (3/11, 27.3%), and keratoacanthoma (1/11, 9.1%). No cases correctly predicted cutaneous carcinosarcoma. Although distant metastasis was not observed in any patient, three patients showed metastasis to the regional LNs (two inguinal and one cervical). Cutaneous carcinosarcomas were resected via wide local excision (WE) with a 5–6 mm margin (WE, 10/11; 90. 9%) and Mohs micrographic surgery (MMS) with a 2-mm margin (first MMS, 1/11; 9.1%). The patients were followed-up for an average of 22.6 (range, 2–60) months after surgery. Although no deaths were reported during the follow-up period, two cases of local recurrence were observed.
Histopathologic and immunohistochemical findings
Histologically, cutaneous carcinosarcomas showed characteristic features. Foci of epithelial dysplasia or SCC or BCC and malignant spindle cell tumor were observed in all cutaneous carcinosarcoma cases (Table 2). The squamous cell component of the carcinomatous area — consisting of invasive or in-situ SCC well or poorly differentiated — was present at the base of the tumor and in the adjacent area. The basal cell component of the carcinomatous area consisted of atypical basaloid keratinocytes that showed peripheral palisading and retraction artifact. The bulk of the lesion was predominantly composed of spindle cells, which were intermingled with various proportions of epithelial cells. Transition zones between the epithelial and spindle tumoral cell components were present in 8 cases (Fig. 2A). The spindle cells in the sarcomatous area showed variable degrees of nuclear pleomorphism with an eosinophilic cytoplasm. In most cases, the nuclei had clumped chromatin and showed a marked mitotic activity with atypical mitosis (Fig. 2B).
Table 2
Histopathologic and immunohistochemical characteristics in 11 cutaneous carcinosarcoma cases
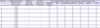
Fig. 2
Histopathologic findings of cutaneous carcinosarcoma. (A) The transition zone between carcinomatous and sarcomatous areas (H & E, × 100). (B) Clumped chromatins and marked mitotic activities in sarcomatous area (H & E, × 400).

The results of the immunohistochemical analyses are summarized in Tables 2 and 3. Positive cytoplasmic staining for cytokeratin AE1/AE3 was present in the epithelial cells of all cases and in the spindle cells of 7 (63.6%) cases (Fig. 3A and B). A strong diffuse expression was observed in one of these 7 cases, while scattered spindle cells with faint expression were observed in the remaining 6 cases. Prominent cytoplasmic expression of EMA was present in the epithelial cells of all cases. Strong nuclear expression for p53 protein was present in six of 11 cases, with cells of both tumor types being immunopositive (Fig. 3C and D). Nuclear expression of p63 protein was seen in the epithelial cells of nine cases. The spindle cells of 10 cases showed a diffuse cytoplasmic expression of vimentin, while focal vimentin expression was observed in the scattered squamous cells of one case (Fig. 3E and F). The spindle cells of only one case showed focal cytoplasmic expression for S-100 protein but not that of desmin.
Table 3
Overall immunohistochemical summary of cutaneous carcinosarcomas
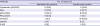
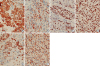
Fig. 3
Immunohistochemical findings of cutaneous carcinosarcoma (A, B) Cytokeratin AE1/AE3 expression in the squamous and spindle cells (immunoperoxidase, × 400). (C, D) Strong positive nuclear p53 protein expression, similar in the squamous and sarcomatous cells (immunoperoxidase, × 400). (E, F) Vimentin expression in the squamous and spindle cells (immunoperoxidase, × 400).
DISCUSSION
Carcinosarcoma also referred as metaplastic carcinoma, sarcomatous carcinoma, pseudosarcoma, and biphasic sarcomatoid carcinoma, are categorized by some studies as a form of malignant mixed tumor.910 The general morphological features show an admixture of carcinomatous and sarcomatous components.1112 Cutaneous carcinosarcoma is an exceedingly rare malignant neoplasm with approximately 120 cases reported to date in the literature; however, this rare tumor may be underreported due to the lack of awareness, tissue sampling variation, and the broad array of clinical and histological phenotypes.1314 Very limited data in Korea are available for patients with cutaneous carcinosarcoma, and those that are available consist primarily of single case reports.151617 We analyzed 11 cases of cutaneous carcinosarcoma, and present the first study of cutaneous carcinosarcoma cases in the Korean population.
Our data were consistent with that of previous studies who reported that the majority of cutaneous carcinosarcomas were observed on the head and neck region of elderly individuals, and this disease had a men gender predominance.918 Similar to SCC or BCC, the predilection for the head and neck of cutaneous carcinosarcoma is related to the sun-damaged skin. Although it has been generally reported that basal cell and squamous cell carcinosarcomas showed a men predominance, as in our study, some carcinosarcomas—such as adnexal carcinosarcoma or cutaneous carcinosarcoma not otherwise specified—have been reported to occur equally between the gender or more commonly in women.13
Several hypotheses have been proposed for the histogenesis of carcinosarcoma, based largely on the pathology of the disease319; first, the collision tumor hypothesis, which proposes the collision of separate neoplasms at the same site resulting in a single neoplasm, based on the fact that skin cancers and malignant fibrous histiocytomas are commonly present in patients with actinically damaged skin; second, the composition hypothesis, which proposes that the mesenchymal component stands for a pseudosarcomatous reaction to the epithelial malignancy; third, the combination hypothesis, which proposes that both epithelial and mesenchymal elements of the tumor originate from a common pluripotential stem cell that undergoes divergent differentiation; and fourth, the conversion/divergence hypothesis, which argues that the sarcomatous component of the tumor represents metaplastic sarcomatous transformation of the epithelial component.31920 Recent immunohistochemical, molecular genetics, and ultrastructural studies suggest and favor the concept of monoclonality in carcinosarcoma from various sites, including uterus, gastrointestinal tract, lung, breast, and bladder.31921 In addition, identical p53 and Kirsten rat sarcoma 2 viral oncogene homolog mutations have been demonstrated in both epithelial and mesenchymal elements of carcinosarcoma, suggesting an early alteration in the histogenesis of the tumor with degeneration of the epithelial element into the sarcomatous element.19
Clinically, cutaneous carcinosarcoma typically arises on sun-damaged skin as a nodular lesion varying in size and often showing ulceration. The duration of these tumors ranges from several months to many years, frequently presenting with early changes.1418 In our study, lesions were commonly presented as nodules with ulceration, ranging from 7 to 50 mm in size and varying duration. Clinical diagnoses of our cases were mainly SCC and BCC. In contrast to carcinosarcomas arising in visceral organs, those primarily arising in the skin do not appear to be necessarily associated with a high mortality rate. Nevertheless, this malignancy has metastatic potential, which is high in the case of penile lesions.22 In a series of 15 carcinosarcoma cases of the penis, inguinal metastases were present in 89% of cases.23 Tumors with adnexal as opposed to epithelial components are high-risk tumors.9 Tumor size > 4 cm has been associated with worse outcome.11 In our study, one patient with penile lesion had metastasis to inguinal LN, while two with 20- and 50-mm sized tumors, respectively, had metastases to regional LNs; however, we did not identify a significant relationship between location or tumor size and aggressive behavior because of the small cohort size.
Microscopically, cutaneous carcinosarcoma is a biphasic tumor composed of malignant epithelial and heterologous mesenchymal components similar to its counterpart in visceral organs, including uterus, lung, bladder, breast, and larynx. About 84%–100% of the reported carcinosarcoma cases have presented both components, but the presence of transition between them has been reported in variable proportion.24 In the present report, all the cases presented both components and approximately 75% of the cases transition. The malignant epithelial components in cutaneous carcinosarcomas comprise SCC, BCC, and malignant adnexal neoplasms including malignant pilomatrixoma, spiradenocarcinoma, and eccrine porocarcinoma, as well as malignant trichoblastoma and Merkel cell tumor.10182526 The mesenchymal component shows histological features of malignancy and consists of spindled and pleomorphic cells showing marked nuclear atypia, necrosis, and numerous atypical mitotic figures. Malignant heterologous mesenchymal elements include osteosarcoma and chondrosarcoma. Only few examples showing skeletal muscle, smooth muscle, myofibroblastic, fibrosarcomatous, or angiosarcomatous differentiation have been reported.272829 The mesenchymal component is scattered throughout the tumor and sometimes focally merges with the epithelial proliferation.30 The epithelial components of our cases were SCC (n = 10) and BCC (n = 1), while the sarcomatous components of all cases were undifferentiated spindle cell sarcomas. No adnexal carcinosarcoma was noted.
Immunohistochemical studies of epithelial and mesenchymal markers are important for diagnosis. Epithelial markers include cytokeratin AE1/AE3, EMA, and keratin18, whereas mesenchymal markers include vimentin, desmin, S-100, and smooth muscle actin, depending on its differentiation.3132 Cytokeratin AE1/AE3 may be negatively expressed in the epithelial component, while p63 protein and MNF116 anticytokeratin antibody (clone MNF116 mouse monoclonal-antibody) are commonly expressed in poorly differentiated epithelial cells.33 The pleomorphic spindle cell population may variably express epithelial markers as our results demonstrated. In our study population, the epithelial markers EMA and cytokeratin AE1/AE3 were positive in the epithelial cells of all cases. Percentage and intensity of staining in tumor cells, which were positive for epithelial markers, varied widely; in some cases, the cells showed diffuse and intense positivity, and in some cases, the staining was weak and focal.34 Vimentin was positive in most of our cases, but S-100 was positive in only one case. None of the cases were positive for desmin. The most controversial aspect of carcinosarcomas is its pathogenesis, the determination of which influences its prognosis and treatment. The epithelial nature of the tumor seems to be strongly supported by the histologic and immunohistochemical expression.21
Diagnosis of cutaneous carcinosarcoma may be difficult and includes a broad differential. The mesenchymal component must be distinguished from reactive or desmoplastic stroma, as well as from atypical fibroxanthoma or spindle cell SCC. Cutaneous sarcomas, such as dermatofibrosarcoma protuberans or leiomyosarcoma, may also enter in the differential diagnosis.8 Cutaneous metastases from high-grade sarcomas of bone and soft tissues are infrequent and only very few cases of primary cutaneous osteosarcoma have been reported in the literature.35 It is essential to recognize the biphasic nature of this neoplasm, including the presence of both malignant epithelial and mesenchymal components, and careful sampling of the tissue is necessary. Metastasis from metaplastic carcinoma of visceral origin constitutes the main differential diagnosis. This is of great importance since metastatic lesions are associated with a much poorer prognosis than primary cutaneous tumors.8
Complete excision of cutaneous carcinosarcoma is the treatment of choice; however, recommended margins are not reported in the literature. MMS has been reported as a treatment option for carcinosarcoma.36 In our study, both WE and initial MMS showed good results. No deaths were reported during the follow-up period.
Since cutaneous carcinosarcoma is a very rare malignancy, leading to misdiagnosis and delays in proper management, a comprehensive clinicopathologic and immunohistochemical analysis of cutaneous carcinosarcomas has not yet been performed in Korea. Although this retrospective study has a small sample size and was limited to a single center, we expect it to make a significant contribution to the diagnosis and management of cutaneous carcinosarcomas in Korea.
 XML Download
XML Download