

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A complex mechanism of the bladder, urethra, and nervous system is involved in the storage of urine and micturition [1]. Therefore, incomplete bladder emptying can result from a wide variety of neurological and urological disorders [23]. In the event of bladder emptying failure, catheterization, bladder expression, reflex voiding, and clean intermittent catheterization (CIC) can be utilized to eliminate urine [4]. Among them, it is known that CIC introduced by Lapides et al. [5] is the gold standard treatment due to a markedly lower incidence of complications such as urinary tract infections and kidney damage compared to all the other treatments [678]. Moreover, CIC is known to be so easy that anyone can perform [9].
However, in spite of benefits, the adherence rate isn't high, variously reported from 20~81% [10111213]. Hence, many studies have been conducted to improve adherence. Some researchers tried to make use of a new catheter, but neither a compact catheter to reduce the burden of carrying nor a lubricated catheter to reduce pain made any differences in the compliance [1415]. Other researchers recommended educational contents and teaching methods [1617181920]. Some of them argued that CIC instructor should evaluate patients' conditions and provide customized education [21]. However, previous studies have only reported the adherence rate related to a disease without mentioning the education contents or methods [101322] or satisfaction with the education program, or whether the patients could perform CIC shortly after the education [1617]. There has been little research about the adherence following the education which contained suggestions and recommendations mentioned above. In the present study, we investigated the adherence to CIC following a CIEP for patients with emptying failure.
METHODS
1. Study Design
This study was a retrospective descriptive study. The purpose of this study was to investigate the adherence to CIC following a CIEP and influencing factors on compliance.
2. Study Participants
We retrospectively reviewed the data in November 2016. The inclusion criteria were as follows: (1) patients aged over 15 years with emptying failure. Emptying failure patients were defined as those who couldn't void at all or could partially void with a large amount (>100 cc) of residual urine. (2) All patients who revisited the CIC clinic for follow up between January 2012 and July 2014. This study was undertaken in a tertiary referral center, and all patients in need of CIC were referred to the CIC clinic in the hospital.
3. Study Protocol
The CIEP on CIC was created at the research hospital in 2011. Since then, all patients who were prescribed CIC have learnt the procedure through the program. It was based on previous protocol [16]. Some of the protocol has been modified on the basis of many research findings. It was made up of theoretical knowledges and hands-on practice. Total education time was approximately one hour, and the education was provided one-on-one in a separate space.
The nurse in charge of education completed a Ph.D. program and had more than 15 years of clinical experience. She has attended a conference with peer group and of physicians every month; and lectured as an expert in the urology academic society every year.
The program consisted of watching video, customized theoretical knowledges instruction, and hands-on practice (Table 1). Before education, the nurse checked a medical record such as results of urodynamic study, ultrasonography, and underlying disease or surgery record.
At first, a patient watched a video for an overview of CIC. The video lasted for 7 minutes.
After watching the video, customized theoretical knowledges instruction was provided based on the disease states and test results individually. The nurse explained the patient's underlying disease and how the underlying disease cause the emptying failure in detail. In addition, the nurse stressed the advantage of CIC and disadvantage of other methods including the mechanism which complications occur. The patient was educated about the CIC thoroughly.
The next course was a hands-on practice. Before practice education, the nurse checked the patient's physical condition and the structure of the toilet of the patient's house. The nurse explained the process as simply as possible in order not to make it strike the patients as a cumbersome technique. They were taught differently depending on the sex: man in the standing position and a woman in the sitting position on a toilet, respectively. The nurse found the most appropriate posture for the catheterization with the patient and taught various ways to locate the urethra. If the patient had poor vision, she taught the ways to locate the urethra by touch. Except for the patients who were bed-ridden and quadriplegic, she encouraged them to catheterize themselves. The practice session continued until the trainee was able to master the technique.
When the education was over, each patient received a questionnaire about the degree of understanding, satisfaction with the education, and degree of confidence that he/she could catheterize alone; and the most inconvenient procedures. Additionally, the nurse asked the patient about the process of catheterization and what he/she needs to know using short answer questions; if the patient answered incorrectly, the nurse explained it again. At the end of the program, the nurse encouraged the patient to express his/her feelings freely and consulted. If the patient wanted additional counselling after returning home, the patient could call the nurse during office hours.
To check the patients' voiding conditions and compliance, the urologist advised them to revisit the urology clinic no later than one month after the completion of the education. When they revisited, the interview was done via a questionnaire. It included questions about who performed the catheterization, how it was done, or what made the subjects compliant or noncompliant. If the CIC method was not correct, re-education was provided.
4. Data Collection
We collected clinical characteristics of patients such as
age, sex, income, education level, occupation, hand dexterity, performance status, primary reasons for emptying failure and voiding status. Among the primary reasons for emptying failure, hysterectomy and low anterior resection was categorized as peripheral nerve injury, and diabetes and peripheral neuropathy were categorized as systemic disease. The voiding status was divided into partial emptying failure and complete emptying failure.
For the short-term adherence rate, answers to the questionnaire and voiding diary in medical records on the second visit were analyzed. The question of questionnaire was “Did you perform CIC as the doctor ordered?” Of the 6 scale answer to the question, ‘somewhat yes’, ‘almost yes’, ‘completely yes’ were categorized as adherent. The medical records and voiding diary in medical record on the last follow-up day were analyzed for the long-term adherence rate. We reviewed the medical record in November 2016. The case that self-voiding was restored and regular catheterizing was performed until the last visit were categorized as adherent. If the last follow-up day was over 6 months, they are categorized follow-up loss and non-adherent.
The level of understanding, satisfaction, and confidence after first education and barrier to CIC were also collected. Finally, we investigated the influencing factor on adherence.
We obtained approval from institutional review board of Seoul National University Hospital (No: H-1408-002-596). This study was exempted from receiving consent because it is unlikely to cause harm to subjects
5. Data Analysis
Descriptive analysis was conducted for description. For the difference in urologic anatomy and urination process by sex, we classified the subjects into male and female groups. Chi-sure or Fisher's exact test for categorical variable and student's t-test for continuous variable were used to compare differences between groups. We evaluated potential influencing factors on the adherence: adherent and non-adherent. These variables were sex, age, the level of education, income, occupation, primary reason for emptying failure, the level of understanding, the level of satisfaction, the level of confidence. Statistical analyses were done with the SPSS software (Statistical Package for the Social Sciences, version 21.0, SPSS Inc.), and a p-value of < 0.05 with a 95% confidence level was considered statistically significant.
RESULTS
1. Characteristics of Patients
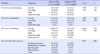
The average age was 65.25±14.18 years and the man was older (p=.002). 62.4 % of patients were men. Unemployment (51.1%) in male and housewives (68.2%) in female were the most common. About 72% of the male and 64.7% of the female patients had a good dexterity of the hand. 56.6 % of patients could walk without help. 77.0% of patients could perform self-catheterization after the first session of education. The most common primary reasons for emptying failure were urologic disease (32.6%) in male and spinal cord lesions (30.6%) in female. Most of the patients with unknown etiologies were in a bedridden state. Demographic and clinical characteristics of the patients are presented in Table 2.
2. Response to Initial CIC Education
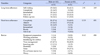
Most of the patients showed a high level of understanding, satisfaction, and confidence. The level of confidence of male was higher than female (p=.014). The most uncomfortable process was significantly different depending on the gender (p<.001). The male patients thought cleaning the perineum caused the most discomfort while the female patients thought identifying the urethra caused the most discomfort. The male patients complained about a sense of discomfort during the insertion of the catheter much more than the female patients (Table 3).
3. Adherence Rate and Barrier
At the second visit, the median duration was 22days, adherence rate was 87.6%(198 of the 226). 28 patients were non-adherent and 16 of 28 did not performed CIC at all. The degree of short term adherence was different by gender (p=.031). The major barrier was time management (44.7%), followed by none (24.8%). Although the number decreased, male still had difficulty inserting the catheter and female patients had difficulty identifying the urethra. The number of people who said there was no difficulty has grown from 23 to 56.
The long-term, the median time was 112 days, adherence rate was 50.4%. Ten of the 30 patients who stopped catheterization on their own authority were too seriously ill to perform CIC and had to switch to indwelling catheterization. And nine of the 51 follow-up loss patients were stable, so referred to the primary clinic where the patient lived (Table 4).
4. The Influencing Factor on Compliance
According to univariate logistic regression analysis, only income variable was associated with adherence (OR: 3.08 [95% CI=1.58~5.99], p=.001), so we couldn't perform multivariable logistic regression analysis. The other variable did not show any significant difference between the two groups (Table 5).
DISCUSSION
We evaluated the adherence to the CIC following the CIEP and influencing factors on the adherence. The shortterm adherence rate (median 22 days) was 87.6% and the long-term adherence rate (median 112 days) was 50.4%. The biggest obstacle was the time management. Only income variable differed significantly between the two groups.
The ongoing CIEP of our clinic were devised by adopting the recommendations suggested by other studies [181920]: providing an overview of the anatomy using educational materials, voiding symptoms, underlying disease and identification of psychological issues, physical problems and consult about them. Additionally, we tried to provide education in a silent and low stress setting and not to give up teaching disabled patients. We spent sufficient time trying to educate the subjects completely. Plain explanations for information on emptying failure and the CIC process that fits the intellectual level of each patient using various audiovisual aids may be helpful. Using various methods to teach how to resolve difficulties in finding the urethra enabled patients to perform the catheterization. Consequently, the level of understanding, satisfaction, and confidence was very high.
Parsons et al.[23] reported that the short term (6 weeks) adherence rate of 309 patients with non-neurogenic bladder was 84%. This is similar to the result of this research. The long-term adherence rate of existing studies was varied [6242526]. The research of Bolinger & Engberg [24] reported that after 60 months, the compliance rate was 76.9 %. However, only 10.2 % of the patients performed CIC according to the doctor's prescription, the remainder catheterized relying on their perception. In presenting study, 50.4% patients performed CIC according to the doctor's prescription. In another study which the study participants were children (60 boys), the long term adherence (9.9 years) was 82%. They claimed that their high adherence rate was due to the constant involvement of an experienced nurse [25]. In this study setting, tertiary hospitals, referral to the primary clinic where the patient lived was common. These feature may influence the low long-term adherence rate. Motavasseli et al.[26] reported the adherence rate (median 42 weeks) of 35 patients with multiple sclerosis was only 29%. The median Expanded Disability Status Scale, EDSS is a method of quantifying disability in multiple sclerosis, of the participants was 6.0. The score 6.0 means the condition that the patients requires a walking aid - cane, crutch, etc. - to walk about 100m with or without resting [27]. The performance state of the study participants was worse than this study participants, 56.6% patients could walk without help, so their adherence may be lower than presenting study.
Discomfort due to CIC changed over time; from storage and irrigation of the catheter, washing the urethra and perineum, and identifying the urethral orifice to the time management. In other studies, the most common barriers associated with CIC were the difficulty of using a bathroom; positioning to insert the catheter [2426]. This means that the vague anxiety about catheterization disappears over time, but having a social life with catheterization, incorporating catheterization into daily routines and being able to perform the procedure properly both outside and inside home are continuous challenges [202829]. So the instructors should provide realistic tips as well as other alternative tips for balancing the catheterization and social life.
The previous literature reported that cost was barrier for CIC [24]. These results are also found in other health behavior-related studies [30]. However, the impact is expected to have been reduced with insurance coverage in 2017.
Girotti et al. [10] reported that the adherence rate (6 month) was 61.7% and higher in women and under the age of 40; and Motavasseli et al. [26] reported more severe voiding dysfunction measured using the Urinary Symptom Profile was associated with adherence. However, there was no difference in sex, age, voiding status between adherents and non-adherents in this study. They also reported that emotional (depression), psychological status and social relationships were associated with adherence. However, the psychological and emotional factors were not analyzed in this study; this might be why we could not find influencing factor except income variable.
At the first follow-up, 10 patients did not perform catheterization; however, after consultation, they performed catheterization well. On the other hand, 29 patients who could catheterize at the clinic gave up self-catheterization at home and the adherence rate decreased over time. These phenomena are good examples that show the importance of continuing education and consultation [1920]. Faure et al. [25] reported that contact with the patients and request to visit the clinic regular intervals was very important in increasing adherence. In addition to the education, therefore, other methods such as emotional and psychological support [1026], and regular follow-up [25] are needed to improve long-term adherence.
This study has a limitation that must be considered. This study is a retrospective study. However, the analysis data that were prospectively designed for patient education and information on CIC could decrease the limitation for this retrospective study. A prospective study needs conducting in a larger population to identify the overall adherence rate and barrier by periodic checks on the performance of catheterization, voiding status, and reasons for cessation.
CONCLUSION
Although satisfaction with the CIEP for CIC was high, the adherence rate was not high. And we couldn't find the influencing factor on adherence except income. This could be because of the psychological reluctance concerning CIC which intrinsically differ from natural toileting practices. So, it is very necessary to provide constant emotional and psychological support and education until the patient can accept the CIC. For this, a policy to apply insurance to the CIC education must be established.



 XML Download
XML Download