

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Disseminated Mycobacterium avium complex (MAC) infection appears late in the course of human immunodeficiency virus (HIV) disease and is an independent predictor of mortality, even after adjusting for CD4 T cell count [1]. In recent years, the annual rate of disseminated MAC has fallen substantially owing to the availability of highly active antiretroviral therapy (HAART) [2]. However, during the initial months of HAART, immune reconstitution is complicated by an adverse clinical phenomenon in which either previously subclinical infections are “unmasked” or pre-existing partially treated, opportunistic infections deteriorate. This immune reconstitution inflammatory syndrome (IRIS) has been associated with various medical conditions. Non-tuberculous mycobacterium (NTM)-associated IRIS is one of the most difficult to diagnose and manage. Even with intensive anti-NTM chemotherapy, the prognosis is often poor due to the absence of a standard treatment [3]. The diagnosis of IRIS is often challenging because its clinical presentation is nonspecific and is complicated by opportunistic infections, drug failure, toxicity, and malignancies. The most common IRIS-associated symptoms of fever, lymphadenopathy, and pulmonary symptoms [3], resemble those seen in patients with acquired immunodeficiency syndrome (AIDS)-related lymphoma (ARL) [4]. In addition, the recently reported high ARL rates shortly after initiation of the newer-class of antiretrovirals [5], makes the distinction between ARL and IRIS important.
We present the case of a patient who following anti-NTM chemotherapy and HAART, exhibited symptoms resembling ARL that were diagnosed as IRIS.
Case report
A 43-year-old man visited the emergency department owing to 3 days of dyspnea and had a history of tuberculosis (TB) in his 20s. A chest computed tomography (CT) at this time showed diffuse ill-defined ground glass opacities in both lung. A pneumocystis pneumonia (PCP) polymerase chain reaction (PCR) test on the bronchoalveolar lavage fluid returned positive result. Moreover respiratory virus multiplex PCR, acid-fast bacilli (AFB) stain, TB PCR, gram stain, and culture returned negative results, we confirmed our diagnosed of PCP. He was treated PCP with trimethoprim (15 mg/kg), sulfamethoxazole (75 mg/kg) combination (TMP-SMX) in addition to prednisolone (PD; 80 mg/day). His CD4 T cell count was 31 cells/µL, an HIV antibody reveled positive and an HIV PCR was a viral load of 47,800 copies/mL. After 9 days of admission, he was discharged.
Twenty-one days after his first visit, an HIV western blot test returned positive results, and we started HAART with tenofovir disoproxil (245 mg/day), emtricitabine (200 mg/day), elvitegravir (150 mg/day), and cobicistat (150 mg/day). However, he has stopped taking the medications after 7 days due to diarrhea. Thirty days after his first visit, we restart HAART with emtricitabine (200 mg/day), tenofovir disoproxil (300 mg/day) and raltegravir (800 mg/day). His CD4 T cell count had increased to 60 cells/µL, and the HIV viral load had decreased to 3,690 copies/mL (Fig. 1).
Figure 1
The series of CD4 cell count and HIV RNA PCR level. The arrows indicate the date of important medication or procedure were conducted.
HIV, human immunodeficiency virus; RNA, ribonucleic acid; PCR, polymerase chain reaction; NTM, non-tuberculous mycobacterium; ABC, abacavir; 3TC, lamivudine; RAL, raltegravir; TDF, tenofovir disproxil; FTC, emtricitabine; LN, lymph node; EVG, elvitegravir.

Sixteen days after starting HAART, he was hospitalized with continuous loose stools and new-onset fever. We suspected a drug side effect, and changed his second-line antiretroviral therapy (ART) to abacavir (600 mg/day), lamivudine (300 mg/day) and raltegravir (800 mg/day). Even though his diarrhea resolved with this change in treatment, his fever persisted (38°C). His white blood cell count was 5,340 cells/mm3, C-reactive protein level was 181 mg/L, and procalcitonin level was 2.08 ng/mL. His chest CT scan demonstrated a decrease in the bilateral ground glass opacities; however, new peribronchial consolidations were seen in both upper lobes. Abdomen/pelvic CT scan exhibited borderline size of paraaortic, aortocaval, retrocaval, and mesenteric lymph nodes (LNs) (Fig. 2). A transthoracic echocardiography did not reveal any evidence of vegetation. For further investigation, bone marrow biopsy was performed. It showed non-caseous necrosis and AFB (Fig. 3); however, the TB-PCR test result was negative. In his sputum culture, MAC was cultivated.
Figure 2
Abdomen/pelvic computed tomography axial plane shows multiple borderline size lymph nodes, paraaortic, aortocaval, retrocaval, and mesentery (red arrows).(Sixteen days after starting HAART).
HAART, highly active antiretroviral therapy.

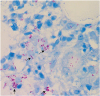
Figure 3
Bone marrow biopsy specimen revealed positive staining for acid fast bacilli.ositive (black arrows). (Ziehl-Neelsen stain, x 400).
Accordingly, the patient was diagnosed with MAC in his sputum and bone marrow, and anti-MAC chemotherapy with rifampicin (450 mg/day), ethambutol (400 mg/day), clarithromycin (500 mg/day), and levofloxacin (500 mg/day) was started. His fever subsided with anti-MAC chemotherapy and he was discharged 3 days after starting anti-MAC chemotherapy.
Thirty four days of starting anti-MAC chemotherapy, he presented at the outpatient department with abdominal pain. Abdomen/pelvic CT (Fig. 4) showed multiple enlargement mesenteric LNs and hepatosplenomegaly. After a week of abdominal pain and fever (38.3°C), he was readmitted to the hospital. We performed a positron emission tomography (PET)-CT scan (Fig. 5A and 5B) for excluding the possibility of a lymphoma. The scan images showed multiple enlarged hypermetabolic LNs in the mesentery and retroperitoneum of the abdomen, right retrocrural, right lower paratracheal, subcarinal, and right hilar areas, along with diffuse hypermetabolic activity in the spleen and bone marrow. The maximum standard uptake value (SUV) was 13.4. The patient's ferritin level was > 1,650 ng/mL, and lactate dehydrogenase (LDH) level was 306 IU/L. We next performed laparoscopic biopsy of the mesenteric LN, and a histological examination of the biopsy specimen revealed partial necrosis (20%); however, no typical granulomas, giant cells, or severe acute and chronic abscesses were found. An AFB staining yielded a positive result, and the biopsy culture grew MAC that was susceptible to macrolides. We started treating him with PD (40 mg), and his abdominal pain and fever resolved. He was discharged on 11th hospital day, and his medication at this time included antiretroviral and antitubercular drugs, along with the steroid.
Figure 4
(A) Abdomen/pelvic computed tomography axial plane shows multiple lymph nodes enlargement along mesentery (red arrows, Thirty four days of starting anti-MAC chemotherapy); (B) Abdomen/pelvic computed tomography shows multiple lymph nodes enlargement along mesentery (red arrows).
MAC, Mycobacterium avium complex.

Figure 5
(A) Positron emission tomography image shows multiple enlarged hypermetabolic LNs in mesentery and retroperitoneum of abdomen, right retrocrural area (maximum standard uptake value = 13.4), right lower paratracheal, subcarinal and right hilar area and diffuse hypermetabolic activity in spleen and bone marrow (red arrows); (B) positron emission tomography/computed tomography image.

Eight months of starting anti-MAC chemotherapy, abdomen/pelvic CT (Fig. 6) demonstrated a slightly decreased multiple enlarged LNs were still present. We accordingly recommended treatment continuation; after 4 months of anti-MAC chemotherapy, his symptoms subsided completely, and the steroid was discontinued. In a final drug susceptibility test, minimal inhibitory concentrations were 2 µg/mL for clarithromycin, 32 µg/mL for ethambutol, and 4 µm/mL for rifampin.

Discussion
The present case emphasizes, the importance of considering a diagnosis of IRIS in AIDS patients, when there is a new symptom or aggravation of an existing symptom.
In this case, we experienced two IRIS event: first, unmasked IRIS after the initiation of ART. second, paradoxical IRIS result from anti-MAC chemotherapy. Unmasking IRIS is defined as the presentation of a new disease within the first 3 months of ART [6]. In our patient, we diagnosed a disseminated MAC infection on 17th day of after ART initiation. There are several cases where an unmasked IRIS was reported within 2 weeks of HAART initiation [7, 8]. Even though our patient's medication was stopped for 3 days, the total duration of medication was 2 weeks at the time of fever. Ten days after ART initiation, his CD4 T cell count increased from 31 cells/mm3 to 60 cells/mm3. Based on these facts, we thought it was unmasked IRIS with MAC and started anti-NTM treatment.
Paradoxical IRIS occurs in HIV-infected patients with very low CD4 T cell counts at ART initiation; the exact underlying mechanism is not fully understood [9]. As many as 31.4% of MAC infected patients develop IRIS after the initiation of ART [10]. MAC-IRIS occurs in about 3.5% of all HIV-infected patients treated with ART, and 20% of the MAC-IRIS cases are fatal [11]. Our patient's abdomen/pelvic CT showed homogeneous enhancement and enlargement of the paraaortic, aortocaval, retrocaval, and mesenteric LNs. Even though LNs are invaded in HIV infection, the sites of invasion are typically the cervical, axillary, and inguinal LNs, with the median number of invasion sites being 3 (range 1-7) [12]. Homogeneous LN enhancement is seen in lymphoma, whereas peripheral enhancement is observed in TB [13]. Up to 10% of HIV-infected patients develop non-Hodgkin's lymphoma [14], and our patient's elevated ferritin and LDH levels suggested the possibility of a lymphoma and we conducted a PET-CT to confirm this. A variety of infections and malignancies can result in increased FDG uptake [15]; however there are disease-specific differences in the uptake pattern. Our patient's SUV max was 13.4, while in lymphoma, the reported median SUV max is 12.8 [16]. HIV infection itself, can result in increased FDG uptake in the LNs; however, here the reported average SUV mean values are 3.4 (range 1.8-9.0) [12]. In MAC infection, macrophages are activated and play an important role in the formation of granulomas which increases the FDG uptake, and consequently, PET-CT scans show enhanced FDG uptake in patients with MAC infection. The average SUV max for LNs in NTM infection is 3.59 ± 2.32 (range 1.14 - 9.01), while for TB infection, this value is 7.23 ± 3.03 (range 1.78- 15.72) [17]. Based on our patient's abdomen/pelvic CT and PET-CT finding, we suspected a lymphoma and conducted a LN biopsy that revealed LN involvement of MAC. There has been one reported case of MAC-IRIS where the SUV max was 18.42 [18]. Therefore, a PET-CT is not sufficient to distinguish between a lymphoma and a LN involvement of MAC-IRIS [19], even though it has been an important clinical tool for diagnosing, staging, and monitoring cancer over the last several years [20]. As we have seen, the clinical signs and symptoms of IRIS overlap with those of ARL [4], and it is important to distinguish between the two diseases. Moreover, pathology and culture results remain important for an accurate diagnosis of IRIS.
In the present case, the pronounced LN enlargements and increased FDG-uptake were indicative of ARL; however, as we have shown, the presence of HIV should always increase the index of suspicion for pathologies other than lymphoma. The present case further illustrates the pitfalls of standard techniques, including 18F-FDG PET-CT scan and microscopic examination of biopsies in the setting of HIV, In conclusion, if an HIV-infected patient with a low CD4 T cell count develops signs of ARL shortly after the initiation of HAART, clinicians must consider IRIS as a possible cause. In such cases, definitive diagnostic LN excisional biopsy is mandatory.
 XML Download
XML Download