

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The mandibular position has been reported to be influenced by head and body posture.1234 The standard patient posture recommended in patients undergoing an occlusal procedure is to sit straight with the head in a natural position.5678 However, we often observe that patients turn their face unconsciously toward the dentist during clinical procedures even though they are sitting straight.9 This could alter the basic mandibular position that the patient uses daily and could therefore spoil the construction of a correct occlusal relationship. Mandibular positions should be in physiological harmony with the stomatognathic system. An inappropriate mandibular position caused by an incorrect occlusal record registration or occlusal adjustment could result in damaged teeth and may also cause functional disorders in muscles and temporomandibular joints.10111213
The mandibular position can be measured using a three-dimensional jaw movement measurement device with six degrees of freedom called the WinJaw System. The WinJaw-System is compact and easy to use from the dental chair, and it can be used to simultaneously analyze even the smallest deviation in condylar and incisal points.81415 The marker that is attached to the mandible is very light, having a weight of only 55 g; therefore, the influence of the marker on the measured value is assumed to be small. Nakajima et al.8 verified the accuracy of this device for measuring mandibular micro deviations. This device has another advantage in that it can acquire measurements without any direct contact, and it therefore does not influence the measurements.
Dental therapies include examinations, diagnostic procedures, and treatments that are performed with the patient in various body postures and the head in different positions. Some studies have investigated the effect of lateral head tilt on mandibular position.8,16,17,18 For example, Nakajima et al.8 investigated the effect of lateral head tilt on mandibular position and concluded the following: the condylar point on the side of the extended neck increased deviation in line with the head tilt angle and had a significant affect on the reference point when the head tilt angle was more than 10°, and the incisal point also showed a significant increase in deviation in the forward direction and a tilting of direction when the head tilt angle was more than 10°. Other studies have reported that lateral head tilting causes mandibular deviation in the tilting direction.116 Those authors have suggested that the main factor contributing to mandibular shifting is the influence of gravity.817 However, a few studies have been conducted to explore the influence of horizontal cephalic rotation (HCR) on mandibular position.192021 The present study was performed to clarify the influence of HCR on mandibular position by investigating the three-dimensional positions of condylar and incisal points.
MATERIALS AND METHODS
Forty dentate subjects (20 males and 20 females with a mean age of 25.8 ± 2.1 years old) with normal positional relationships of the upper and lower first molars and no stomatognathic dysfunction, such as functional disorders of the muscles and temporomandibular joints, were selected as subjects for this study. They were fully informed of the purpose of the study and provided informed consent to participate. The present study was approved by the Ethics Committee of The Nippon Dental University School of Life Dentistry at Niigata with the approval number ECNG-H-182.
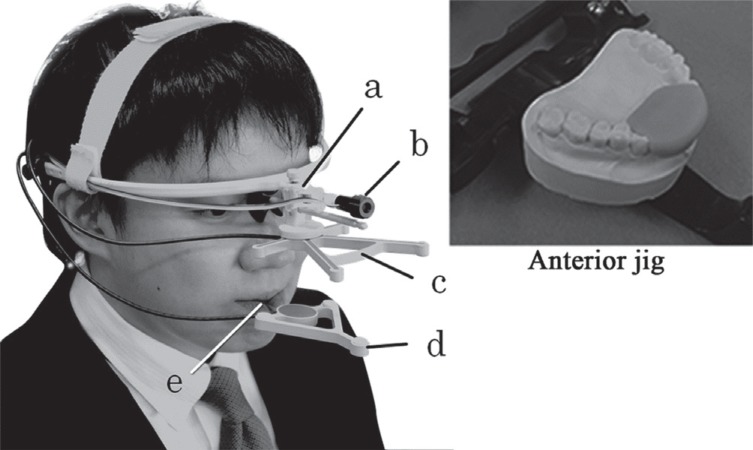
To measure the condylar and incisal points, a three-dimensional jaw movement measurement device with six degrees of freedom called the WinJaw System (Zebris, Aachen, Germany) was used (Fig. 1). A paraocclusal clutch designed to fix the marker of the WinJaw System was made on the cast model with room temperature curing resin (Pattern Resin, GC, Tokyo, Japan) and attached to the labial and buccal sides of the mandible dentition with poly-carboxylate cement (Hybond Temporary Cement, Shofu, Kyoto, Japan). An anterior jig22 was fabricated on the cast model and mounted on an articulator with room temperature curing resin (Tray Resin, Shofu, Kyoto, Japan) (Fig. 1). A flat table with an approximately 5 mm diameter was placed parallel to the occlusal plane around the tapping point to obtain the natural head position.8 An increased vertical dimension of occlusion of less than 3 mm was made using the jig.6822
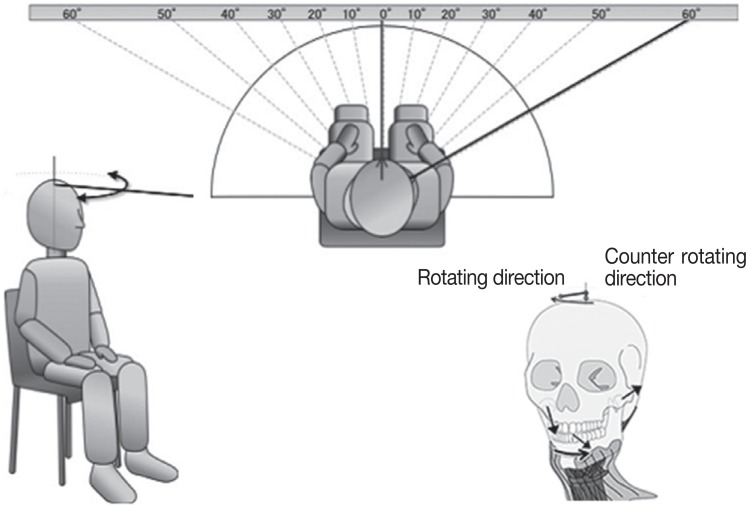
The subjects were asked to sit straight without leaning against the backrest. The head was kept in a natural position without any fixation according to the method of Ohta et al.5 Indicating lines were drawn on the wall that faced the subject so that the rotational angles could be determined by locating the center on the head of the subject. The subjects wore the WinJaw System and the anterior jig. A red light made by a laser irradiation apparatus was mounted on the tip of the face bow to measure the cephalic rotational angle (Fig. 1). The subjects were instructed to move the red light to meet the indicating line by rotating their head horizontally. There were seven rotating conditions, including 0°, 10°, 20°, 30°, 40°, 50°and 60°, in each direction (right or left) because the occlusal position was reported to start shifting at a 30° angle of HCR,19 and the limitation of HCR was reported to be a 60° to 70° angle (Fig. 2).20 The measuring order was randomized for each condition. The natural head position was adjusted to a 0° angle as the reference position.
In the present study, the condylar points were defined as the points located at the inner 68.4%23 of the distance on the line connecting Beyron's points24 on both sides. Beyron's point is an imaginary point on the face that is located 13 mm from the posterior edge of the tragus along the line that connects the vertical midpoint of the posterior edge of the tragus and the outer canthus point. This measurement point is very close to the actual condyle and more accurate than an assumed point on the skin surface for recording deviations. The incisal point was defined as the midpoint of the line that connects the mesioincisal angle of the bilateral central incisors. For each angle condition, the deviational data obtained from the reference points on the coordinate axes were recorded while tapping was performed 10 times at a speed of 3 times per 2 seconds for each measurement while the mouth was open for a width of approximately 10 mm.6825 The reference points were the condylar points located on both the rotating direction side and the counter-rotating direction side and the incisal points. Measurements were performed three times for each condition. The mean values were calculated and analyzed.
Analyses were performed with the condylar points at each of the following coordinate axis: the X-axis indicates movement in the anteroposterior axis (anterior: +, posterior: −), the Y-axis indicates right and left movement (rotating direction: +, counter rotating direction: −), and the Z-axis indicates movement in the vertical axis (upward: +, downward: −). Concerning the incisal point, analyses were performed for the X-axis, which indicated movement in the anteroposterior direction, and the Y-axis, which indicated movement in a lateral direction. Statistical analysis software (SPSS 17.0, SPSS JAPAN, Tokyo, Japan) was used for all analyses. The Friedman test was used to analyze deviations of the condylar points in the rotating and counter rotating direction sides toward any direction along the X, Y, and Z axes and deviations of the incisal point toward any direction along the X and Y axes during each angle condition of HCR. When the Friedman test identified a significant difference, a multiple comparisons Wilcoxon signed-rank test was performed with Bonferroni inequalities.
RESULTS
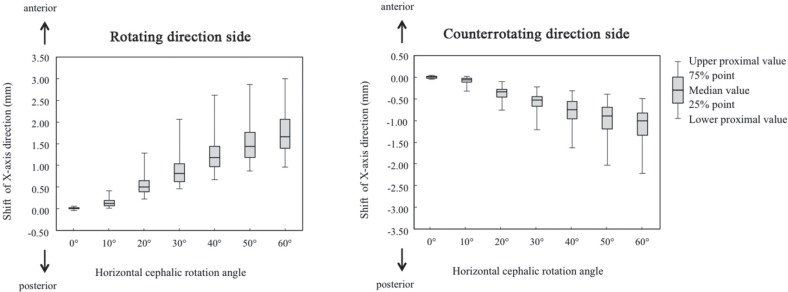
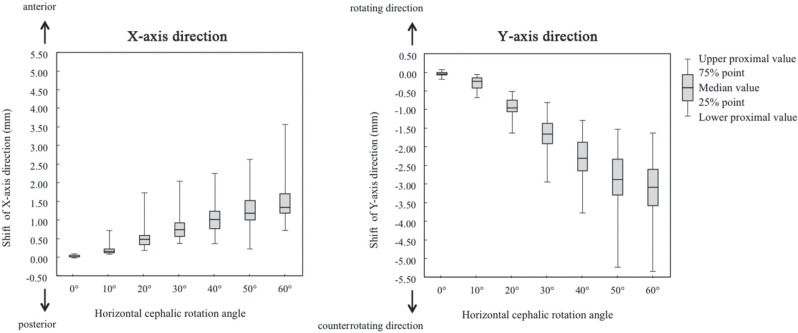
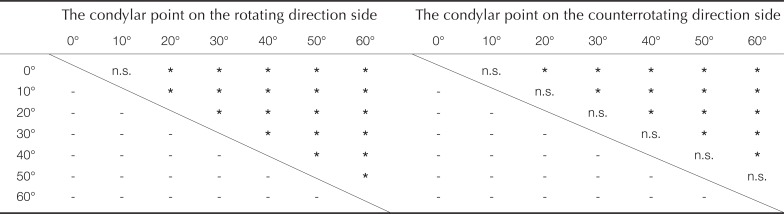
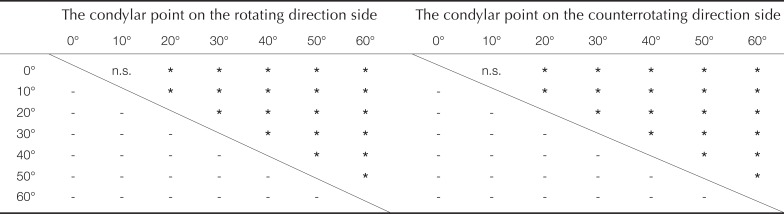
Figure 3 shows the deviations observed at the condylar points along the X-axis. As the rotational angle became larger, the condyle on the rotating direction side tended to move forward, while that on the counterrotating direction side tended to move backward, and the deviation increased. The results of multiple comparison tests are shown in Table 1. A significant difference was found for angle conditions higher than a 20° angle.
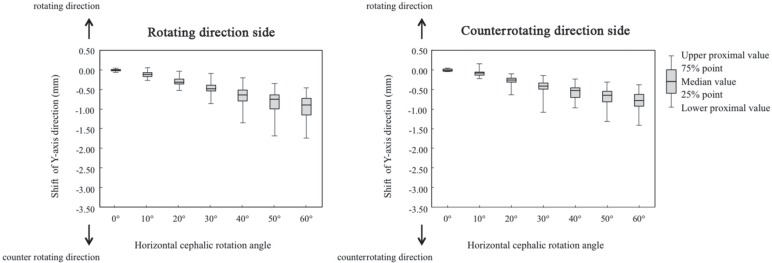
Figure 4 shows the deviations observed in the condylar points along the Y-axis. As the rotational angle increased, the condyle on either side tended to move toward the counterrotating direction side and to increase the deviation. The results of multiple comparison tests are shown in Table 2. A significant difference was found for angle conditions higher than a 20° angle.
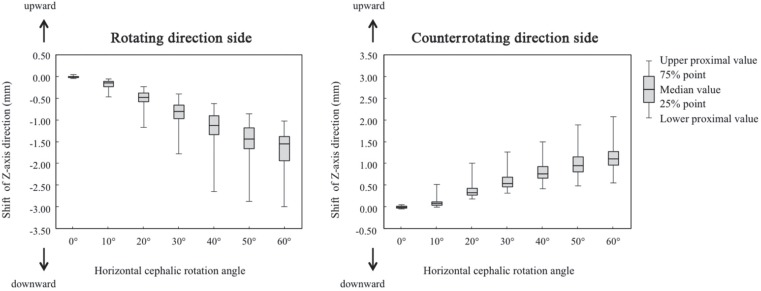
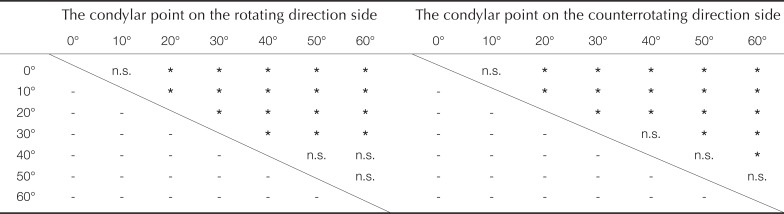
Figure 5 shows the deviations observed in the condylar points along the Z-axis. As the rotational angle increased, the condyle on the rotating direction side tended to move downward, and the condyle on the counterrotating direction side tended to move upward as the deviation increased. The results of multiple comparison tests are shown in Table 3. A significant difference was found for angle conditions higher than a 20° angle.
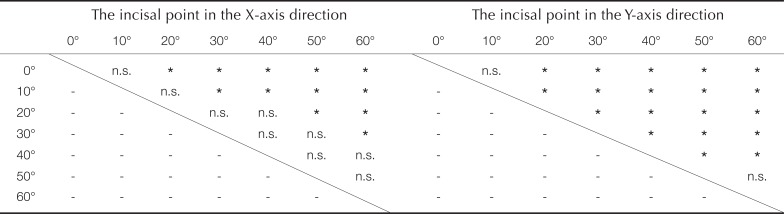
Figure 6 shows the deviations in the incisal point. As the rotational angle increased, the incisal point tended to move forward and in a counterrotating direction as the deviation increased. The results of multiple comparison tests are shown in Table 4. A significant difference was found for angle conditions higher than a 20° angle.
DISCUSSION
In this study, we examined the influence of horizontal cephalic rotation (HCR) on mandibular position by investigating the three-dimensional positions of condylar and incisal points. In accordance with HCR, the condylar point on the rotating direction side shifted forward, downward, and toward the inside, while the condylar point on the counterrotating direction side shifted backward, upward, and toward the outside. The incisal point shifted forward and toward the counterrotating direction side. For angles of rotation higher than 20°, the deviations in the condylar and incisal points were significantly different from the reference position observed at a 0° angle. These findings are in agreement with previous reports by Kuraishi et al.19
Winnberg et al.18 reported the positions of the masseter muscle, suprahyoid muscles, and hyoid bone during the opening and closing cycle of movement in the mouth to analyze the flexion and extension of the head. They concluded that an altered head posture caused the compression and extension of soft tissues associated with the mandible. Therefore, the stress released in the soft tissue may change the patterns of activity observed in mouth opening and closing muscles. During HCR, compression seemed to be produced in soft tissues associated with the mandible on the rotating direction side, and simultaneous extension may have been produced on the counterrotating direction side. For example, when a head was rotated to the right, the cranium moved to the right, and the hyoid bone was relatively positioned to the left. Then, the mandible was pulled to the left by the suprahyoid muscles (which are attached to the mandible and hyoid bone), infrahyoid muscles (attached to the hyoid bone), platysma muscle, and skin.19 The condyle on the right side would then shift forward, downward, and toward the inside, while the condyle on the left side would shift backward, upward, and toward the outside.
The major muscle involved in HCR is the sternocleidomastoid muscle, which is the largest muscle in the lateral region of the neck. On the counterrotating direction side, this muscle contracts to rotate the head horizontally.21 Some patients with temporomandibular disorder experienced pain caused by occlusal disorder in the muscles of the neck region, especially the sternocleidomastoid muscle. A previous study reported that these symptoms disappeared after occlusal therapy.10 Another report indicated that the muscle memories caused by occlusal contact (called “engrams”) are mainly based on sensory information and are influenced by the mandibular position.1125 This phenomenon suggested that occlusal disorder caused tonus in the sternocleidomastoid muscle, inducing cephalic rotation. Some reports have shown that alterations in head position can cause occlusal disorder.12 Additionally, occlusal disorder may directly influence the growth of the mandibular condyle;13 necessitating adequate observation or care.
In clinical dentistry, the majority of dental examinations and treatments are performed while the dentist is standing on the right side or to the right and forward of the patient sitting in the dental chair unit. One report showed that patients tended to rotate their head position significantly to the right side within an instant of their sitting on the dental chair. In addition, when the dentist stands by a patient, the patient's head will rotate even more to the right.9 Sometimes, patients are very cooperative and turn their face toward the dentist to provide a good view of their mouth. In these situations, the patients may possibly rotate their head to the right, inducing a deviation in the mandibular position and potentially jeopardizing the examination and any subsequent treatment. Thus, during dental treatments involving occlusion, such as registration of the occlusal relationship and occlusal adjustment, it is essential to consider the possibility of a deviation in the mandibular position. In addition, the results of the present study strongly suggest that there is a relationship between occlusion and posture in sports. Many sports, such as baseball, golf, and archery, need to be played with the head in a rotated position, making it easy to imagine that while playing these sports, the occlusion is shifted from a routine position. Further research on the relationship between occlusion and the cephalic posture may improve performance and prevent abnormal postures and injuries.
CONCLUSION
The results of this study make it clear that a horizontal cephalic rotation with an angle of more than 20° causes the condyle on the rotating side to shift forward, downward, and toward the inside and the condyle on the counterrotating direction side to shift backward, upward, and toward the outside. The incisal point shifted toward the forward and counterrotating directions during horizontal cephalic rotations with an angle of more than 20°. Therefore, it is necessary to consider this deviation in the mandibular position when performing an occlusal procedure.

 XML Download
XML Download