

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In the USA, approximately 92% (300,000) of patients with cardiac arrest die, and the deaths are attributed to the increasing number of cardiovascular diseases, which are considered major health problems owing to the rapid increase in the elderly population and influence of western lifestyle.1 Despite several efforts for improving the survival rate of patients with cardiac arrest in the community, and despite the reduced mortality rate of most cerebrovascular diseases, the survival rate of patients with acute cardiac arrest remains low.
In cardiac arrest, because irreversible brain damage occurs within 4–5 minutes, bystanders who witness a cardiac arrest should start cardiopulmonary resuscitation (CPR) as soon as possible to minimize brain damage in case of recovery. Research has shown that early access to emergency services, prompt defibrillation, and high-quality CPR significantly affect the survival rate of patients with cardiac arrest.23
Furthermore, when a bystander performed CPR for patients with cardiac arrest, the survival rate was 2–4 times higher compared to when CPR was not performed.45 The bystander CPR rate during witnessed cardiac arrest in Korea is approximately 12%,6 which is lower than that in the USA (54%), Denmark (45%), and Singapore (42%).789 The instructions provided by the dispatcher before the arrival of the ambulance were effective in increasing the bystander CPR rates by witnesses, and this result was presented in several studies.101112
In addition, in the 2010 American Heart Association guidelines, the dispatcher is an important team member in the initial emergency treatment of patients with cardiac arrest. Moreover, the guidelines recommend that all dispatchers should receive appropriate education to provide standardized, medically approved CPR instructions over the telephone.13 We expect that a standardized telephone CPR program will increase the rates of bystander CPR and improve good neurological outcomes.
METHODS
Study setting
This was an interrupted time-series study that used data from a nationwide prospective emergency medical service (EMS) out-of-hospital cardiac arrest (OHCA) registry in Korea. In total, 16 provincial headquarters of the fire department (FD) operate a fire-based EMS with approximately 1,500 ambulances and 8,500 emergency medical teams (EMTs; approximately 50% of level 1 and 50% of level 2). Moreover, 15 provinces have single and unified central dispatch centers, and only 1 province has agency-based dispatch centers. Medical directors oversee the CPR instructions of the dispatchers.
A strict nationwide quality assurance program on EMS for 4 major emergency conditions, including OHCA, severe trauma, acute myocardial infarction, and acute stroke, has been established in 2011 and has provided feedback to the provinces' FDs, EMS agencies, and individual EMTs.
There are around 460 emergency departments (EDs) in the country, which are designated as level 1, 2, or 3 based on their capacity that is identified by the Ministry of Health and Welfare. Board-certified emergency physicians in 20 level 1 and 130 level 2 EDs mandatorily provide 24/7 emergency care. The level 1 EDs must also have at least 20 emergency intensive care units. The general practitioners in level 3 EDs provide basic emergency care.
Study population
Patients with OHCA who received EMS from January 2009 to December 2014 were included in the study. However, those who did not receive resuscitative efforts, those who were witnessed by EMS providers, or those with missing information on treatment outcomes at discharge were excluded.
Nationwide implementation of telephone CPR (intervention)
In 2011, Seoul FD, one of the largest provinces in Korea, implemented a telephone CPR program, and an extremely significant improvement in treatment outcomes and an increase in the bystander CPR rate were observed. In October 2012, the National Emergency Management Agency expanded the program to all provincial FDs and developed a nationwide intervention by launching the telephone CPR program. In 2013, all dispatch centers set-up an electronic program for detecting an OHCA case in which instructions about CPR are provided to bystanders via telephone and the process is reported.
Thus, we defined 3-time periods, namely, before intervention, during intervention, and after intervention. Moreover, the specific periods were as follows: 1) before intervention: January 1, 2009 to December 31, 2010; 2) during intervention: January 1, 2011 to December 31, 2012; 3) after intervention: January 1, 2013 to December 31, 2014.
The program was developed based on the 2010 American Heart Association14 guidelines, which included; 1) 2 simplified key questions for identifying OHCA (altered mental status and abnormal breathing) and 2) standard communication processes for providing high-quality bystander CPR. The protocol was modified to accommodate the different characteristics of the 3 distinct patient groups: 1) general CPR protocol for OHCAs in adults with presumed cardiac etiology and general trauma; 2) CPR protocol for respiratory-induced OHCA, including asphyxia, hanging, chocking, and drowning; and 3) pediatric, infant, and neonate CPR protocols. Chest compression only CPR was used for the general OHCAs, whereas chest compression plus rescue ventilation method was used for respiratory OHCAs. For patients younger than 8 years, pediatric, infant, and neonate CPR protocols were used.
Education program for dispatchers was actively executed in the telephone CPR course that was developed by the Pan-Asian Resuscitation Outcomes Study8 network of the Asian EMS Council, Cardiac Arrest Registry to Enhance Survival investigators of the US, Save Hearts in Arizona Registry and Education investigators of Arizona, and Laerdal Medical in 2011. The education program included didactic sessions for telephone CPR, interactive skill sessions, and feedback sessions. More than 90% of dispatchers completed the course training in 2013. After the off-line courses, all dispatchers took a web-based, self-learning program translated in Korean and completed refresher training workshops annually.
Data collection
We used 3 data sources: EMS run sheets for basic ambulance operation information, EMS cardiac arrest registry, and dispatcher CPR registry. Data on outcomes were collected using data released by the Bureau of Statistics and reports published by the Korea Centers for Disease Control (KCDC). All EMS registries for each patient are linked as 1 episode using the ambulance dispatch number. The KCDC reviewed the medical records of all patients with OHCA who were transported by EMS to hospital EDs (approximately 700 hospitals) based on the abovementioned EMS registries.
Primary outcomes
The primary outcomes of this study were bystander CPR rate and good neurological outcomes. Good neurologic outcomes were categorized when the surviving patient had a cerebral performance category score of 1 or 2.
Statistical analysis
Categorical variables were presented as frequency and percentage, and continuous variables were presented as means with standard deviations. Comparison between groups was performed using χ2 test/Fisher's exact test for categorical variables and analysis of variance for continuous variables (age, response time, and prehospital time).
To compare the changes before and after the implementation of telephone CPR program, both risk ratio and risk difference were estimated and presented. Meanwhile, to describe the changes in the trend before and after the intervention, a segmented regression analysis was performed to estimate the intervention effects in the interrupted time-series studies, which allowed the calculation of the excess number of patients who additionally received bystander CPR and had good neurological outcomes.
RESULTS
The total number of EMS-assessed OHCA cases was 148,403. Among the 164,221 target patients, 8,190 (5.0%) patients with unavailable medical records (Fig. 1), 1 with unknown sex, and 7,627 with unknown outcomes (4.9%) were excluded. The demographic characteristics of the study participants are presented in Table 1. No differences in the distribution of patients according to sex were observed. The average age of the participants was 63.7 years, and this indicates that the configuration of the adult group before the intervention was higher than that after the intervention and that the highest configuration of the elderly group was after the intervention. Approximately 66.4% of cardiac arrest occurred in private with 37.3% of witnesses. In addition, the after group had a lower number of initial shockable rhythm than the before group, whereas the number of applied advanced airway management was higher in the during group, and the percentage of transfer to levels 1–2 EDs increased in the after group.
Fig. 1
Flow of patient enrollment.
EMS = emergency medical service, OHCA = out-of-hospital cardiac arrest.
Table 1
Demographic findings of study participants in the before, during and after intervention groups

Intervention: telephone CPR program implementation.
EMS = emergency medical service, ECG = electrocardiogram, VF/VT = ventricular fibrillation/ventricular tachycardia, PEA = pulseless electrical activity, SD = standard deviation, ED = emergency department, CPR = cardiopulmonary resuscitation, ROSC = return of spontaneous circulation.
The percentage of cardiac arrest outcomes increased from the before to after group: from 2.9% to 10.3% in bystander CPR; from 1.4% to 4.3%15 in pre-hospital return of spontaneous circulation (ROSC); from 3.5% to 5.0% in survival discharge; and from 1.0% to 2.6% in good neurological outcomes (Table 1).
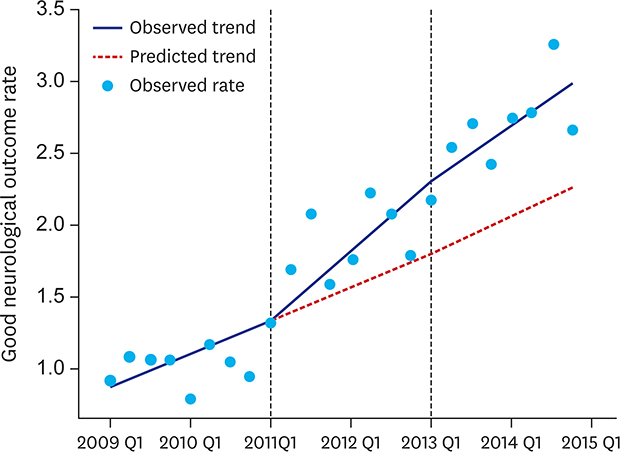
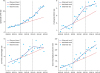
In the segmented regression analysis, the trend of bystander CPR rate had significant changes. A sharp change in the slope was found in the observed trend than the predicted trend during and after the telephone CPR, and a similar tendency was observed in the rate of good neurological outcomes. In addition, the sharp slope changes were also observed in the survival discharge rate during intervention. However, a decrease in the slope with an increase in the width was identified after the intervention (Fig. 2).
Fig. 2
Observed and predicted trends in the outcomes.
CPR = cardiopulmonary resuscitation, ROSC = return of spontaneous circulation.
The number of bystander CPR increased by 1.9 times (95% confidence interval [CI], 1.8–2.0) and 3.3 times (95% CI, 3.1–3.5) during and after the intervention compared with before the intervention, whereas the number of good neurological outcomes increased by 1.8 times (95% CI, 1.6–2.0) and 2.6 times (95% CI, 2.3–2.9) during and after the intervention, respectively. The rate of bystander CPR also increased by 2.5% (95% CI, 2.2–2.7) during the intervention and by 6.4% (95% CI, 6.2–6.8) before and after intervention, and this result indicates that the rate of good neurological outcomes increased by 0.8% (95% CI, 0.6–0.9) during the intervention and by 1.6% (95% CI, 1.4–1.7) after the intervention (Tables 2 and 3).
Table 2
The effect of telephone CPR program on bystander CPR

Table 3
The effect of telephone CPR program on good neurological outcome

The excess number is defined as the number of bystander CPR and good neurological outcomes, which was additionally performed or obtained during and after the intervention, and this was indicated by the differences in the observed and predicted trends. In total, 493 and 2,127 patients with OHCA during and after the intervention periods received additional bystander CPR, respectively, and 125 and 339 patients with OHCA during and after the intervention periods had good neurological outcomes, respectively (Tables 2 and 3).
DISCUSSION
This study evaluated the effects of a nationwide telephone CPR program in terms of an increase in the bystander CPR rate and improvement in the good neurological outcomes of patients with OHCA. The bystander CPR rate significantly increased from 2.9% before the intervention period to 5.6% and 10.3% during and after the intervention period, respectively. The number of good neurological outcomes also increased from 1.0% before the intervention period to 1.8% and 2.6% during and after the intervention period, respectively. Specifically, 2,620 patients with OHCA received bystander CPR, and 464 patients with OHCA had good neurological outcomes after the implementation of the telephone CPR program.
The researches from the systemic review suggested the effectiveness of telephone CPR in improving survival outcomes. However, the increase in bystander CPR itself was not always associated with an increase in survival outcomes.16 Thus, we decided to define the result of bystander CPR as good neurological outcomes.
The initial response and treatment are crucial factors in cardiac arrest because irreversible brain damage occurs within 3 minutes and death within 4–6 minutes. Moreover, patients who received delayed emergency treatment survive with insufficient neurological function to ensure self-sufficiency, which directly leads to clinical and economic burden. As such, several countries have been investing lots of efforts to increase the survival rate of patients and prevent the effects of OHCA by building the initial response system for participants with OHCA. Telephone CPR is initiated for bystanders to start CPR immediately before the arrival of the emergency response team, which leads to early resuscitation that increases the possibility of neurologic recovery. Based on the research outcome, data present the sharp increase in the rate of bystander CPR and good neurological outcomes after the intervention. A recent research by Ro et al.17 on the effect of providing telephone CPR to patients with OHCA has shown that the group that was provided telephone CPR had a better neurologic recovery and 1.5 times higher prehospital ROSC than the no bystander CPR group.
The percentage of cardiac arrest in the elderly population has increased from 48.6% in 2006 to 57.3% in 2014 according to the KCDC.6 Moreover, our data showed an increase from 51.5% in the before intervention group to 56.2% in the after intervention group. Several studies have shown that old age is associated with worse outcomes in several critical illnesses,181920 and the same result was observed in cardiac arrest.21222324 Therefore, the increase in the elderly population with cardiac arrest is among the factors that decrease the number of good neurological outcomes.
The early use of a defibrillator by bystanders is positively associated with an increased survival.2526 According to a statistics annual report of the national emergency medical center, public access defibrillation and its installation were mandated since 2007, which led to 21,015 (prevalence of 4.1 per 100,000 person) installations.27 However, the number is marginal compared with the 440,000 and 2,400,000 installations in Japan28 and the USA,29 respectively. The evaluation of the effectiveness of Automated External Defibrillator (AED) is challenging due to underutilization. That is, the attempt rate by bystanders is only 4.1%, and the rate of defibrillation use is 0.7%.
Advanced airway management, such as insertion of supraglottic airways or endotracheal intubation, has long been the standard for airway management in patients with OHCA, and recent studies have shown the challenges in the survival benefit of advanced airway management compared with conventional bag-valve-mask ventilation in clinical settings.303132333435 The prospective, nationwide, population-based study by Hasegawa et al.35 showed that any type of advanced airway management was associated with the decreased odds of good neurological outcome compared with conventional bag-valve-mask ventilation in adult patients with OHCA. Our study also showed that the rate of applied advanced airway management increased to 10.7%. However, there is no enough evidence showing the correlation between good neurological outcomes and advanced airway management.
The level of ED care is determined based on human resources, equipment, and availability of each specialty. All EDs are categorized into levels 1, 2, and 3. Level 1 EDs have the highest capability and capacity, and most level 1 EDs provide hypothermia therapy and 24/7 emergency percutaneous coronary intervention (PCI), of which the transfer rate increased from 9.1% (before the intervention) to 11.5% (during the intervention) and 11.2%.15 In addition, there was no significant change after the sharp increase in 2011 according to the quarterly data, as shown in Fig. 3.Several studies have reported the beneficial effects of post-resuscitation care, including therapeutic hypothermia, on the neurologic recovery of patients with OHCA.153637 In particular, OHCA with a shockable rhythm is a major indication of therapeutic hypothermia.1536 Therefore, the increase in shockable rhythm leads to the increase in therapeutic hypothermia. In addition, the fact that bystander CPR increases the shockable rhythm has been proven in several studies.383940 Thus, therapeutic hypothermia is a mediating variable, not a confounding variable, that needs adjustment.
Fig. 3
Transfer rate to level 1 ED among patients with EMS-assessed OHCA.
ED = emergency department, EMS = emergency medical service, OHCA = out-of-hospital cardiac arrest.

The present study had several limitations. First, this was an observational study and not a randomized controlled trial. There was a significant possibility that a confounding variable could have affected the study results. Second, this study was conducted in an EMS facility with an intermediate service level, which is different from that in North American or European models with advanced service levels. The generalization of the study findings should be cautiously performed. Third, this study could not show the results after adjusting for confounding factors owing to the characteristics of the data, although it suggests the differences in OHCA before and after the intervention. Finally, the use of retrospectively collected data caused important variables to be categorized as unknown or missing, which might have caused some misclassification bias. Moreover, patients with unknown outcomes were excluded, which could have resulted in selection bias.
With the nationwide implementation of standardized telephone CPR, the number of bystander CPR and good neurological outcomes increased. Moreover, continuous quality control and expansion of education program, including telephone CPR, will result in a higher survival rate and improvements in good neurological outcomes of patients with cardiac arrest.
 XML Download
XML Download