

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A transrectal ultrasound-guided prostate biopsy (TRUSPB) is the most widely used diagnostic method for prostate cancer. Recently, the use of TRUSPB has increased markedly during health checkups for prostate cancer. However, TRUSPB can lead to complications such as pain, hematuria, hemospermia, rectal bleeding, dysuria, acute urinary retention (AUR), urinary tract infection (UTI), acute prostatitis, bacteremia, and life-threatening sepsis.1 Infectious complications are usually uncommon, but they sometimes result in severe morbidity and even death. Therefore, antibiotic prophylaxis is routinely used to reduce these complications at the time of TRUSPB.23 Fluoroquinolones (FQs) are broadly prescribed as prophylaxis because of their ease of administration, safety profile, and high penetration into prostate tissues.456 Nevertheless, infectious complications have been increasing alarmingly in recent years.78 Concerns about the risks and medical costs of these complications after TRUSPB have also increased. Hence, many physicians have questioned the old prophylaxis regimens and are trying to establish new drug protocols. Many recent studies suggest that infectious complications after TRUSPB due to FQ-resistant organisms are increasing.789
The American Urological Association (AUA) and the European Association of Urology guidelines for antibacterial prophylaxis for TRUSPB recommend FQs as agents of first choice, and these associations also recommend other drugs as alternatives to ciprofloxacin.1011 Several reports have shown that combined FQ and aminoglycoside prophylaxis, such as amikacin, reduces infectious complications after TRUSPB.9101112
In this study, we investigated whether the addition of amikacin to ciprofloxacin-based antimicrobial prophylaxis reduces infectious complications after TRUSPB in the era of high FQ-resistant rectal flora.
METHODS
Data collection
This retrospective study was performed between January 2015 and February 2017 in Chonnam National University Hwasun Hospital, Korea. All patients who were undergoing TRUSPB were examined for rectal flora using a rectal swab within 2 weeks before biopsy. Patients whose rectal swab culture showed no growth were excluded from this study.
Rectal swabs (KOMED, Seongnam, Korea) were plated directly onto MacConkey agar (KOMED) with or without 1 μg/mL ciprofloxacin and incubated overnight at 37°C in ambient air. All isolates were characterized on the Vitek® 2, using the GN and AST-GN30 cards (bioMérieux, Durham, NC, USA) for identification and susceptibility testing, respectively. Rectal swab samples were obtained within two weeks prior to the administration of prophylactic antibiotics and TRUSPB.
A total of 503 patients were enrolled in this study, and were divided into 3 groups according to FQ resistance of their rectal flora and prophylactic antibiotics. The 248 patients in group 1 who had FQ-sensitive rectal flora were given intravenous doses of ciprofloxacin (500 mg, twice daily) on the day of biopsy, which was continued orally for 2 days after TRUSPB. The 97 patients in group 2 who had FQ-resistant rectal flora received ciprofloxacin in the same manner as group 1 did. The remained 158 patients in group 3 who had FQ-resistant rectal flora received a single intravenous dose of 1 g amikacin 1 hour before TRUSPB in addition to intravenous ciprofloxacin. All biopsies procedures were carried out using a LOGIQ E9 TRUS device (General Electric, Milwaukee, WI, USA). An ACECUT automatic biopsy gun (CIVCO Medical Solutions, Kalona, IA, USA) with an 18-gauge needle was used to obtain standard 8–12 core biopsies, using the same protocol.
All patients who underwent TRUSPB were administered an enema (COLCLEAN-S ENEMA® 133 mL; Dibasic sodium phosphate, Monobasic sodium phosphate) on the day of biopsy. Rectal cleansing with povidone-iodine (Povidone iodine 10% solution) was performed immediately before biopsy.
All patient characteristics were assessed, including age, serum prostate-specific antigen (PSA), prostate volume, diabetes, surgical history, prostatitis, UTI, antibiotic exposure (FQ or others) within 6 months, and previous prostate biopsy history (within one year or greater than one year prior) before TRUSPB. Periprocedural data were also obtained on all patients, such as the number of biopsy cores, prophylactic antibiotic type, duration of antibiotic use, local anesthesia, rectal enema use, povidone-iodine rectal cleansing, infectious complications after TRUSPB, and pathological results.
We investigated the infectious complications, history of acute urinary retention (AUR), and hematuria after TRUSPB. Infectious complications included hospital admission due to infection, fever, symptomatic UTI, acute prostatitis, bacteremia, sepsis, and systemic inflammatory response syndrome (SIRS). The assessment of infectious complications was limited to 30 days after TRUSPB to accurately include only those patients with biopsy-related events. If the patients were admitted because of infectious complications, blood and urine samples from these patients were collected and examined to confirm the pathogens and their antibiotic sensitivity.
Statistical methods
Statistical analyses were performed with SPSS software ver. 19.0 (SPSS Inc., Chicago, IL, USA). Continuous variables are reported as mean values and standard deviations, and categorical variables are reported as frequencies (%). Fisher's exact tests were conducted to assess associations between covariate distributions and FQ resistance, extended-spectrum β-lactamase (ESBL) positivity, and infectious complications. Multivariate logistic regression (stepwise backward procedure) was performed to determine factors influencing infectious complications. Statistical significance was set at P < 0.05 for all analyses.
RESULTS
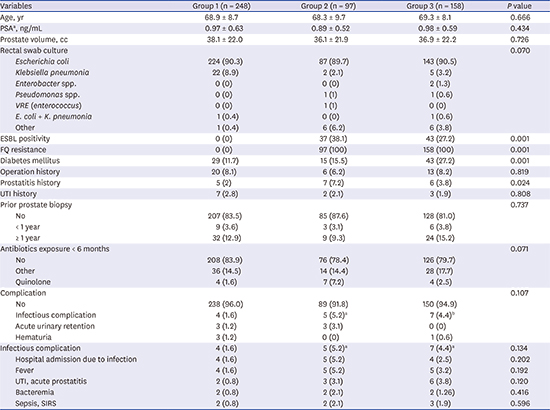
As shown in Table 1, there was no significant statistical difference in the patient characteristics, except history of prostatitis (P = 0.024) and diabetes (P = 0.001). We found that FQ resistance was 54.9% and ESBL positivity was 17.2% from reports of the rectal swab cultures, which were performed before TRUSPB. Overall complication rates including infectious complications, AUR and hematuria were not statistically significant (P = 0.107). In Group 1, four patients (1.6%) developed infectious complications. In Groups 2 and 3 with FQ-resistant rectal flora, the incidence of infectious complication increased 5.2% (5 patients) in group 2, and 4.4% (7 patients) in group 3. But the difference of infectious complications among the groups was not statistically significant (P = 0.1348).
Table 1
General characteristics of the patients

Data shown are mean ± standard deviation or number (%).
PSA = prostate specific antigen, VRE = vancomycin-resistance enterococci, ESBL = extended-spectrum beta-lactamase, FQ = fluoroquinolone, UTI = urinary tract infection, SIRS = systemic inflammatory response syndrome.
aLogarithmically adjusted; bgroup 2 vs. group 3, P = 0.7576.
A history of surgery within 6 months and ESBL positivity of rectal flora were strongly associated with infectious complications, as determined by using multivariate analysis (odds ratio [OR] = 3.68; P = 0.035 and OR = 4.02; P = 0.008, respectively). However, the other clinical parameters were not statistically different (Table 2).
Table 2
Associations between clinical parameters and infectious complications after prostate biopsy

The rectal flora obtained from rectal swab cultures before TRUSPB mostly included Escherichia coli, but Klebsiella pneumoniae, Enterobacter species, Pseudomonas species, and vancomycin-resistant enterococcus (VRE) were also found. Among the 16 patients who presented with infectious complications, 11 had positive culture reports (2 in group 1, 2 in group 2, and 7 in group 3). Table 3 shows details of the pathogens cultured from infected patients. The most common pathogens in patients with FQ-resistant rectal flora were FQ-resistant and ESBL-producing E. coli. All E. coli pathogens isolated from Group 3 were amikacin-susceptible species. Patients who had infectious complications were successfully treated with intravenous imipenem or piperacillin-tazobactam.
Table 3
Results of cultures performed for patients with infectious complications

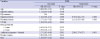
Multivariate analysis was performed to evaluate parameters that were associated with the FQ resistance of the rectal flora (Table 4). Table 4 shows that a history of diabetes was a risk factor for FQ resistance (OR = 2.19; P = 0.002). Another analysis was performed to assess the factors influencing the ESBL positivity of the rectal flora (Table 5). Age, diabetes, FQ resistance, surgical history, prostatitis history, UTI history, previous prostate biopsy history, antibiotic exposure history, prostate volume, and PSA were included in our model. As a result of this multivariate analysis, the antibiotic exposure within 6 months was found to be associated with ESBL positivity of the rectal flora (OR = 2.96; P = 0.005).
Table 4
Univariate and multivariate logistic regression analysis of factors influencing quinolone resistance of rectal flora
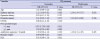
Table 5
Univariate and multivariate logistic regression analysis of factors influencing ESBL positivity of rectal flora
There was also a difference in diabetes and prostatitis history of the patients. However, in the multivariate analyses, we found no statistical difference in infectious complications and ESBL positivity associated with diabetes (Tables 2 and 4). In addition, a history of prostatitis was not an influencing parameter of infectious complications, FQ resistance, and ESBL positivity (Tables 2, 4, and 5).
DISCUSSION
If antibiotic resistance of rectal flora is low, additional aminoglycoside such as amikacin might reduce infectious complications after TRUSPB. However, there has been no trial comparing a combined regimen of amikacin and ciprofloxacin to ciprofloxacin alone as prophylaxis in TRUSPB in the era of high FQ-resistant rectal flora. In this study, we evaluated FQ resistance and ESBL positivity of rectal flora before biopsy in patients who were undergoing TRUSPB, and the results showed high antibiotic resistance of rectal flora (FQ resistance was 54.9% and ESBL positivity was 17.2%). We investigated whether the use of amikacin with ciprofloxacin lowered infectious complications after TRUSPB. However, no significant reduction of infectious complications was found after TRUSPB in patients with antibiotic-resistant rectal flora, despite the addition of amikacin.
Increasing health checkups for cancer and the introduction of the PSA screening test has led to a rise in the use of TRUSPB. As a result, the incidence of complications after TRUSPB has increased, and many physicians have attempted to reduce these complications, especially life-threatening sepsis. There has been no consensus on the most appropriate antibiotics and procedural details, such as bowel preparation and rectal swab at the time of TRUSPB, until now. However, antibiotic prophylaxis is routinely administered in almost all cases of TRUSPB, and ciprofloxacin was chosen as the most common antibiotic used for prophylaxis in TRUSPB because of its ease of use, pharmacological profile, and high bioavailability in the prostate.456 Kapoor et al.13 showed that using ciprofloxacin before transrectal prostate biopsy reduced infection rates significantly compared to those in the placebo group.
Unfortunately, FQ-resistant E. coli isolates are increasing annually in most countries worldwide,14 and many studies suggest that a single ciprofloxacin prophylaxis may not be sufficient to prevent infectious complications after TRUSPB.7815 Thus, several investigators have attempted to identify individual parameters that influence infectious complications after TRUSPB and improve protocols for antimicrobial prophylaxis to overcome the increased resistance to standard antibiotic regimens.1617 Many reports have shown that adding aminoglycosides reduced infectious complications after TRUSPB.912181920 In addition, some reports have suggested that the use of rectal swab culture to determine the rectal flora and its antibiotic-resistance pattern before TRUSPB may be beneficial. Targeted prophylaxis is an option to select an effective antibiotic for certain risky patients who are undergoing TRUSPB.2122
Many studies have shown the reduced incidence of infections after TRUSPB by adding amikacin to standard FQ prophylaxis, because amikacin reaches high concentrations in prostate tissue after one dose and E. coli are highly susceptible to it.91218 Another aminoglycoside, gentamicin, reduced infectious complications after TRUSPB in other studies.1920 As a result, some investigators have argued that the addition of aminoglycosides to standard FQ prophylaxis is cost-effective compared to that of FQ prophylaxis alone.1820
Recently, a single report revealed that another FQ, levofloxacin, showed good efficacy compared to that of ciprofloxacin.23 Unnikrishnan et al.23 reported a reduction in post-biopsy infectious complications in a severe case after changing the prophylactic antibiotics from ciprofloxacin to levofloxacin. Both FQs were used in combination with an aminoglycoside, and levofloxacin was chosen because it has a longer half-life and higher oral bioavailability than ciprofloxacin. They concluded that levofloxacin is superior to ciprofloxacin when used in combination with aminoglycosides in preventing severe infections after TRUSPB.
Marino et al.24 reported that single agents, such as ciprofloxacin, ceftriaxone, and gentamicin, alone are less effective than a combination regimen as prophylaxis for TRUSPB. In some studies, researchers argued that more intensive antibiotic regimens were needed to reduce the rate of complications.2526 However, if used unwisely, this may become a “double-edged sword.” Costelloe et al.27 reported that the pooled OR for antibiotic resistance was 2.5 within 2 months and 1.33 within 12 months of antibiotic treatment in UTI. They also showed that longer durations and multiple courses of prescribed antibiotics were associated with higher rates of bacterial resistance. Bacteria in a patient who is prescribed antibiotics can develop resistance to that antibiotic; this resistance is strongest in the month directly after treatment, but it can persist for up to 12 months. Costelloe et al.27 noted that this residual effect is likely to be an important enhancer for spreading resistance to first-line antibiotics and may lead to increased use of second-line antibiotics in the patient's community.
Hyle et al.28 reported that inappropriate initial treatment with antibiotics is an independent risk factor for mortality in patients with bacteremia caused by ESBL-producing bacteria. Therefore, it is reasonable for a physician to try to find a pathogen before TRUSPB and choose a suitable antibiotic. In the current study, we found a high incidence of isolated ESBL-positive E. coli in patients with a history of antibiotic treatment within 6 months, and this was statistically significant (P = 0.005).
In this study, we investigated whether the use of amikacin with ciprofloxacin lowers infectious complications after TRUSPB. However, no significant reduction in infectious complications was found after TRUSPB despite different groupings according to FQ resistance and addition of amikacin. Rectal disinfection with povidone-iodine was used as a potential adjunct to antibiotic prophylaxis in this study. The rationale for a povidone-iodine rectal cleansing is to reduce the rectal bacterial burden before biopsy and lessen the microbial inoculum introduced during the biopsy procedure. In the groups 2 and 3 with quinolone resistance, a povidone-iodine enema could reduce the infectious complication rate by reducing the microbial load. This could explain the absence of a statistical difference in infectious complications among the groups.
Furthermore, all E. coli pathogens isolated in group 3 were amikacin-susceptible species. This is inconsistent with the results of other studies that support an effect of amikacin in reducing infectious complications after TRUSPB.912 Batura et al.12 studied 871 patients who underwent TRUSPB, and they found a reduction in bacteremia after the addition of amikacin, but not all infections caused by ciprofloxacin-resistant organisms were prevented. Recently, a prospective study by Miyazaki et al.29 revealed that the addition of amikacin to levofloxacin prophylaxis showed no advantage compared with levofloxacin alone in febrile UTI after TRUSPB. They studied 447 patients and found two with febrile UTI in the levofloxacin group and one with febrile UTI in the amikacin co-treatment group. The pathogens isolated from the three patients were FQ-resistant E. coli in two cases and ESBL-positive E. coli in the remaining case, but all were susceptible to amikacin. According to this result, Miyazaki et al.29 suggested that combined amikacin has no benefit, but they also noted that a low occurrence of febrile infection lowered the statistical power of their study.
In a retrospective study of 1,339 patients who underwent TRUSPB, Özden et al.30 compared ESBL-producing and non-producing E. coli isolated from patients who had infectious complications after TRUSPB. They reported that ESBL-positive E. coli had a significant reduction in activity for most antibiotics, including FQ, amikacin, and cephalosporin (P = 0.028). Extended antibiotic prophylaxis might be useful if the antibiotic resistance of the rectal flora is low. However, according to our results, extended antibiotic prophylaxis has limitations in patients with antibiotic-resistant rectal flora, especially ESBL-positive bacteria. Therefore, extended antibiotic prophylaxis might not be useful if the antibiotic resistance of the rectal flora is high, as observed in this study.
Our study showed that diabetes and antibiotic exposure history within 6 months were risk factors of FQ resistance (OR = 2.19; P = 0.002) and ESBL positivity of rectal flora (OR = 2.96; P = 0.005). These results are similar to those of Loeb et al.,16 who showed that diabetes is significantly associated with increased risk of post-prostate biopsy infections.
More infectious complications were found in patients with FQ-resistant rectal flora and most pathogens that caused infectious complications after TRUSPB were FQ-resistant and ESBL-positive E. coli strains (OR = 4.02; P = 0.008). A history of surgery within 6 months also showed significant association with infectious complications after TRUSPB (OR = 3.68; P = 0.035). This can be easily understood because broad spectrum antibiotics were used often during intensive surgery. These results regarding patient characteristics are not consistent with those of other studies,1624 and some considerations should be pondered to determine whether or not this risk factor is important prior to TRUSPB. Because western and European countries usually follow guidelines recommending single-dose prophylactic antibiotics in most surgeries, recent surgical history may not be a risk factor in these countries.
Unfortunately, in this study, no reduction in infectious complications was shown after addition of amikacin in patients with risk factors. Therefore, during TRUSPB planning, sufficient explanation about possible infectious complications after biopsy should be provided to patients with risk factors. If the patient cannot accept these potential complications, the physician can exclude them from transrectal prostate biopsy or restrictively use broad-spectrum antibiotics or targeted antibiotic prophylaxis based on rectal swab cultures.
All E. coli pathogens isolated from patients in Group 3 were amikacin-susceptible strains, but additional amikacin use did not reduce the incidence of infectious complications. Therefore, further research is needed regarding amikacin, including the most effective prescribed course, dosage, absorption in the body, prostate penetration, and bioactivity in the prostate.
Increasing incidents of FQ-resistant and ESBL-positive coliforms are found in the world today.78914 Gradually, more infections after TRUSPB are happening and more money is spent for treatment of infectious complications. Therefore, further extensive studies are necessary to reduce infectious complications after prostate biopsy, including those that examine choosing prophylactic antibiotics, customizing procedures for the patient, and managing potential infection during biopsy.
The current study has several limitations. We used MacConkey agar with 1 μg/mL ciprofloxacin. The rates of quinolone resistance in institutions that use MacConkey agar with 1 μg/mL ciprofloxacin could be higher than those in other institutions that use agar with 10 μg/mL ciprofloxacin. The variation in FQ resistance among studies may reflect regional and temporal differences in antibacterial susceptibility. However, methodological differences between studies are also relevant. We designed this study without other types of quinolones for antibiotic prophylaxis because of regulatory restrictions by the National Health Insurance Corporation. In practice, ciprofloxacin is commonly used for antibiotic prophylaxis in Korea; therefore, further study with levofloxacin is recommended. The small cohort, retrospective nature of this study were also limitations.
In conclusion, addition of amikacin to ciprofloxacin prophylaxis showed no advantage in patients with FQ-resistant rectal flora. Therefore, further trials of extended protocols will be required in the era of high FQ-resistant rectal flora.
 XML Download
XML Download