

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is an epidemic globally and a major risk factor of chronic diseases, including type 2 diabetes, hypertension, cardiovascular diseases, and stroke (1). The major cause for obesity is an increased intake and decreased consumption of energy. However, the bridge between energy intake and obesity is not fully understood (1). The mechanism between obesity and increase of cardiovascular disease is not fully explored, either. Recently, experimental and clinical studies about the role of bacterial lipopolysaccharides (LPS, endotoxin) have been noted (2). Energy intake is associated with endotoxemia in animals and human (1). The alteration of endotoxin can be involved in changes in energy extraction from the diet and modulation of endocrine functions, lipid metabolism, and the immune system. It can contribute to obesity or metabolic syndrome (34). Metabolic endotoxemia (ME, increased endotoxin in blood) also triggers toll-like receptor 4-mediated inflammatory adipokines and leads to a chronic low grade inflammatory status, which affects cardiovascular risk increase and target organ damage (1567). Exercise is a safe and effective treatment to prevent obesity and to improve prognosis for obesity or cardiovascular diseases (8910). Although some evidence shows that exercise may modify gut microbiota such as endotoxin (1011121314), the relationship between exercise and endotoxin has received less attention. In this study, we examined the circulating endotoxin according to energy intake and investigated impacts of controlled exercise on it in Korean women with obesity.
MATERIALS AND METHODS
Subjects
We recruited women who met obesity criteria of body mass index (BMI) 25 kg/m2 or greater between the age of 19 and 60 years. Participants were enrolled regardless of presence or diagnosis of any metabolic or cardiovascular disorders such as hypertension, diabetes, or thyroid disease. However, they were excluded if they reported at baseline any of the following situations: 1) if they have taken ergogenic levels of nutritional supplements that may affect muscle mass, hormone levels, or weight loss within 2 months; 2) if changes among medications affecting the evaluation variables of the study are expected (taking any weight loss medications, starting a new hyperlipidemia treatment, disconnecting the drug that was taken, or changing the drugs); 3) if they have antibiotic treatment within the previous 1 month or suffering from any acute cardiovascular, gastrointestinal (GI) or immunological diseases; and 4) if they already exercised regularly prior to the start of the study.
Exercise program
All participants took part in a supervised exercise program, well-known as Curves program, over 3 days per week throughout the protocol. Each workout consisted of 12 pneumatic or hydraulic resistant exercises in a concentric circle. Participants were instructed to complete as many repetitions as they could in 30 seconds for each piece of equipment. In an interval fashion, they performed floor-based aerobic exercises for 30 seconds after each resistance exercise in an effort to maintain an exercise heart rate that corresponded to 60% to 80% of their maximum heart rate. Heart rate was measured via palpation of the radial artery or carotid artery during exercise. Participants were required to complete 2 circuits and stretch every part of the body, which took approximately 30 minutes. All workouts were supervised by trained fitness instructors, who provided information about proper use of all equipment and assisted in maintaining of exact exercise technique. Attendance was recorded about each workout to monitor compliance to the exercise program.
Anthropometrics
The weights and body fat percentage of the subjects were measured with light clothing using an Inbody 330 (Biospace, Seoul, Korea), which is a multifrequency bioimpedence analysis device. BMI was calculated using the formula:
Waist circumferences and Hip circumferences were measured to the closest 0.1 cm in upright posture at the midpoint between the lower margin of the last palpable rib and the top of the iliac crest, and around the widest portion of the buttocks according to the World Health Organization (WHO)'s data gathering protocol. The average value of more than 2 measurements was used for all items recorded at baseline and after 12 weeks of exercise.
Biochemical analysis
After 8 hours of fasting, blood samples were taken at baseline and after 12 weeks of exercise. Also, blood samples at 2 hours and 4 hours after a high calorie meal intake (beef hamburger, coke, and French fries, 1,036 kcal; 15.8 g saturated fat, 43 g carbohydrate, 30 g protein) were taken. In all blood samples, serum was separated by centrifugation at 3,000 rpm for 10 minutes at room temperature and these were the re-centrifuged at 5,000 rpm for 5 minutes to obtain cell-free serum, which were stored at −80°C until analysis for lipid profiles, glucose, circulating endotoxin, and so on.
Analysis of circulating endotoxin
Circulating endotoxin level was analyzed using a commercially available QCL-1000TM Limulus Amebocyte Lysate (LAL) Endpoint assay (Lonza, Walkersville, MD, USA). Optical densities were measured using a micro plate reader at 405 nm (Molecular device, San Francisco, CA, USA).
Statistical analysis
Statistical analysis was performed using standard software (SPSS version 20.0; IBM Corp., Armonk, NY, USA). Variables were expressed as mean ± standard error of the mean (SEM) or median (interquartile range [IQR]), depending on assessment for Gaussian distribution. Data were analyzed by para-metric or non-parametric test where appropriate. A P value less than 0.05 was considered as statistically significant.
RESULTS
Participants' characteristics and changes of lipids over postprandial time at baseline
A total of 20 women (age 37.1 ± 9.7 years old, BMI 27.9 ± 0.5 kg/m2) were enrolled in this study. Their baseline anthropometric characteristics and postprandial changes of lipid profiles show in Tables 1 and 2. Ingestion of a high calorie meal led to a significant rise in glucose after 2 hours (postprandial 2 hours [PP2]) (85.9 ± 9.1 mg/dL at fasting vs. 117.7 ± 6.4 mg/dL at PP2, P < 0.01) and in triglyceride (TG) over postprandial 4 hours (PP4) (141.4 ± 31.9 mg/dL at fasting vs. 201.4 ± 30.1 mg/dL at PP2 and 250.0 ± 41.9 mg/dL at PP4, P < 0.01) (Table 2, Fig. 1A and 1D). Total cholesterol (TC) remained relevantly unaltered over 4 hour's period. Low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) changed and showed significantly at PP4 (reduced, P < 0.05 for LDL-C, P < 0.01 for HDL-C).
Table 1
Participant characteristics
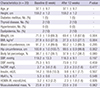
Data are expressed as mean ± SEM or median ± SEM (IQR), depending on assessment for Gaussian distribution.
BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, hsCRP = high-sensitive C-reactive protein, HbA1c = hemoglobin A1c, HOMA-IR = homeostasis model assessment of insulin resistance, SEM = standard error of the mean, IQR = interquartile range.
Table 2
The postprandial changes in glucose and lipid profiles before and after exercise

Data are expressed as mean ± SEM or median ± SEM (IQR), depending on assessment for Gaussian distribution.
TC = total cholesterol, TG = triglyceride, HDL-C = high-density lipoprotein-cholesterol, LDL-C = low-density lipoprotein-cholesterol, SEM = standard error of the mean, IQR = interquartile range, PP0 = postprandial 0 hour.
*P < 0.01; †P < 0.05 vs. at PP0 of same week.

The level of circulating endotoxin at baseline
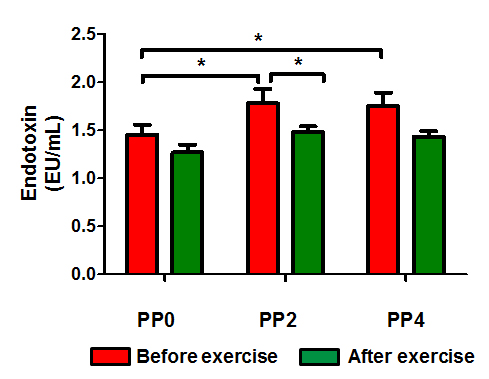
The fasting circulating endotoxin level was 1.45 ± 0.11 EU/mL at baseline. Postprandial exposure to a high calorie meal led to a significant rise in circulating endotoxin levels and the peak level of circulating endotoxin showed after 2 hours (1.45 ± 0.11 EU/mL at fasting vs. 1.78 ± 0.15 EU/mL at PP2 and 1.75 ± 0.14 EU/mL at PP4, P < 0.05, Table 2 and Fig. 1B). These changes of endotoxin related to a meal were similar pattern to those of glucose.
The effect of 12 weeks exercise on anthropometric data
Table 1 shows the results comparing the average body composition measured before and after 12 weeks of exercise. All mean values of the weight, BMI, body fat percentage, and waist and hip circumference showed a tendency to decrease at post-exercise compared to pre-exercise. The weight, BMI, and hip circumference were significantly reduced at post-exercise compared to pre-exercise (P < 0.01). However, the changes in waist circumference and body fat percentage were not statistically significant.
The effects of 12 weeks exercise on endotoxemia and lipid profiles
After 12 weeks of exercise, the fasting level of circulating endotoxin was 1.27 ± 0.08 EU/mL, that decreased compared to before exercise but was not statistically different. The postprandial change of circulating endotoxin by ingestion of a high calorie meal showed a similar tendency at pre- and post-exercise. The level of circulating endotoxin was increased after 2 hours and then, reduced. The peak level of circulating endotoxin, measured at PP2, was significantly different between pre-exercise and post-exercise. After 12 weeks exercise, the peak circulating endotoxin significantly decreased (1.78 ± 0.15 EU/mL at baseline vs. 1.48 ± 0.06 EU/mL after 12 weeks, P < 0.05, Table 2 and Fig. 1B). The glucose also showed a similar tendency at PP2 after 12 weeks exercise (117.7 ± 6.4 mg/dL at baseline vs. 100.7 ± 5.1 mg/dL after 12 weeks, P < 0.05, Table 2 and Fig. 1A).
DISCUSSION
The human gut microbiota is known as a “microbial organ,” because it is involved in various homeostatic processes in humans. Recently, gut microbiota was demonstrated as having a close relationship with obesity (1). Turnbaugh et al. (2) reported that the gut microbiota is different between obese and lean mice. When they transferred the gut microbiota from obese and lean mice to germ-free mice, germ-free mice that received microbiota from obese mice, compared with those that received the gut microbiota from lean mice had higher energy extraction from food and showed greater weight gain. It was also reported that people with obesity have a less diverse gut microbiota than those with normal body weight (24). These findings suggest that gut microbiota is probably not a mere consequence of obesity and may have a prominent role in overweight and obesity pathogenesis. It was supported that gut microbiota is associated with obesity-related disorders such as overall adiposity, insulin resistance, and dyslipidemia (35615). Especially, gram-negative bacteria-derived compounds, endotoxin produces activation of Toll-like receptor-4 signal, contribute low-grade inflammatory states and play a pivotal role in pathogenesis of metabolic diseases. ME that is elevated after high fat or energy intake is remarkable in people with obesity-related, cardiovascular disorders including non-alcoholic fatty liver disease, diabetes mellitus, hypertension, and dyslipidemia (5671516). In a large prospective cohort study, it is reported that endotoxemia is associated with increased risk for clinically incident diabetes and is independent of other established diabetes risk factors including glucose, lipid, and C-reactive protein, as well as BMI (616).
Exercise is a good non-pharmacological treatment to control and improve prognosis for obesity and cardiovascular diseases (8910). In some studies, exercise has been shown to modulate gut microbiota (10111214). Petriz et al. (10) demonstrated that non-obese and hypertensive rats harbor a different gut microbiota from obese rats and that exercise training alters gut microbiota from an obese and hypertensive genotype background. Clarke et al. (11) reported that athletes had a higher diversity of gut micro-organisms compared with controls. The results provide evidences for a beneficial impact of exercise on gut microbiota diversity. Although the relationship between obesity related disorders and gut microbiota, especially endotoxin, is becoming more evident, the impacts of exercise on the gut microbiota have not been fully unknown. The effects of exercise on gut microbiota need to be further investigated through the controlled parameters such as exercise volume and intensity. The Curves for women program is followed at over 10,000 fitness franchises across the globe with millions of women worldwide following the program. It is not only a resistance-based exercise program for muscle, but it is also a typical aerobic exercise that is relatively stable and safe (17). All participants in this study performed a supervised, controlled exercise program of Curves. As a result of the study, exercise treatment was so effective that body weight and hip circumferences of participants were reduced. The circulating endotoxin level at fasting state was also decreased after an exercise treatment. The postprandial circulating endotoxin level was increased after a high energy meal, like that, endotoxemia is associated with high energy or fat intake in previous studies. However, postprandial endotoxemia was suppressed over 4 hours in post-exercise and showed no significant differences compared with a fasting level. Postprandial circulating endotoxin levels in post-exercise were lowered significantly from those in pre-exercise. The suppression of endotoxemia before and after a diet is thought that it can inhibit a low grade inflammatory status and prevent progressions to greater body weight or cardiovascular disorders. Consequently, this is thought to explain underling mechanisms between exercise treatment and better clinical outcomes.
Our study has several limitations with small sample size. Although we used a pretty controlled exercise, Curves, in our study, other physical activities were not controlled in all participants. Even though we excluded conditions such as antibiotics treatment, we could not completely eliminate other possible conditions that can cause changes for endotoxin. The possibility of subclinical disorders that could be responsible for alterations of circulating endotoxin should be considered. We investigated circulating endotoxin at fasting and postprandial state, both. However, diet control was not performed in the study. Diet for several days that participants ate before taking blood samples can exert an influence on circulating endotoxin levels.
In conclusion, this is the first study, to the best of our knowledge, to show circulating endotoxin levels in Korea and we confirm that high energy intake is associated with endotoxemia. Also, we investigate that the rise of circulating endotoxin can be suppressed despite the same high energy intake after exercise treatment prospectively. These data present the knowledge regarding the effect of exercise on gut microbiota, especially endotoxin. Of course, further studies need to establish the impact and clinical outcomes of these modulations on host homeostasis.
 XML Download
XML Download