

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There is growing interest in outcomes of schizophrenia and other psychoses as psychoses have been associated with premature mortality and reductions in life expectancy (1). Several previous studies have explored the elevated mortality risks commonly found in mental disorder patients and have conveyed that individuals diagnosed with substance use disorder, schizophrenia, and bipolar disorder show higher risks for all-cause mortality (2). In fact, life expectancies of schizophrenia patients have been known to be 10 to 25 years shorter than that of the general population (3). Similarly, bipolar disorder has been associated with decreased life expectancy by around nine to 14 years and behavioral disorder resulting from alcohol and substance use has been related with an increased risk of death (45). Unsurprisingly, individuals with mental disorders also report higher standardized mortality ratios (SMRs) compared to the general population (6).
Natural and unnatural causes have been known to attribute to higher mortality commonly found in psychoses patients. Specifically, suicide mortality has been identified as the primary unnatural cause, with it being the most common cause of death among individuals with schizophrenia (1). Substantially increased suicide rates were also found in patients with depression, bipolar disorder, opioid use, and alcohol use disorder (6). Identifying excess all-cause and suicide mortality associated with mental disorders is particularly significant in Korea because major mental disorders are prevalent (schizophrenia and schizoaffective disorder 0.3%, major depressive disorder 5.6%, and nicotine and alcohol use disorder 16.4%) and its suicide rate is the highest among the Organization for Economic Cooperation and Development (OECD) countries (78).
Previous research investigating elevated mortality rates in patients with schizophrenia and other psychoses have mainly focused on Western European and North American countries (9). Additionally, few previous studies have examined mortality using a large, nationally representative sample (10). With regard to studies conducted on East Asia, a study by Saku et al. (11) revealed that Japanese bipolar patients exhibit significantly higher SMRs than the general population using longitudinal data from 1948 to 1982. As for studies in Korea, an investigation by Park et al. (12) reported higher mortality risks in psychiatric patients based on data from a general hospital. Hence, despite the substantial economic burden of psychoses in Korea, few Korean studies have investigated excess mortality associated with psychotic disease using a large, nationally representative sample of individuals with follow up data. Therefore, the aim of this study was to examine all-cause and suicide mortality in a nationally representative cohort of individuals with schizophrenia, mood disorder, and mental and behavioral disorders due to psychoactive substance use and to compare mortality in this cohort with that of the general population.
MATERIALS AND METHODS
Study population
This study used data from the Korea National Health Insurance (NHI) Service National Sample Cohort, 2002 to 2013. The NHI data consisted of 1,025,340 nationally representative random samples of the Korean population in 2002, which accounted for around 2.2% of the entire population. Data were collected by the Korean NHI Service (KNHIS) using a systematic sampling method to generate a representative sample of the 46,605,433 Korean residents recorded in 2002. Follow up data were available up to 2013 and included information on medical claims filed between 2002 and 2013.
In this study, all study participants with a diagnosis record of schizophrenia and schizoaffective disorders (International Classification of Diseases version 10 [ICD-10] F20, F25), mood disorders (F30–39), and mental and behavioral disorders due to psychoactive substance use (F10–19) were screened for inclusion at baseline. Individuals with at least 2 outpatient claims or one inpatient claim for the defined ICD-10 codes in primary, secondary, or tertiary hospitals were included. To ensure identification of individuals with a first diagnosis of the stated diseases, individuals diagnosed before 2005 were excluded from the analysis. Individuals aged below 15 years were also excluded, which led to the final inclusion of 9,387 schizophrenia and schizoaffective disorder cases, 86,922 mood disorder cases, and 10,881 mental and behavioral disorders due to psychoactive substance use cases. Categorization of subjects with multiple disorders was made according to the primary ICD-10 diagnosis recorded.
Case-tracing procedure
The study population was followed up for 9 years to identify all-cause and suicide deaths. Occurrences of death were recorded in the cohort based on the National Statistical Office (NSO) database. In Korea, all deaths are compulsory reported to the NSO through a death notice. Suicide deaths were separately recognized using the ICD-10 code X60–84.
Variables
Information on the age, sex, income, region, and Charlson Comorbidity Index (CCI) of the study participants were collected. Age was categorized into 15–24, 25–34, 35–44, 45–54, 55–64, 65–75, and 75 or above. Sex was classified into men or women, income into medical aid, low, middle, or high, region into Seoul/metropolitan cities or others, and CCI from 0 to 7. Schizophrenia was partitioned into schizophrenia and schizoaffective disorder. Income was categorized into medical aid, low, middle, and high based on the NHI contribution premium level of patients, which can be seen as a surrogate indicator of income. For workplace insured NHI, insurance contribution premiums are calculated depending on the average annual salary level of individuals. For regionally insured NHI, contributions premiums are calculated using taxable income and assets that can reflect individuals' living standards. Hence, contribution premiums can be seen as a proxy for the ability to pay. With regard to region, Seoul and the seven metropolitan cities of Korea were grouped into the same category and all other provinces into another category. CCI was adjusted to account for the potential effect of comorbidities. The CCI was calculated yearly using the Quan's method, in which 19 diseases were categorized into scores of 1, 2, 3, or 6 and the CCI per subject obtained by the sum of all scores (13).
Statistical analysis
Crude mortality rates were calculated for all-cause and suicide mortality per 100,000 person years (PY) stratified by baseline socio-demographic and health related characteristics. Date of first applicable record of schizophrenia, mood disorder, and mental and behavioral disorder due to psychoactive substance use was utilized as the entry point and date of death or end of follow up period as the end-point. Poisson regression modelling was conducted to quantify the effect of baseline socio-demographic and health related characteristics on risks of all-cause and suicide mortality while adjusting for confounders. SMRs with 95% confidence intervals (CIs) were calculated for all-cause and suicide mortality. SMRs refer to the ratio of the observed number of deaths in each psychiatric group to the expected number of deaths in the same cohort based on the general Korean population. All calculated P values were 2-sided and considered significant at < 0.05. Analysis was performed using the SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
All-cause and suicide mortality rates by socio-demographic and health related characteristics for all-cause and suicide death are presented in Tables 1, 2, 3. All-cause mortality was the highest among mental and behavioral disorder due to psychoactive substance use patients (1,051.0 per 100,000 PY), followed by schizophrenia (949.1 per 100,000 PY), and mood disorder patients (559.5 per 100,000 PY). Mortality rates generally increased with age and were higher among men than in women. Participants scoring lower on the CCI showed lower mortality rates.
Table 1
Mortality rates (per 100,000 PY) by baseline characteristics in schizophrenia patients
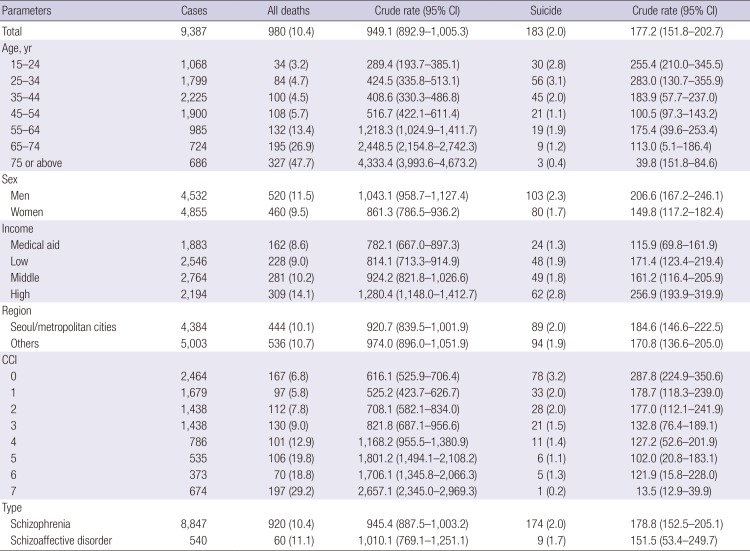
Table 2
Mortality rates (per 100,000 PY) by baseline characteristics in mood disorder patients
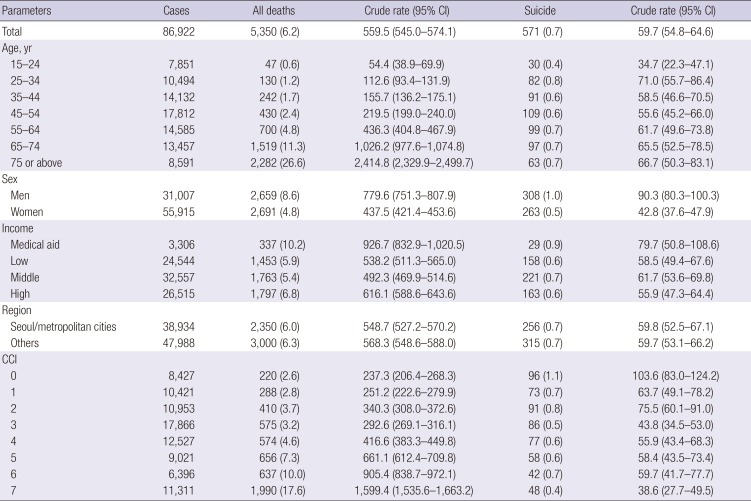
Table 3
Mortality rates (per 100,000 PY) by baseline characteristics in mental and behavioral disorder due to psychoactive substance use patients
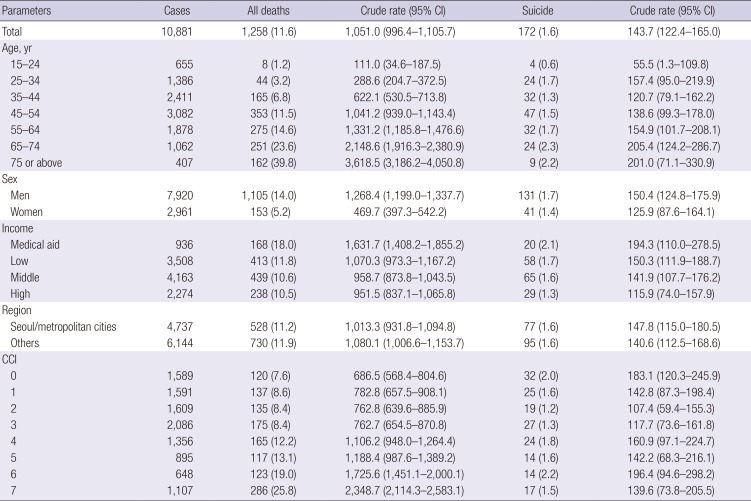
Highest suicide mortality was found in schizophrenia (177.2 per 100,000 PY), mental and behavioral disorder due to psychoactive substance use (143.7 per 100,000 PY), and mood disorder patients (59.7 per 100,000 PY). In schizophrenia patients, younger cases had higher suicide death rates. Such trends were reversed in patients diagnosed with other psychoses. Overall, suicide mortality rates were higher in men than in women.
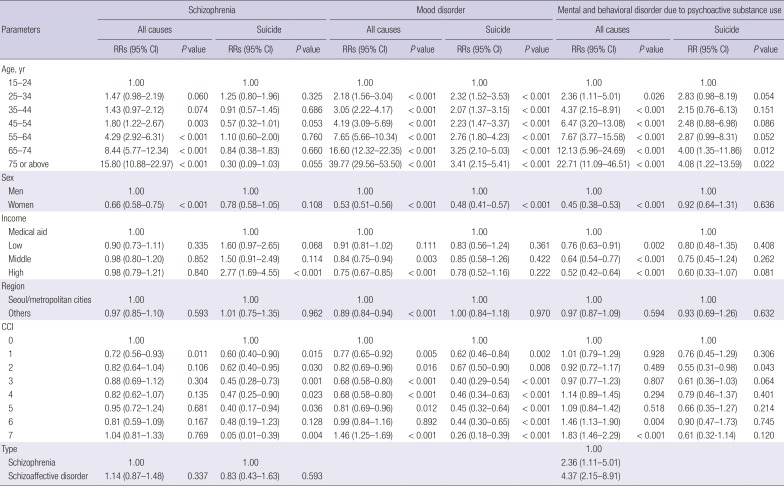
Table 4 shows the results of the Poisson regression modelling. The rate ratios (RRs) for all-cause mortality were significantly lower for younger and women populations. Apart from schizophrenia patients, suicide mortality rates were also reduced in younger aged individuals. Women generally had lower suicide death rates and higher scores on the CCI were associated with decreased suicide mortality rates.
Table 4
RRs for all-cause and suicide mortality by baseline sociodemographic characteristics
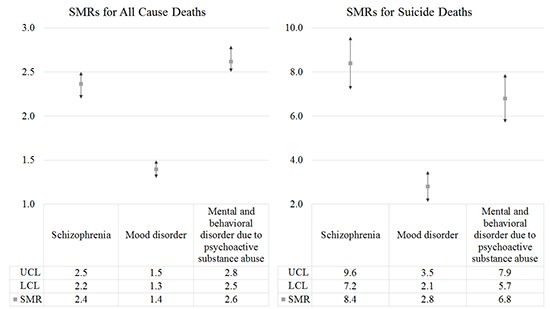
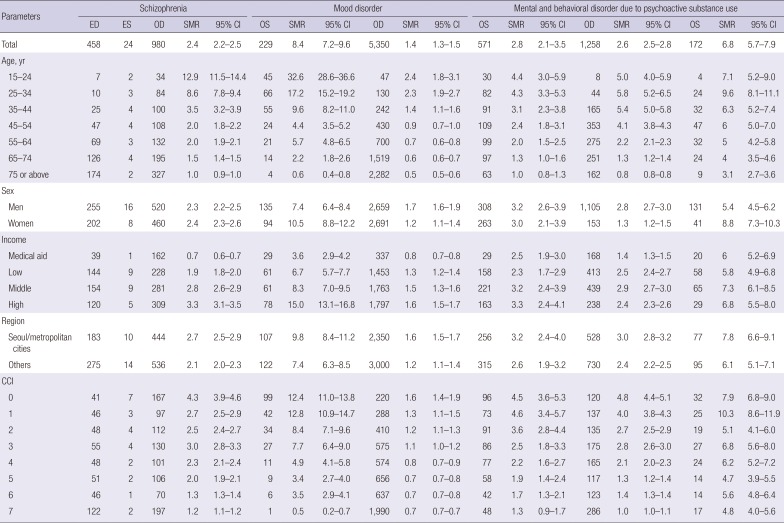
The SMRs for all-cause and suicide deaths are presented on Table 5. Schizophrenia, mood disorder, and mental and behavioral disorder due to psychoactive substance use patients showed increases in all-cause mortality compared to that of the general cohort (schizophrenia, SMR 2.4; 95% CI 2.2–2.5; mood disorder, SMR 1.4; 95% CI 1.3–1.5; mental and behavioral disorder due to psychoactive substance use, SMR 2.6; 95% CI 2.5–2.8). SMRs were more pronounced for cases in lower age groups. Patients also exhibited higher SMRs for suicide deaths (schizophrenia, SMR 8.4; 95% CI 7.2–9.6; mood disorder, SMR 2.8; 95% CI 2.1–3.5; mental and behavioral disorder due to psychoactive substance use, SMR 6.8; 95% CI 5.7–7.9). Likewise, younger participants had escalated SMRs, in particular schizophrenia patients.
Table 5
SMRs for all causes and suicide deaths
DISCUSSION
The results of this study reveal that adults diagnosed with schizophrenia, mood disorder, or mental and behavioral disorder due to psychoactive substance use die at approximately 2.4, 1.4, and 2.6 times the rate of the general population. The results are in line with previous studies in which psychoses were associated with higher mortality risks. A previous study reported significantly higher all-cause mortality for severe mental disorders in French participants (14). In schizophrenia patients, the SMR for all-cause mortality was analyzed to be 2.98 based on a meta-analysis of 38 studies (15). Elevated SMR was also found among late onset schizophrenia patients aged 60 or above, inferring that schizophrenia also increases mortality in old age (16). With regard to mood disorders, all-cause mortality increased 2-fold among Swedish patients with bipolar disorder in prior research (17). Alcohol, drug use, and antisocial personality disorders were also related with a higher risk of death in a study focussing on American participants (5).
Increased mortality risk was also found for suicide deaths, with the SMRs rating 8.4 for schizophrenia, 2.8 for mood disorder, and 6.8 for mental and behavioral disorder due to psychoactive substance use. The study findings are consistent with prior evidence as suicide mortality has been repetitively reported to be high for psychoses patients (1819). The tendencies toward higher SMRs were particularly pronounced in younger aged groups, particularly for schizophrenia. This may have resulted due to the low expected death rates of younger Korean populations (12) and the fact that schizophrenia patients often exhibit a reduced age of death. In fact, a previous Danish study revealed that schizophrenia patients experience shortened life expectancies, with it being 18.7 years for men and 16.3 years for women (20). Similarly, decreases in life expectancy have also been reported in other United States, Swedish, and Finnish studies and this mortality gap has increased in recent years (20). Apart from age, males had higher suicide mortality risks than females, which is also consistent with prior research (21).
The large health risks observed in individuals diagnosed with schizophrenia, mood disorder, and mental and behavioral disorder due to psychoactive substance use highlight the need for effective medical care provision to psychoses patients. Studies have documented that patients with severe mental disorders are less likely to use general medical services and that these individuals often receive lower quality medical care (1722). Several explanations have been proposed to elucidate the reasons for disparities in quality of care often received between psychoses and non-psychoses patients. First, patients with mental disorders are frequently unable to effectively communicate with health care providers due to cognitive disturbance or affective instability (23). Furthermore, non-psychiatrist physicians may be biased against psychoses patients, leading to poorer medical management and quality of care (24). Non-psychiatrist providers may also lack experience in treating mental illnesses, which requires the need for adequate cooperation between non-psychiatrists and psychiatrists (25). Psychoses patients with poor socioeconomic status may also have poor access to health services and may face difficulties in receiving adequate medical care (22). Therefore, considering the tendencies of East Asian individuals to express psychiatric problems less frequently, efforts should be made on addressing the risk factors for mortality and to monitor vulnerable groups of individuals in the aim of reducing the mortality gap of psychoses (26).
This study has some limitations. First, the data used in this study classified medical illnesses based on ICD-10 codes. The ICD-10 codes were used to identify and analyze patients diagnosed with schizophrenia, mood disorder, and mental and behavioural disorder due to psychoactive substance use. Other standard classification systems, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) could not be utilized. Hence, there may have been inaccuracies in diagnoses as recordings were made by different individuals. Second, information was not available on several key risk factors, including education level, smoking status, and alcohol consumption status. Third, because the date of death was only given up to the year and month in the NHI data, there may have been some inaccuracies in estimating date of death. Despite the limitations described above, this study offers insights, as it is the first to investigate excess mortality in Korean psychiatric patients using a large nationally representative sample.
In conclusion, the results of this study confirm that individuals diagnosed with schizophrenia, mood disorder, and mental and behavioral disorder due to psychoactive substance use show excess mortality in Korea. Higher risks of mortality were found for suicide deaths, particularly among younger aged populations. Taking into account the number of psychoses patients and the fact that Korea ranks first among OECD countries in suicide, efforts should be made on targeting and addressing vulnerable groups of individuals to reduce the mortality gap of mental illnesses in the coming decades.
 XML Download
XML Download