

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) is a major global health problem as a leading cause of death worldwide. In 2014, an estimated 9.6 million people developed TB and 1.5 million died from the disease (1). TB is also one of the serious threats to public health in Republic of Korea, with an estimated incidence in 2014 was 86 per 100,000 population (1), which corresponds to an intermediate national burden of TB.
Due to the destructive nature of TB, pulmonary TB may induce chronic lung impairment (2). Despite effective TB therapy, the healing process following resolution of active TB can lead to structural damage to the lung parenchyma and airways (3). Recent systematic reviews (45) and general population based Burden of Obstructive Lung Disease (BOLD) study (6) have found that past TB was associated with an increased risk of airflow obstruction (AFO) (456) as well as an increased risk of spirometric restriction (6).
Population-based studies defined a prior infection with TB mainly through self-reported history (78) and only a small number of studies based on TB lesion on chest X-ray (CXR) (910). Using a definition of either a history or TB lesion on CXR, TB survivors who were cured and do not have a TB lesion on CXR or persons who have TB lesions on CXR but did not undergo medical treatment are not included in prior TB group and that can be the cause of underestimation on the presence of past TB. Furthermore, the clinical characteristics of TB survivors who were cured and do not have a TB lesion or who have a TB lesion on CXR without treatment are poorly understood.
The aim of this study was to compare the clinical characteristics and pulmonary function of participants based on different evidence of previous TB infection (i.e. self-reported history or radiologic evidence) in a representative Korean national population study.
MATERIALS AND METHODS
Study population and data collection
This study was based on data obtained from the Korea National Health and Nutrition Examination Survey (KNHANES) between 2008 and 2012. The KNHANES is a cross-sectional, national surveillance system designed to examine the health and nutritional status of the non-institutionalized Korean population and is conducted by the Korea Centers for Disease Control and Prevention (KCDC). The KNHANES followed a multi-stage cluster probability sampling design to ensure independent and homogenous sampling for each year as well as nationally representative sampling (11). Among 23,612 subjects aged 40 years or older, a total of 13,522 participants who underwent CXR and spirometry with reliable spirometer data were eligible for the study. Subjects who had active TB (n = 26), and non-responders to the question regarding TB history were excluded from the study (n = 54) (Fig. 1).
Fig. 1
Flowchart of the study population.
KNHANES = Korean National Health and Nutrition Examination Survey, CXR = chest X-ray, TB = tuberculosis, Hx = history of physician diagnosis, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, TB Hx (−)/CXR (+) = subjects with TB lesions on CRX without a history of TB, TB Hx (+)/CXR (+) = subjects with both having a history of TB and TB lesions on CXR.

CXR
Since 2008, the KNHANES has included a TB section to their health survey by performing population-wide screening with CXR to estimate the national prevalence of pulmonary TB. CXR images were taken with DigiRAD-PG (Sitec Medical Co., Ltd., Kimpo, Korea), which were installed on the examination vehicle. The results of CXR allowed 2 radiologists to independently interpret the presence of lung disease, and individual readings were compared weekly, and CXR demonstrating TB related lesions were re-interpreted by 6 radiology specialists to confirm the results.
Definition of past TB
Persons having evidence of past TB were defined as those with a self-reported history of physician-diagnosed TB or TB lesions on CXR. Therefore, the subgroups of past TB were; 1) a history of TB without TB lesions on CXR (only a history of TB), 2) TB lesions on CXR without a history of TB (only TB lesions on CXR), and 3) having both a history of TB and TB lesions on CXR.
Measurement of pulmonary function
Pulmonary function was measured using a dry rolling seal spirometer (Model 2130; Sensor-Medics, Yorba Linda, CA, USA) according to the American Thoracic Society/European Respiratory Society criteria for standardization (12). Spirometric data obtained on site by clinical technicians was transferred to an internet review center for processing. The data was compared against criteria metrics for acceptability, reproducibility, and quality control. A principal investigator validated and stored the data in a KCDC repository management system. AFO is defined by a decrease of the pre-bronchodilator forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) below 70%. Severity of AFO was classified by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage system. Pre-bronchodilator FEV1/FVC ≥ 70% and FVC < 80% was defined as spirometric restriction.
Measurement of clinical parameters
Participants' demographics and previous medical history were collected from standardized health questionnaires. Information included lifestyle behaviors such as cigarette smoking and physical activity. Cigarette usage was divided into 2 categories: no history of smoking and ever smoker (those who had smoked 100 or more cigarettes over their lifetimes). Regular exercise was defined as engaging in moderate or vigorous exercise on a regular basis (20 minutes at least 3 times per week). The presence of respiratory symptoms was also surveyed.
Statistical analysis
Data were analyzed using the survey procedures of SAS version 9.2 (SAS Institute Inc., Chicago, IL, USA). To produce an unbiased national estimate, a sample weight was assigned for participating individuals in order to represent the Korean population. Sampling weights were constructed to account for the complex survey design, survey non-response, and post-stratification. Continuous variables were expressed as the mean with standard error and categorical variables as cases per category and frequency of responses. Baseline characteristics of past TB groups based on historical or radiographic evidence were analyzed by analysis of variance (ANOVA) or χ2 tests. The association of different groups for AFO or spiometric restriction was modeled by logistic regression after adjusting for age, gender, body mass index (BMI), education, income, and smoking. P for trend was calculated by assigning the mean or percentage values of lung function and odds ratio (OR) of distinct TB evidence groups as continuous variables. All statistical analyses were performed with SAS version 9.3 (SAS Institute Inc.), and a P value < 0.05 was considered to indicate statistical significance.
RESULTS
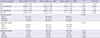
Among 13,522 participants, there were 1,372 (10.1%) persons with evidence of prior TB infection: 312 subjects (2.3%) had only a history of TB, 667 (4.9%) had only radiographic evidence of TB on CXR, and 393 (2.9%) had both a clinical history and CXR evidence of TB (Fig. 1). Participants having pulmonary TB lesion on CXR (with or without a history of TB) were more likely to be male, of older age, ever smokers, lower educational background, and be over lower income than those without TB on CXR. The participants with a history of TB without TB lesion were demographically similar to those without evidence of TB by gender, age, smoking history, education, and income (Table 1).
Table 1
Baseline characteristics of study population

Values are presented as frequency (and proportion), or means ± standard error.
TB = tuberculosis, Hx = history of physician diagnosis, CXR = chest X-ray, TB Hx (+)/CXR (−) = subjects with a history of TB without radiographic evidence of TB on CXR, TB Hx (−)/CXR (+) = subjects with TB lesions on CXR without a history of TB, TB Hx (+)/CXR (+) = subjects having both a history of TB and radiographic evidence of TB on CXR, BMI = body mass index.
*Exercise was defined as engaging in moderate or vigorous exercise on a regular basis (20 minutes at least 3 times per week).
The predicted FEV1 (P < 0.001), FVC (P = 0.006), and FEV1/FVC ratio (P < 0.001) were lower in the subjects with only a history of TB compared to subjects with no evidence of TB. The proportion of the subjects with respiratory dysfunction (P < 0.001), GOLD stage 2 or more (P < 0.001), and those with wheezing (P = 0.007) were higher in subjects with only a history of TB compared to subjects with no evidence of TB (Table 2).
Table 2
Comparison of pulmonary function and symptoms between subjects with no evidence of TB and subjects with history of TB without TB lesions on CXR
Values are presented as frequency (and proportion), or means ± standard error.
TB = tuberculosis, CXR = chest X-ray, Hx = history of physician diagnosis, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity, GOLD = Global Initiative for Chronic Obstructive Lung Disease.
*GOLD 1, ≥ 80% predicted FEV1; GOLD 2, 50%–80% predicted FEV1; GOLD 3, 30%–50% predicted FEV1; or GOLD 4, < 30% predicted FEV1.
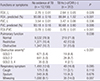
The predicted FEV1 (P < 0.001, P for trend < 0.001), FVC (P = 0.025, P for trend < 0.007), and FEV1/FVC ratio (P < 0.001, P for trend < 0.001) tended to be lower in those with only a history of TB, those with only TB lesion on CXR, and those with both a history and TB lesion on CXR. The proportion of the subjects with respiratory dysfunction (P < 0.001), and proportion of those at GOLD stage 2 or more (P < 0.001) were higher in the following order: those with both a history and TB lesion on CXR, those with only TB lesion on CXR, and those with only a history of TB (Table 3).
Table 3
Comparison of pulmonary function and symptoms amongst subjects with previous TB
Values are presented as frequency (and proportion), or means ± standard error.
TB = tuberculosis, Hx = history of physician diagnosis, CXR = chest X-ray, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, TB Hx (−)/CXR (+) = subjects with TB lesions on CRX without a history of TB, TB Hx (+)/CXR (+) = subjects with both having a history of TB and TB lesions on CXR, GOLD = Global Initiative for Chronic Obstructive Lung Disease.
*GOLD 1, ≥ 80% predicted FEV1; GOLD 2, 50%–80% predicted FEV1; GOLD 3, 30%–50% predicted FEV1; or GOLD 4, <30% predicted FEV1.
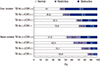
The proportion of those with respiratory dysfunction was more frequent in ever smokers than never smokers. Ever smokers had a higher proportion of AFO than spirometric restriction, otherwise, never smokers had a higher proportion of spirometric restriction (Fig. 2).
Fig. 2
Proportion of those with respiratory dysfunction among subjects with different evidence of TB by smoking status.
TB = tuberculosis, Hx = history of physician diagnosis, CXR = chest X-ray, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, TB Hx (−)/CXR (+) = subjects with TB lesions on CRX without a history of TB, TB Hx (+)/CXR (+) = subjects with both having a history of TB and TB lesions on CXR.
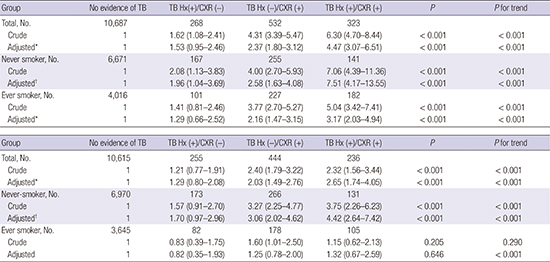
After adjusting for gender, age, BMI, education, income, and smoking, the adjusted OR for AFO tended to increase based on those with only a history of TB (OR 1.53, 95% confidence interval [CI] 0.95–2.46), only TB lesion on CXR (OR 2.37, 95% CI 1.80–3.12), and those with both a history and TB lesion on CXR, (OR 4.47, 95% CI 3.07–6.51; P for trend < 0.001) (Table 4).
Table 4
ORs (95% CI) of obstructive dysfunction in all participants with no evidence of pulmonary TB as a reference group

P for trend was calculated by OR of TB groups.
OR = odds ratio, CI = confidence interval, TB = tuberculosis, Hx = history of physician diagnosis, CXR = chest X-ray, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, TB Hx (−)/CXR (+) = subjects with TB lesions on CRX without a history of TB, TB Hx (+)/CXR (+) = subjects with both having a history of TB and TB lesions on CXR, BMI = body mass index.
*Age, sex, BMI, education, income, and smoking pack year; †Age, sex, BMI, education, and income.
After adjusting for gender, age, BMI, education, income, and smoking, the adjusted OR for spirometric restriction tended to increase based on those with only a history of TB (OR 1.29, 95% CI 0.80–2.08), only TB lesion on CXR (OR 2.03, 95% CI 1.49–2.76), and those with both a history and TB lesion on CXR (OR 2.65, 95% CI 1.74–4.05; P for trend < 0.001) (Table 5).
Table 5
ORs (95% CI) of restrictive dysfunction in all participants with no evidence of pulmonary TB as a reference group

P for trend was calculated by OR of TB groups.
OR = odds ratio, CI = confidence interval, TB = tuberculosis, Hx = history of physician diagnosis, CXR = chest X-ray, TB Hx (+)/CXR (−) = subjects with a history of TB without TB lesions on CRX, TB Hx (−)/CXR (+) = subjects with TB lesions on CRX without a history of TB, TB Hx (+)/CXR (+) = subjects with both having a history of TB and TB lesions on CXR, BMI = body mass index.
*Age, sex, BMI, education, income, and smoking pack year; †Age, sex, BMI, education, and income.
The magnitude of the OR of respiratory dysfunction was stronger in never smokers than in ever smokers. Never smokers with only a history of TB were independently associated with AFO (OR 1.96, 95% CI 1.04–3.69) after adjusting for gender, age, BMI, education, and income (Table 4).
DISCUSSION
In this national representative Korean population study of adults 40 years and over, the definition of past TB influenced the magnitude of association between past TB and respiratory dysfunction. AFO was independently associated with having only a clinical history of TB (OR 1.53, 95% CI 0.95–2.46), with having only TB lesion on CXR (OR 2.37, 95% CI 1.80–3.12), and with having both (OR 4.47, 95% CI 3.07–6.51). Two systematic reviews reported a significant association between past TB and AFO (OR 1.37–3.05) (45). The BOLD study reported that a self-reported history of TB was associated with AFO (OR 2.51) (6). The association between TB and AFO was strong in countries with a high incidence of TB and among never smokers (4). In our study, the magnitude of the OR between TB and AFO was much stronger amongst never smokers, suggesting that past TB is an important contributing factor to the development of obstructive lung disease among never smokers (1314).
The association between past TB and restrictive lung disease has rarely been reported in large population studies. In the present study, spirometric restriction was independently associated with subjects having only a history of TB (OR 1.29, 95% CI 0.80–2.08), having only TB lesion on CXR (OR 2.03, 95% CI 1.49–2.76), and with having both (OR 2.65, 95% CI 1.74–4.05). The BOLD study reported that a history of TB was associated with spirometric restriction (OR 2.13) (6).
In the present study, ever smokers had higher proportion of AFO compared to spirometric restriction whereas never smokers had a higher proportion of spirometric restriction compared to AFO. A study in sub-Saharan Africa wherein 90% of participations were never smokers with normal baseline lung function also revealed that restrictive pattern was dominant in post-TB spirometric changes (15).
Smoking modifies residual lung function impairment following treatment of TB. After 6 months of anti-TB therapy, the extent of initial radiographic infiltration predicted the degree of lung function impairment in never smokers but not in smokers (16). A retrospective multicenter study of Korean patients with TB-induced structural lung disease reported that with exacerbations, lung function progressively declined the FEV1 and FVC but that the FVC was significantly higher in patients with AFO than in those without AFO. Baseline demographic and radiologic characteristics were similar but the only significant difference was that the proportion of smokers was higher in patients with AFO than without AFO (17).
There is growing evidence of a bi-directional relationship between TB and chronic obstructive lung disease (COPD) (18). Smoking is a major, well-established risk factor for COPD (1920) and it is also known that smoking increases the risk of TB (2122). Patients with COPD had a 3-fold higher risk of developing TB compared to control subjects (23). Corticosteroid use for COPD treatment may be one of the contributing risk factors for infection with TB (24). In the present study, subjects having TB lesion on CXR compared to subjects without having TB lesion had a greater proportion of older age, male gender, ever smoker, and be of low socioeconomic status. It should be noted that subjects with TB lesion on CXR without a clinical history of TB had an increased risk of TB reactivation because a significant number of subjects already had AFO and did not receive proper anti-TB treatment. The presence of radiologic lesion on CXR consistent with old healed TB was reported as one of the strongest risk factors for the development of active TB (25).
In the present study, even subjects having only a history of TB were similar demographically to participants with no evidence of TB, but they had lower pulmonary function and a higher proportion of AFO as well as obstructive severity compared to the subjects with no evidence of TB. In never smokers, having a history of TB without TB lesion was independently associated with an increased risk of AFO (OR 1.96, 95% CI 1.04–3.69). Since having a history of TB itself is a risk factor of AFO, even patients who have successfully treated pulmonary TB without sequelae of TB on their CXR, should keep track of their pulmonary function after treatment of TB.
This study has some limitations. Firstly, because of the cross-sectional study design, we cannot rule out reverse causality as an explanation for the observed associations. Secondly, AFO was defined by FEV1/FVC rather than post-bronchodilator FEV1/FVC and spirometric restriction was defined by FEV1/FVC ≥ 70% and FVC < 80%. Total lung capacity (TLC) measurement is recommended in diagnosing restrictive lung disease (26). Using FVC as a surrogate of TLC may have low sensitivity and specificity for identifying restrictive patterns depending on the spirometry test quality (27). Measuring TLC by plethysmography and using bronchodilators, however, are unrealistic in large population studies and spirometry results in our study were stringently quality-controlled. Thirdly, the extent of TB lesions on CXR could not be evaluated due to limited information.
How prior infection with TB is defined in a population study can influence the magnitude of association between TB and respiratory dysfunction. Without considering TB lesions on CXR, the association between past TB and respiratory dysfunction may be underestimated in a population study. The pulmonary function was lower and the risk of respiratory dysfunction increased in the following order: in those with only a history of TB; those with only TB lesion on CXR; and those having both. Any evidence of past TB should be understood as a significant risk factor for respiratory dysfunction. With national TB control efforts, attention to the persons with past TB is crucial for population health, especially in countries with more than an intermediate burden of TB.
 XML Download
XML Download