

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Group B streptococcus (GBS, Streptococcus agalactiae) is an important pathogen among infants (1). Although the introduction of intrapartum antibiotic prophylaxis and maternal screening has reduced the incidence of invasive GBS disease (e.g., sepsis and meningitis) during recent years, the rates of morbidity and mortality from invasive GBS disease remain high in many countries (2). Preliminary epidemiological studies revealed a correlation between low concentrations of maternally derived antibodies against the capsular polysaccharide (CPS) of GBS and infants' susceptibility to GBS infection (345). Therefore, an intrapartum vaccine was developed to protect infants from invasive diseases, which generated transplacental-acquired serotype-specific capsular antibodies until the age of 3 months, as > 95% of invasive GBS diseases occur during this period (67).
Similar to protection against other bacteria (e.g., Haemophilus influenzae type b, Streptococcus pneumoniae, and Neisseria meningitides), protection against GBS generally involves antibody-mediated opsonization by phagocytes and complement components (8). Thus, the opsonization assay has become an important tool for assessing the immunogenicity of pneumococcal vaccines (9), and a multiplexed opsonophagocytic killing assay (OPA) was developed (10) to facilitate the widespread use of the pneumococcal opsonization assay. Burton and Nahm (The Bacterial Respiratory Pathogen Reference Laboratory, National Institutes of Health; University of Alabama at Birmingham [UAB]) (10) performed minor modifications to the OPA protocol and detected opsonic antibodies against GBS CPS in rabbit antisera (the UAB GBS OPA assay). This killing-type assay measures antibodies' specific abilities to actually kill bacteria by counting the surviving bacteria, although it has not been used to test human sera. In the present study, we used to UAB GBS OPA to evaluate the opsonization indices (OIs) of GBS Ia-, Ib-, and III-specific antibodies in the sera of Korean infants and in several commercial intravenous immunoglobulin (IVIG) products from different countries. The GBS Ia, Ib, and III serotypes were selected because they are included in a trivalent GBS vaccine formulation that is being developed (CRM197-glycoconjugate GBS vaccine) (1112).
MATERIALS AND METHODS
Bacterial strains
The GBS strains (serotype Ia: E-GBS 001, serotype Ib: E-GBS 002, and serotype III: E-GBS 003) were obtained from Dr. Hye-Kyung Cho (Gachon University, Gil Medical Center). The strains had been isolated from infants with invasive GBS diseases, and were stored at −80°C in 0.5 mL of Todd-Hewitt broth with 15% glycerol. GBS were identified based on the presence of gram-positive cocci in pairs or short chains, beta hemolysis on blood agar plates, catalase-negative results, and formation of a substance (Christie-Atkins-Munch-Petersen [CAMP] factor) that enlarges the hemolysis area formed by β-hemolysin from Staphylococcus aureus. The GBS serotype was identified using a slide latex agglutination test (Denka Seiken, Tokyo, Japan).
Infants' sera
This study evaluated sera from infants who underwent blood testing for health evaluations between 2009 and 2010. The sera were stored at −70°C until testing. Infants with known immune deficiencies or premature birth status (gestational age of < 37 weeks at birth) were excluded. Based on the available sera, we selected 103 sera from infants who were < 1-year old at the evaluation. The infants were stratified according to age using 1-month intervals (0 months to 11 months). Among the 103 sera, 98 sera were found to be free from antibiotics (based on their inability to inhibit the growth of R36A pneumococcal bacteria), and were incubated at 56°C for 30 minutes to inactivate endogenous complement activity before our testing.
Commercial IVIG products
Nineteen lots of IVIG products were analyzed in this study. Ten lots (Korea-A) and 6 lots (Korea-B) were obtained from 2 Korean manufacturers, separate lots were also obtained from 2 Japanese manufacturers (Japan-A and Japan-B), and 1 lot was obtained from an American manufacturer (US). To purify the IVIG, Korea-A, Korea-B, and US products had been treated using cold ethanol solvent/detergent, while the Japan-A and Japan-B products had been treated using polyethylene glycol. The Korea-A, Korea-B, and Japan-B products were formulated as liquids, while the Japan-A and US products were formulated as lyophilized powder. All IVIG products were formulated at a concentration of 50 mg/mL.
OPA for antibodies against GBS (the UAB GBS OPA assay)
Duplicate samples of sera or IVIG (20 µL) were serially diluted (1:3) in opsonization assay buffer B (OBB; Hanks' balanced salt solution [with magnesium and calcium] with 0.1% gelatin and 5% defined fetal bovine serum [6000; Gibco, Waltham, MA, USA]) in 96-well round-bottom plates. Frozen working stocks of each of the target strains were thawed and washed twice with OBB and centrifuged (12,000 × g for 2 minutes), then the bacteria were prepared in OBB to an approximately concentration of 1 × 105 colony-forming units (CFUs)/mL. Ten microliters of the bacteria were added to each well, and the plates were incubated at room temperature for 30 minutes with shaking. After the incubation, 10 μL of baby rabbit complement (BRC; Pel-Freez Biological, Rogers, AR, USA) were added to the wells, except for the control A wells, which received 10 μL of heat-inactivated BRC (heated at 56°C for 30 minutes). Forty microliters of differentiated HL60 cells (containing 4 × 105 cells) were added to all wells, and the plates were incubated for 45 minutes in a 37°C/5% CO2 incubator with shaking. Afterwards, 5-μL aliquots of the reaction product from each well were spotted onto THYA-NR plates (Todd-Hewitt agar [1.5%] with yeast extract containing neutral red [30 μg/mL] and 1M Tris solution [0.02M]) and the plates were incubated overnight (37°C/5% CO2). After the overnight incubation, the plates were removed from the incubator and left at room temperature for 4–5 hours, which decreased the background color. The numbers of surviving colonies on the plates (Fig. 1) were enumerated using NICE colony counting software (National Institute of Standards and Technology's Integrated Colony Enumerator; National Institute of Standards and Technology, Gaithersburg, MD, USA). OIs were calculated using linear interpolation. To facilitate the data analysis, an Excel-based data processing program was used to transfer the colony counts to an “opsonization index” program (“opsotiter3” from the UAB reference laboratory). The OI value was defined as the reciprocal of the interpolated dilution of serum that killed 50% of the bacteria. If an undiluted serum sample killed 50% of the bacteria, this produced an OI value of 4 in our system. A detailed protocol is posted at http://www.vaccine.uab.edu/.
Fig. 1
Microcolonies of serotype III GBS on a THYA-NR plate (Todd-Hewitt agar with yeast extract containing neutral red and Tris solution) after overnight incubation (37°C/5% CO2) and incubation for 4–5 hours at room temperature/room air. The numbers of surviving colonies were counted on the plates. The average diameter of the microcolonies was approximately 0.3 mm, and the colonies were clearly red and spatially separated.
GBS = group B streptococcus.

Statistical analysis
The geometric mean indices (GMIs) and associated 95% confidence intervals (CIs) were calculated for each of the serotypes. Differences in the GMIs among the IVIG products were analyzed using the Kruskall-Wallis test and the Mann-Whitney U test. Box and whisker plots were used to report the median, minimum, and maximum values, as well as the 25th and 75th percentiles for each group. Seropositivity was defined as the presence of detectable OI (≥ 4). Pearson's χ2 tests and Cochran's Q test were used to compare seropositive rates. The χ2 test for trend was used to evaluate the relationship between the seropositive rates and age. The linear correlations between the OIs and infant age (≥ 3 months) for each serotype were evaluated using Spearman's correlation coefficients. Serum samples with OIs of < 4 were assigned a value of 2 for the present analyses. Differences were considered statistically significant at a P value of < 0.05. Statistical analyses were performed using SPSS software (version 23.0; SPSS Inc., Chicago, IL, USA).
RESULTS
The OIs to serotype Ia, Ib, and III GBS among IVIG products
The box and whisker plots for OIs to serotype Ia, Ib, and III GBS among the 19 IVIG products are shown in Fig. 2. The OI values were 635–5,706 (serotype Ia), 488–1,421 (serotype Ib), and 962–3,315 (serotype III). None of the IVIG lots exhibited undetectable OI values (< 4). We observed lot-to-lot variations between the Korean manufacturers for serotype Ia (Korea-A: 635–987; Korea-B: 791–5,706) and serotype III (Korea-A: 1,223–1,823; Korea-B: 962–3,315), but not for serotype Ib (Korea-A: 488–568; Korea-B: 504–607). The GMI values were not significantly different between the Korean manufacturers for all 3 serotypes (Table 1).
Fig. 2
OIs for GBS according to serotype (Ia, Ib, and III) in various IVIG products (n = 19). The top bar is the highest value, the bottom bar is the lowest value, the top of the box indicates the third quartile, the bottom of the box indicates the first quartile, and the middle bar is the median value. The lower limit of detection for the opsonization index was 4. The numbers of lots are given in parentheses.
OIs = opsonization indices, GBS = group B streptococcus, IVIG = intravenous immunoglobulin.
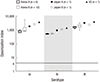
Table 1
OIs and seropositive rates for GBS (serotypes Ia, Ib, and III) in various IVIG products and in Korean infants

The OIs to serotype Ia, Ib, and III GBS among the infants' sera
The OIs of the infants' sera to GBS were 2–119 for serotype Ia, 2–2,486 for serotype Ib, and 2–1,557 for serotype III (Fig. 3). The seropositive rates were 18.4% (18/98) for serotype Ia, 38.8% (38/98) for serotype Ib, and 38.8% (38/98) for serotype III (Table 1). The seropositive rate for serotype Ia was significantly lower, compared to the rates for serotypes Ib or III. The seropositive rates were lowest for all 3 serotypes among infants who were 3–5 months old. The seropositive rates for each serotype were higher among younger infants (0–2 months old). Infant age of ≥ 3 months was positively correlated with the seropositive rates for each serotype. There were positive correlations between age and the OIs against serotypes Ia, Ib, and III (r = 0.49–0.57).

DISCUSSION
The present study revealed that several commercial IVIG products had functional antibodies to serotype Ia, Ib, and III GBS, regardless of their manufacturer's location. However, many infants did not have functional antibodies against the 3 GBS serotypes.
As IVIG is produced using pooled plasma from up to 100,000 donors (13), it contains a wide range of immunoglobulin G (IgG) to many microorganisms, which reflects the donors' cumulative environmental exposures. Many previous studies have measured the titers of antibodies in commercial IVIG products to encapsulated bacteria, such as H. influenzae type b (14), meningococci (15), and pneumococci (1416). However, to the best of our knowledge, no studies have measured the titers of functional antibodies to GBS in IVIG products. The present study's findings of functional antibodies to serotype Ia, Ib, and III GBS in commercial IVIG, regardless of the donor population, is to be expected, as GBS is a human commensal in the gastrointestinal and genital tract that does not typically cause infection or disease (17). Among pregnant women, the rate of GBS carriage in the vaginal and rectal microbiota is similar in both developing and developed countries (181920), although large variations in the colonization rates are observed in different populations (21). In Korea, the reported carriage rates are 6.3%–11.5% among pregnant women (222324). However, the titers of pathogen-specific antibodies in IVIG may varying according to the plasma source, as they are influenced by the cumulative environmental exposure of the donor population. Therefore, continuous testing of antibody titers is needed to monitor different IVIG products from different countries.
In contrast with our findings from the IVIG products, most infants in the present study (61.2%–81.6%) did not have functional antibodies to the 3 GBS serotypes. Furthermore, the seropositive rate for serotype Ia was especially low, compared to the rates for serotypes Ib or III. Nevertheless, infant age of ≥ 3 months was positively correlated with the seropositive rates for each serotype. Moreover, there were positive correlations between age and OIs in the infants' sera, which exhibited moderate variations according to serotypes. These results suggest that, even during infancy, specific functional immune responses to the 3 GBS serotypes can be achieved through a commensal in the gastrointestinal or genital tract, without causing infection or disease at older ages.
The delayed immunoglobulin synthesis and low rate of transplacental antibody transfer in neonates suggest that IVIG may be a useful adjunctive therapy for treating GBS infections. In addition, IVIG may reduce the morbidity and mortality that is associated with GBS infections in high-risk neonates (25). In this context, IVIG provides immune protection in experimental models of GBS infection. However, meta-analyses of IVIG for treating cases of suspected or proven neonatal sepsis have revealed conflicting results, although these studies did not specifically target GBS sepsis (2627). Moreover, several studies have revealed that, compared to IVIG preparations from adults who were immunized with GBS (hyperimmune IVIG), standard IVIG preparations contain only modest levels of antibodies to GBS (28), exhibit dose- and preparation-dependent variations in their in vitro opsonophagocytosis, and are significantly less protective in experimental infection models. Baker et al. (29) have reviewed the studies regarding IVIG in human neonates and reported inconclusive findings, which were related to the small numbers of included infants, the lack of suitable controls, the use of a clinical definition for sepsis (vs. a strict microbiological definition), and single-center study designs. Thus, further studies are needed to provide evidence regarding the efficacy of IVIG for treating neonatal GBS sepsis.
The GBS Ia, Ib, and III serotypes selected in this study are included in the trivalent GBS vaccine formulation (1112). Based on the serotype distribution in South Africa, a GBS vaccine that incorporates these 3 serotypes is estimated to help prevent 85% and 98% of early-onset and late-onset invasive disease, respectively, among infants (30). Another study revealed that a pentavalent vaccine (serotypes Ia, Ib, II, III, and V) was estimated to prevent up to 98% of neonatal disease and 88% of pregnancy-associated disease in the US (1). Moreover, a conjugate vaccine incorporating the 5 GBS serotypes (Ia, Ib, II, III, and V) could prevent > 85% of GBS disease among < 3-month-old infants throughout the world (31). In Korea, the most prevalent serotypes are III, V, and Ia (in that order) (222324), and different populations exhibit varying serotype distributions (3031). Therefore, further studies are needed to consider the other serotypes (II and V) in their analyses.
In the present study, we used the UAB GBS OPA to measure the titers of serotype-specific antibodies to GBS. Similar to other encapsulated bacteria, protection against GBS is generally mediated by serotype-specific antibodies, which can be evaluated using enzyme-linked immunosorbent assays (ELISA) (35). However, ELISA typically only measures IgG, and recent evidence has revealed that IgM contributes to opsonization-related immune protection against pneumococci among children and adults (3233). Moreover, ELISA does not measure the functional capacity of the antibodies, and simply evaluates their capacity to bind antigens that are coated on a plate (34). Thus, we believe that the UAB GBS OPA function assay is useful for measuring serotype-specific antibodies to GBS in sera and IVIG. An OPA using adult polymorphonuclear leukocytes was developed in 1992 (35), and it expressed opsonophagocytic activity as the log10 reduction in the CFU/mL of GBS, compared to the control well (35). However, the UAB GBS OPA has several unique features: the ability to use frozen aliquots of target bacteria, the use of cultured cells as phagocytes (HL60; effector:target ratio of 400) (36), and automated colony counting (37), based on the use of a chemical that colors GBS colonies growing on the agar plate. Moreover, the OI is calculated as the reciprocal of the interpolated dilution of serum that kills 50% of the bacteria. Thus, this OPA method is both quicker and simpler, compared to the previous OPA method. As the UAB GBS OPA assay provides an excess number of functional phagocytes (HL60 cells), the same assay conditions can be used for evaluating opsonic antibodies to pneumococci and the efficacy of pneumococcal vaccines (910).
The present study has several limitations. First, an OPA titer of 8 is an important threshold for providing protection against most pneumococcal serotypes among children (9), although no such threshold has been established for protecting against GBS. Nevertheless, GBS serotype-specific antibody titers have been suggested in recent studies (383940), and those findings may be useful for developing appropriate cut-off values. Second, we only included a small number of IVIG products from Japan and the US, which precluded any definitive comparisons with the Korean IVIG products. Third, we did not compare the titers of functional antibodies in the mothers and their infants, and further studies are needed to address this issue.
In conclusion, we established the clinical utility of the UAB GBS OPA. This assay revealed that current IVIG products have opsonic antibodies against the 3 GBS serotypes. However, most of the Korean infants in this study did not have opsonic antibodies. Therefore, further studies are needed to evaluate the clinical utility of IVIG in infants with limited immunity, as well as the seroprevalences of other serotypes. Moreover, studies are needed to target different age groups and IVIG products from a greater number of manufacturers.
 XML Download
XML Download