

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary airway tumors originating from the larynx, trachea, and bronchi are rare in the pediatric and adult populations. Previous studies show that these tumors account for less than 0.1% of all tumors in adults (123). Primary malignant tumors of the lung and large airway represent only 0.2% of all pediatric malignancies (4).
Early and accurate diagnosis of a primary airway tumor is particularly important. Although it is a benign airway tumor, it has the potential to become dangerous if it is obstructing a central airway, creating a life-threatening consequence requiring emergency care (5). Tracheal tumors that obstruct 50% to 75% of the lumen does not necessarily produce symptoms in children (6). Therefore, tracheal tumors are difficult to diagnose until urgent symptoms appear. Some bronchial tumors are asymptomatic and may be diagnosed incidentally by an imaging study (7).
In general, the signs, symptoms, and radiologic features of a primary lung and airway tumor depends on the location (8). However, most reports in the literature of these tumors in children are case reports or series and are rarely sufficient. Fauroux et al. (9) compared the clinical characteristics and outcomes of carcinoid tumors in 6 patients and mucoepidermoid carcinoma (MEC) in 11 patients, but only in patients with bronchial tumors. Yu et al. (10) compared the clinical characteristics and outcomes of 35 adults and 19 children with tracheal and bronchial tumors. Eyssartier et al. (11) and Roby et al. (12) only described the characteristics and outcomes of cases of 12 bronchial and 14 tracheobronchial patients, respectively.
To date, there is little information are available on tumors of the airway, from the larynx to bronchus in children. Little effort has been made to compare the clinical characteristics of primary airway tumors in children based on the location. Therefore, we performed a study to identify the difference in clinical characteristics, imaging findings, and prognosis based on the location from larynx to bronchi, in Korean children with primary airway tumor.
MATERIALS AND METHODS
Study subjects and design
A retrospective chart review of children with tumors of the larynx, trachea, and bronchi at the Asan Medical Center from January 2000 to July 2016 was conducted. All cases were of patients under 18 years of age and we focused to tumors originating from the primary airway. We documented the following detailed information: age at onset and diagnosis; sex; presenting symptoms and signs at diagnosis; location of tumor; results from imaging studies (simple radiographs and chest computed tomography [CT]), laryngoscopies, and flexible bronchoscopies; the pathologic diagnosis; the treatment and duration; and outcomes (recurrences) at follow-up.
Laryngoscopy, flexible bronchoscopy
Laryngoscopy was performed in 8 children with an Olympus ENF-P4 (3.4 mm diameter; Olympus America Inc., Melville, NY, USA). It was advanced along the midline in the oral cavity with minimal force. Flexible bronchoscopy was performed on 7 pediatric patients using an Olympus BF-N20 (2.2 mm external diameter; Olympus America Inc.) and an Olympus BF-Xp40 (2.8 mm external diameter; Olympus America Inc.). Laryngoscopies and bronchoscopies were performed by a medical specialist at the Department of Otolaryngology and Pediatric Pulmonology and attended by at least 1 pediatrician with experiences at least 5 years, 1 intern, and 1 nurse.
Pathologic diagnosis
Histopathologic slides were prepared and stained by routine hematoxylin-eosin for recurrent respiratory papillomatosis (RRP), pleomorphic adenoma, fibrous histiocytoma, hemangioendothelioma and hamartoma, as well as immunohistochemical staining (e.g., S-100 protein for granular cell tumor, CD99 for Ewing's sarcoma). MEC is histologically diagnosed by Alcian blue and periodic acid-Schiff staining.
Definition of terms
Age at onset was defined as the age when major symptoms associated with an airway tumor became apparent in patients prior to visiting our hospital. Age at diagnosis was defined as the age when the pathologic diagnosis was confirmed except hemangioma, in which diagnosed as laryngoscopy and chest CT. Interval between onset and diagnosis was the number of months between the age at onset and age at diagnosis. Symptoms or signs were defined as the main symptoms or signs at the time when the patient presented our hospital. Finally, the duration of follow-up duration was based on medical records. Patients who were lost to follow-up or the period after patients were moved to their relevant place, were not taken into account.
Statistical analysis
Statistical analysis was performed with Statistical Package for the Social Sciences (SPSS) version 23.0 (IBM Corp., Chicago, IL, USA). The Pearson's χ2 test was used to compare the categorical variables based on the location of the tumors in the airway. The Kruskal-Wallis test was used to compare the continuous variables based on the tumor location in the airway. P < 0.05 was considered statistically significant.
RESULTS
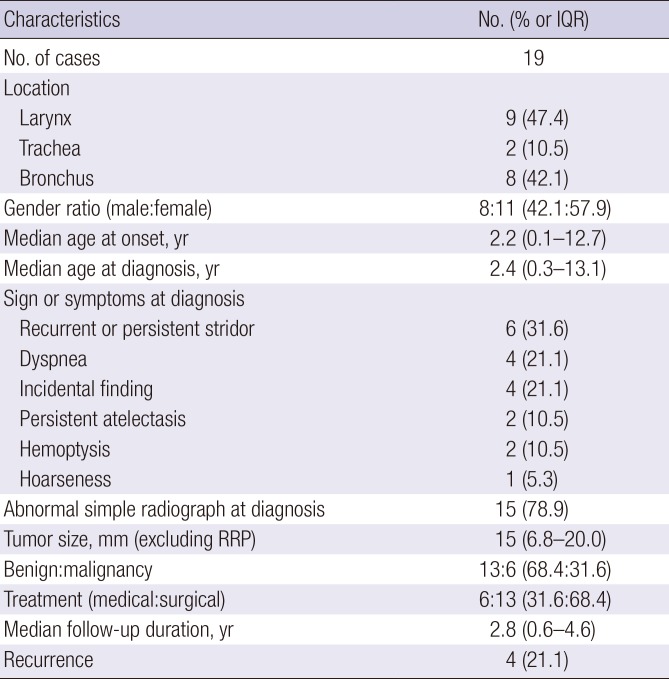
Basic demographics of all 19 patients (9 larynx, 2 trachea, and 8 bronchus tumors) summarized in Table 1. Common presenting symptoms or signs at diagnosis included recurrent or persistent stridor and dyspnea. Benign tumors were twice as common as malignant tumors.
Table 1
Basic demographics in total patients
Clinical characteristics and outcomes of children with tumors in the larynx
Nine patients were diagnosed with laryngeal tumors (Table 2). The median age at onset was 2 months (interquartile range [IQR], 0.9–22 months) and age at diagnosis was 4 months (IQR, 2.5–26 months). The most common presenting symptom and sign was recurrent stridor (n = 5). Simple radiograph images were normal in 4 and abnormal in 5 patients. Chest CT showed a small mass with a median size of 5.3 mm (IQR, 4.0–10.0 mm). Most laryngoscopy was performed before the chest CT in 8 of the 9 cases, leading to early diagnosis (Fig. 1). Laryngoscopy was used to determine the severity of airway obstruction and chest CT characterized and confirmed hemangiomas. RRP and Ewing's sarcoma were confirmed by surgical biopsies. Finally, 6 patients had subglottic hemangiomas, 2 patients had extensive RRP in the laryngeal area, including the vocal cord and 1 patient was diagnosed with Ewing's sarcoma in the true vocal cord. The Ewing's sarcoma patient was operated on with CO2 laser-assisted laryngomicrosurgery (LMS) using micro forceps and intralesional injection of mitomycin-C. Chemotherapy and radiotherapy were combined after LMS. Median follow-up duration was 1.4 years (IQR, 0.3–6.0 years) and no recurrences were observed, except in patients with RRP.
Table 2
Clinical characteristics and outcome in children with laryngeal tumor
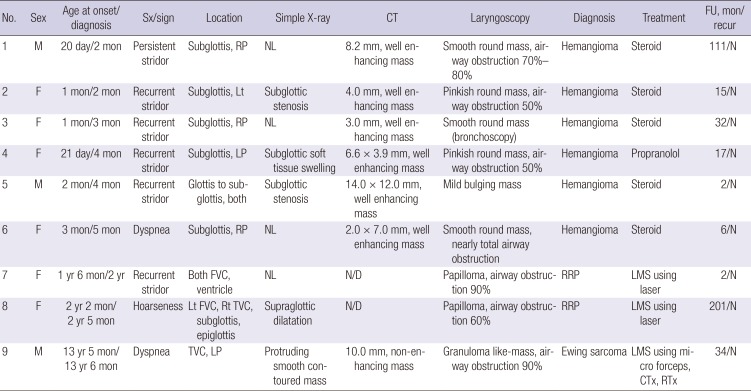
Sx = symptom, CT = computed tomography, FU = follow-up, recur = recurrence, M = male, RP = right posterior, NL = normal, N = no recurrence, F = female, Lt = left, LP = left posterior, FVC = false vocal cord, N/D = not done, RRP = recurrent respiratory papillomatosis, LMS = laryngomicrosurgery, Rt = right, TVC = true vocal cord, CTx = chemotherapy, RTx = radiotherapy.
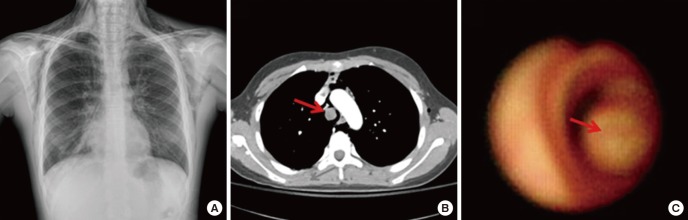
Fig. 1
Laryngoscopic findings demonstrating the tumor in the larynx (refer to Table 2). (A) RRP in both FVC and ventricle (thin circle), patient No. 7. (B) Subglottic hemangioma (thin circle), patient No. 4, (C) Ewing sarcoma (thin circle), patient No. 9.
RRP = recurrent respiratory papillomatosis, FVC = false vocal cord.

Clinical characteristics and outcomes of children with tumors in the trachea
Two patients were identified with tracheal tumors (Table 3). The median age at onset and diagnosis were 12 years and 4 months and 12 years and 10 months, respectively. Before admission, these 2 teenagers had been evaluated for dyspnea during the previous 5 months. Medical records described refractory asthma as being unresponsive to inhaled bronchodilators and corticosteroids. In patient No. 1, chest CT images showed large protruding masses with 15.0 mm in the right margin of the trachea and diagnostic bronchoscopy was performed and pathology revealed a benign pleomorphic adenoma (Fig. 2). Median follow-up duration for the tracheal tumors was 4.2 years and neither patient had evidence of tumor recurrence.
Table 3
Clinical characteristics and outcome in children with tracheal tumors

Fig. 2
Work-up findings showing the pleomorphic adenoma in the trachea, patient No. 1 (refer to Table 3). (A) Extensive subcutaneous emphysema with pneumomediastinum on chest X-ray. (B) Homogenous mass on chest CT (thin arrow). (C) Severe airway obstruction on bronchoscopic view (thin arrow).
CT = computed tomography.
Clinical characteristics and outcomes of children with tumors in the bronchi
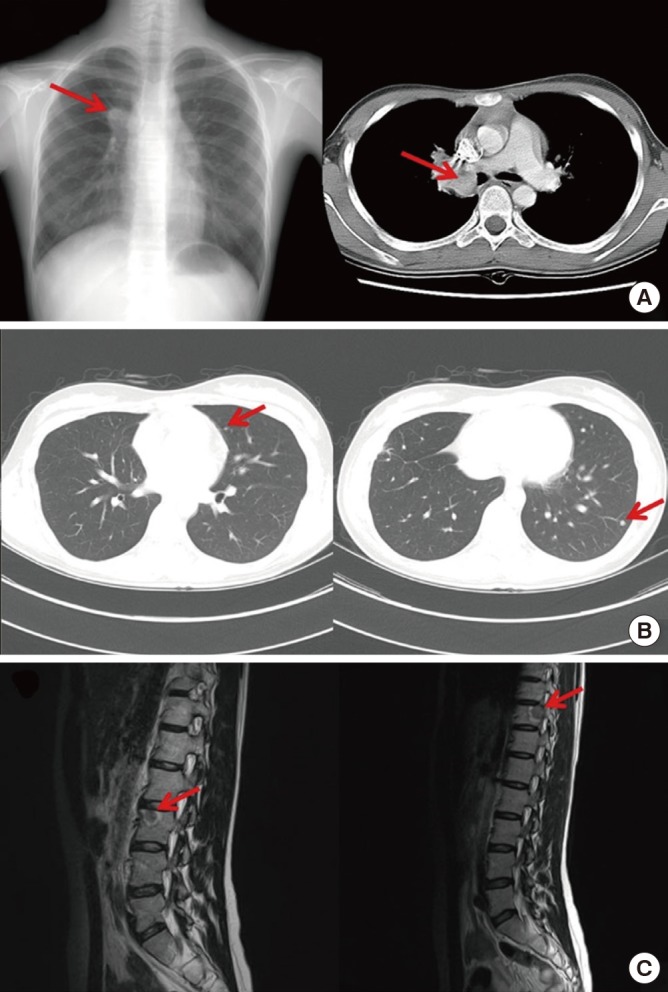
Eight children were found to have bronchial tumors (Table 4). The median age at onset was 136 months (IQR, 37–154 months) and age at diagnosis was 138 months (IQR, 36–160 months). Only 2 patients were symptomatic and presented with hemoptysis. The main radiograph findings were lobar atelectasis (62.5%) and unilateral emphysematous changes (25%). The median size of tumor was 20.0 mm (IQR, 16.8–23.0 mm). Pathologic diagnosis of the tumor was made by surgical resection for 5 patients, bronchoscopy for 3 patients, and a CT-guided biopsy for 1 patient. Four patients, who were over 10 years of age, had malignancies (3 MEC and 1 carcinoid tumor). Patients younger than 10 years of age had benign tumors. The median duration of follow-up was 7.0 years (IQR, 2.9–12.3 years); and 2 patients experienced recurrence after surgical intervention. Patient No. 7 exhibited recurrence as evidenced by a mass-like lesion seen on a simple radiograph during follow-up 9 years later. The chest CT image revealed the recurrence of a carcinoid tumor on the left upper and lower lobes, which was successfully removed by wedge resection. The second recurrence occurred 4 years after wedge resection and had metastasized to the 11th thoracic vertebrae and 3rd lumbar vertebrae (Fig. 3). The patient is now being treated palliatively with radiotherapy. Patient No 4. had a local recurrence in the same location 3 months after bronchoscopic laser ablation. The patient underwent a repeated laser ablation and is disease-free after 2 years of follow-up.
Table 4
Clinical characteristics and outcome in children with bronchial tumors
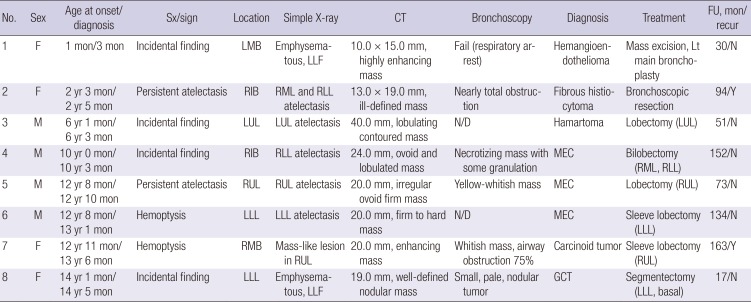
Sx = symptom, CT = computed tomography, FU = follow-up, recur = recurrence, F = female, LMB = left main bronchus, LLF = left lung fields, Lt = left, N = no recurrence, RIB = right intermediate bronchus, RML = right middle lobe, RLL = right lower lobe, M = male, LUL = left upper lobe, N/D = not done, MEC = mucoepidermoid carcinoma, RUL = right upper lobe, LLL = left lower lobe, RMB = right main bronchus, GCT = granular cell tumor.
Fig. 3
Carcinoid tumor in RMB indicated thin arrow, patient No. 7 (refer to Table 4). (A) Well-enhanced mass, initial chest X-ray and CT. (B) First metastasis on LUL and LLL, chest CT. (C) Second metastasis to L3 and T11, sagittal T2-weighted MRI.
RMB = right main bronchus, CT = computed tomography, LUL = left upper lobe, LLL = left lower lobe, MRI = magnetic resonance imaging.
Comparison of clinical characteristics among children with a tumor in the larynx, trachea, and bronchi
We compared the clinical characteristics among children with airway tumors based on tumor location, including the larynx, trachea, and bronchi (Table 5). Laryngeal tumors (median age, 4.0 months; IQR, 2.5–26 months) were diagnosed earlier (P = 0.004) than both tracheal (154 months) and bronchial tumors (median age, 138 months; IQR, 36–160 months). Likewise, age at onset of symptoms or signs was younger in children with laryngeal tumor (median age, 2.0 months; IQR, 0.9–22 months) than in those with both tracheal (148 months) and bronchial tumors (median age, 136 months; IQR, 37–154 months; P = 0.049). However, the interval between diagnosis and onset was not significantly different among children with laryngeal, tracheal, and bronchial tumors, although the interval in those with tracheal tumors (5.5 months) was slightly longer than those with both laryngeal (median age, 2.0 months; IQR, 0.7–2.7 months) and bronchial tumors (median age, 2.5 months; IQR, 2.0–4.5 months).
Table 5
Comparison of characteristics between the 3 locations
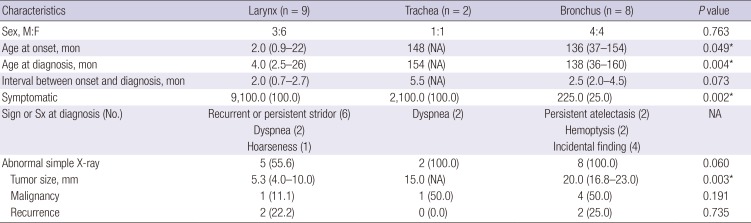
All children with laryngeal or tracheal tumors had respiratory symptoms, but only 2 children (25%) with bronchial tumors had such symptoms (P = 0.002). All children with tracheal and bronchial tumors showed abnormal simple radiograph findings, but 4 children with laryngeal tumors had normal radiograph (P = 0.060). Bronchial tumors were significantly larger (median size, 20.0 mm; IQR, 16.8–23.0 mm; P = 0.003) than laryngeal (median size, 5.3 mm; IQR, 4.0–10.0 mm) and tracheal tumors (median size, 15.0 mm). There was no difference in sex, malignancy, and recurrence.
DISCUSSION
This study analyzed 9 larynx, 2 trachea, and 8 bronchus tumors. The differences between the 3 locations were median age at onset and diagnosis, presence of symptoms, and median size of the tumors. To the best of our knowledge, this is the first study in Korea which included the most diverse specimen of airway tumors and compared the clinical characteristics based on the tumor location.
Patients with tumors in the larynx (referred to as the upper airway) were younger at onset and diagnosis than those with tumors in the bronchus and trachea (referred to as the lower airway) in our study. In the pediatric age group, common laryngeal tumors are hemangioma and papillomas (13). Subglottic hemangiomas are uncommon congenital benign vascular neoplasms (14); and most patients present the symptoms before the age of 6 months (15). RRP is believed to be caused by human papillomavirus (HPV), usually type 6 or 11, transmitted from infected mothers to their infants (16). The classic presentation in those children is persistent hoarseness or weak crying, occurring between 2 and 4 years of age (17). Therefore, laryngeal tumors are diagnosed early because they trigger upper airway symptoms due to the obstruction in early life.
In our study, patient No. 8 with RRP had frequent recurrence after the first LMS. The patient developed lung involvement with air-filled cystic lesion after 14 years of follow-up. The cystic lesion is under observation and has not caused any particular problems until now. Concomitant pulmonary parenchymal papillomas are present in less than 1% of affected patients (18). Such pulmonary parenchymal papillomas are believed to be caused by the seeding originating from the more proximal disease during endoscopic evaluation and treatment (1920).
In contrast, because an obstruction of 50% to 75% of the lumen by tracheal tumor does not always produce symptoms (6), correct diagnosis is delayed in tracheal tumor. Moreover, bronchial tumors usually appear through incidental findings or as a persistent chest infiltration, rather than triggering symptoms of severe airway obstruction. Therefore, they also have a frequent delayed diagnosis. Previous studies reported that most laryngeal tumors tend to occur in infants, while tracheobronchial tumors tend to occur in adolescents (101221). These findings are consistent with the median age at diagnosis and onset found in our study.
Our study found that the presence of symptoms was directly related to the location of the tumors, with the most statistical significance. The centrally located tumors are more likely to cause symptoms than tumors with peripheral location (2223). Our patients with tumors in the larynx and trachea were symptomatic at diagnosis, compared that 75% of the bronchial tumors were asymptomatic. Notably, most laryngeal tumors had a previous history of recurrent croup such as stridor and 2 tracheal tumors had a prolonged history of refractory asthma. Most cases of bronchial tumors had persistent lobar atelectasis, although with no respiratory symptoms. These finding suggest that if we suspect an airway tumor in children who have symptoms of airway obstruction, the symptoms and signs of the patients would help distinguish the location of the airway tumor.
In addition, chest radiograph is a useful for diagnosing an airway tumor. In patients with trachea-bronchial tumors, the chest radiographs always revealed abnormalities (21242526). The abnormal findings in our study included lobar atelectasis, air-leak syndrome and emphysematous changes due to obstruction. Previous studies commonly showed lobar atelectasis or unilateral overinflation involving the bronchi, especially in patients with bronchial tumors (1011). Simple radiographs of patients with laryngeal tumors had mostly normal findings, although some findings mimicked the radiograph finding of croup. If further localization or exclusion of lymphadenopathy and extension of the neoplasm is required, a chest CT has been shown to be efficacious (27). Endoscopy is indicated as the diagnostic test of choice because it is particularly helpful in evaluating the presence of intraluminal lesions and can facilitate diagnosis with biopsy (6).
Malignancy rate in this study is consistent with the previous findings that most primary airway tumors are usually malignant in adults, but benign in children (20). Benign neoplasms are located in the proximal portion of the central airways, while malignant neoplasms such as carcinoid tumors and MEC tend to be located in the distal trachea or bronchi (122829). In malignancy, previous data showed that carcinoid tumors accounted for about 50% of primary malignant lung tumors in patients under the age of 19 years and MEC consisted of < 10% of these tumors (30). However, in a study of Asian patients (10), there were only 2 carcinoid tumors while 73% were MEC, which presented a difference in occurrence when compared with the data previously reported in Western studies. Our study also showed that 25% of carcinoid tumors and 75% of MEC were malignant, comparable with the Asian study.
Ewing's sarcoma, rhabdomyosarcoma, and other malignant tumors rarely involve the larynx (16). Ewing's sarcoma originating from the larynx is even more unusual. To the best of the authors' knowledge, only 2 pediatric cases of laryngeal Ewing's sarcoma have been reported in the literature; one in a newborn (16) and another in a male 9-month-old infant (31). In this article, we reported on a third case of laryngeal Ewing's sarcoma in a 13-year-old male.
Three patients had local recurrences (2 patients with RRPs and 1 patient with a fibrous histiocytoma) and 1 patient had systemic metastasis 9 years after the surgical removal of a bronchial carcinoid tumor. Other studies reported 2 patients with local recurrences of a MEC, 4 and 8 years after successful removal (9). The indolent growth of all endobronchial tumors and the potential for local or distant recurrence should always be considered during follow-up (21). The risk of recurrence justifies a long-term clinical follow-up, at least 10 years after removal, specifically for malignant tumors (11).
Our study is limited because it is a retrospective, single-center study. Further investigation and detailed studies are required for a better understanding and evaluation. Due to the lack of prospective data, we were unable to estimate the incidence of airway tumors of children in Korea. In regards to the outcomes of the study patients, follow-up could only be determined based on clinical visits to the institution where this study was conducted. Also, recurrence or malignant transformation rates might have been underestimated if the patients were either still undergoing follow-up or were unavailable for follow-up, including transfer to another hospital.
This study suggests that we should consider the different tumor locations based on the age at onset and diagnosis, initial presence of symptoms, and median size of the tumors. We may be able to predict the malignant potential of the tumor and recurrence depending on location. It is for this reason that we demonstrated and compared clinical characteristics based on the location of the tumor in the airway. Considering the fact that recurrences have been reported many years after surgery, long-term follow-up, perhaps even life-long follow-up, is essential.
 XML Download
XML Download