

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of urolithiasis varies between 2% and 20% worldwide, and seems to depend on the geographic location and socioeconomic characteristics of different populations (12). The incidence of urolithiasis in Korea has progressively increased, as has the incidence in other developed countries (345). Despite the complexity of the etiology of urolithiasis, intrinsic and environmental factors contribute to increased urolithiasis, and improvements in diagnostic procedures increase observation of these stones. ‘Westernization’ of diets and sedentary lifestyles are factors that contribute to obesity and the metabolic syndrome (678). Obesity increases urinary excretion of metabolites that promote crystallization and urine acidity, and it contributes to an increase in calcium oxalate lithogenesis (9). Both hypertension and diabetes mellitus are also associated with significant changes in urinary chemistry, which affect the crystallization of various stone-forming salts (10). Epidemiological data suggest that a link exists between hyperlipidemia and urine metabolic profiles and stone composition (11). Thus, we hypothesized that urinary composition and lithogenic risk in patients with urolithiasis might have changed over time along with these clinicopathological variables. Understanding these chronological trends is important to enable the development of appropriate public-health strategies for stone prevention. We therefore determined the levels of urinary lithogenic risk in patients attending our clinic over the past 20 years. To our knowledge, only one previous study has evaluated the long-term trends of urinary lithogenic risk in patients with urolithiasis in Korea; this study by Kim et al. (12) involved a retrospective analysis of metabolic assessments in 619 patients with calcium stone former over a period of 14 years.
The present study was designed to assess the chronological trends of clinical and metabolic features over 20 years in Korean patients with urolithiasis. Patients were categorized into 4 groups according to the date of the initial diagnosis, and measurements of clinicometabolic characteristics and stone composition were compared.
MATERIALS AND METHODS
Study population
The study involved a retrospective analysis of 4,076 consecutive patients with a first-time stone episode, who were diagnosed and treated between 1996 and 2015 at our institution. Data were collected on stone history, body mass index (BMI), metabolic evaluation (including serum and 24-hour urine chemistry), and radiographic imaging of the urinary tract. Urinary stone formation was diagnosed by radiological modalities such as abdominal radiography, ultrasonography, and noncontrast computerized tomography. Exclusion criteria consisted of any of the following factors: urinary bladder stone, urethral stone, or staghorn calculi; pediatric patients (younger than 16 years); incomplete 24-hour urine collection (creatinine < 17 mg/kg per 24 hours in men and < 13 mg/kg per 24 hours in women); impaired renal function or the presence of a single kidney; urological malformation; urinary tract obstruction; or metabolic disease that could affect calcium and bone metabolism.
Measurement and definition of parameters
Urinary metabolic data were available in 1,421 patients (34.9% of the total cohort), and stone analysis data were available in 723 patients (17.7% of the total cohort). Medications that could affect serum and 24-hour urine chemistry results were discontinued at least 2 weeks before complete metabolic evaluation. The metabolic evaluation was performed at least 4 weeks after completion of stone management. Urinary metabolic abnormalities were classified by using the definitions of Lifshitz et al. (13) and Norman (14). Specific metabolic evaluation was indicated in high-risk stone formers including early onset of urolithiasis, familial stone formation, uric acid or brushite-containing stones, solitary kidney, anatomical abnormalities, and metabolic disease that could affect calcium and bone metabolism according to guidelines (114). In addition, metabolic evaluation was also performed even first stone formers without above stone forming risk. In this cases, the decision to perform the metabolic evaluation was made entirely by the patients. Stone samples were sent for analysis of composition by Fourier-transform infrared spectrometry (Green Cross, Yongin, Korea).
Statistical analysis
Patients were categorized into 4 groups according to the date of initial diagnosis, as shown in Table 1. Differences in urine variables between groups were assessed by the Kruskal-Wallis test. Categorical variables were compared by χ2 test or Fisher's exact test if appropriate. All statistical analyses were performed using SPSS ver. 21.0 software (IBM, Armonk, NY, USA). All tests were performed with 2-tailed analyses and P < 0.05 was considered statistically significant.
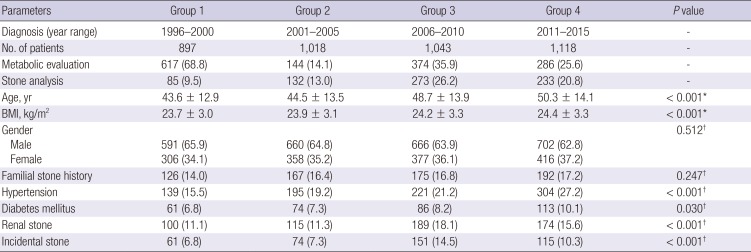
Table 1
Chronological trends of clinical features of patients with urolithiasis diagnosed over 20 years
Ethics statement
The study was carried out in agreement with the applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of Chungbuk National University approved this study protocol (Approval number: 2011-04-004). Informed consent was waived by the board.
RESULTS
Chronological trends in clinical features over the study period of 20 years
Patient demographics of the study population (n = 4,076) are detailed in Table 1. Statistical analysis indicated significant differences between the means of BMI and age in the different groups, and both sets of values increased as time progressed. Similarly, the prevalence of diabetes mellitus and of hypertension increased from one group to the next throughout the study period. The male:female ratio and prevalence of family history of urolithiasis did not differ between the groups. The prevalence of renal stones and incidental stones showed overall increases from the first to the last time period.
Chronological trends in urinary metabolic features over the study period of 20 years
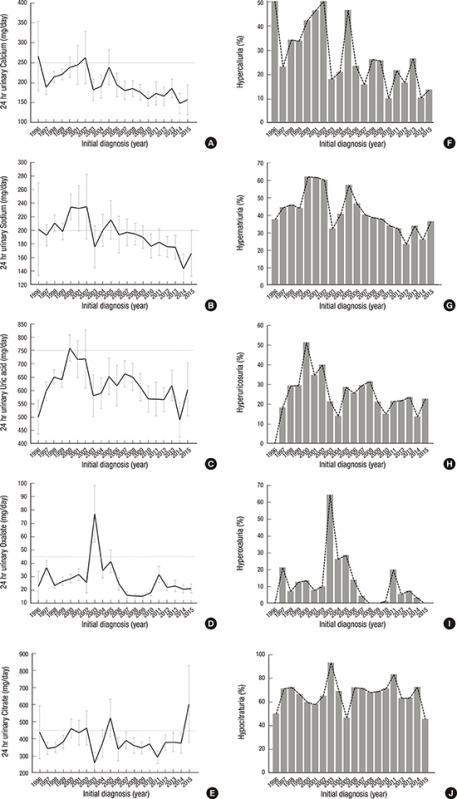
Urinary metabolic profile data and the prevalence of urinary metabolic abnormalities for patients in each year of the study period are shown in Fig. 1, and for patients in each 5-year period are shown in Table 2. Differences between mean values of 24-hour urine constituents, or between proportions of patients with metabolic abnormalities, across the 4 groups were determined by statistical analyses. Significant differences were seen in 24-hour urinary excretion of sodium, calcium, uric acid, magnesium, and oxalate between the groups, which corresponded to observations of reduced excretion across the study period. Similar patterns of decreased prevalence of the urinary metabolic abnormalities hypernatriuria, hyperuricosuria, hypercalciuria, and hyperoxaluria were also observed. By contrast, 24-hour urinary citrate excretion, urine volume and pH did not differ between the groups (all P > 0.05).
Fig. 1
Annual levels of urinary stone-forming constituents in patients with urolithiasis over 20 years. Mean 24-hour urinary excretion of calcium (A), sodium (B), uric acid (C), oxalate (D), and citrate (E) (error bars represent 95% CIs) and the incidence of urinary metabolic abnormalities, hypercaliuria (F), hypernatriuria (G), hyperuricosuria (H), hyperoxaluria (I), and hypocitraturia (J).
CI = confidence interval.
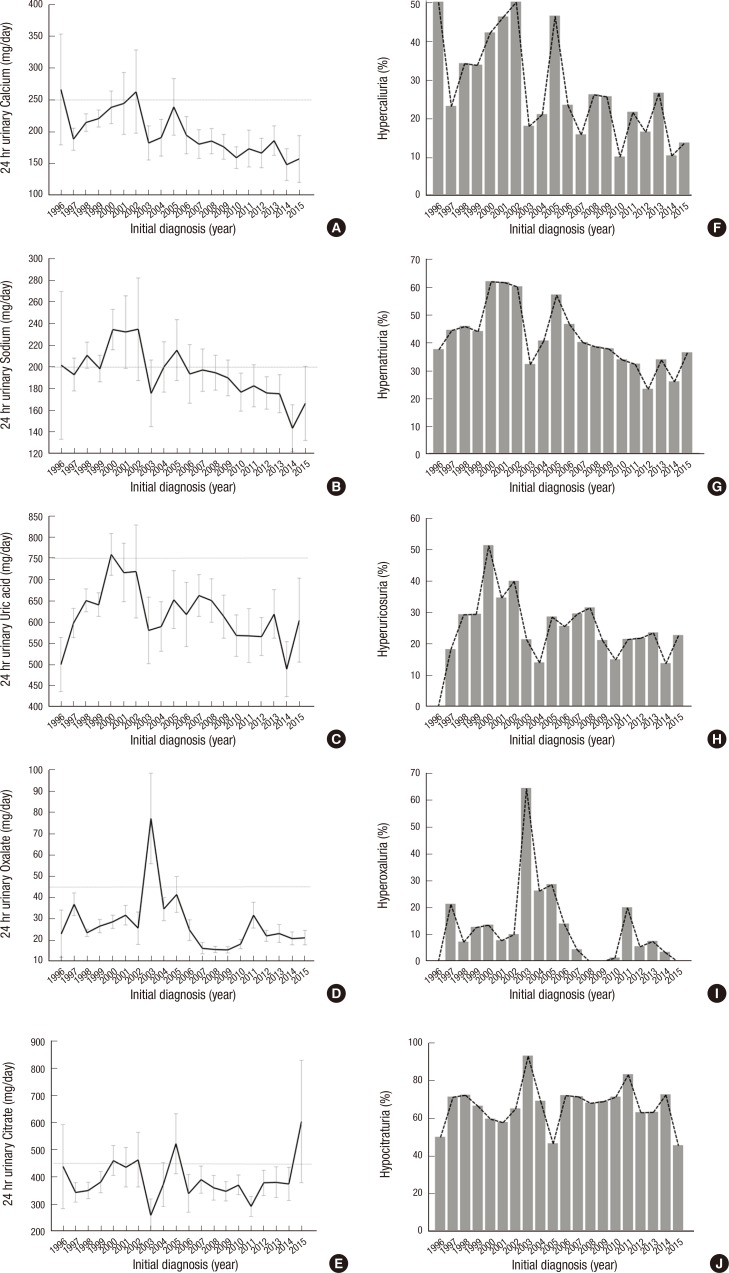
Table 2
Chronological trends in urinary metabolic features (24-hour urine constituents and 24-hour urine metabolic abnormalities) of urolithiasis patients diagnosed over 20 years
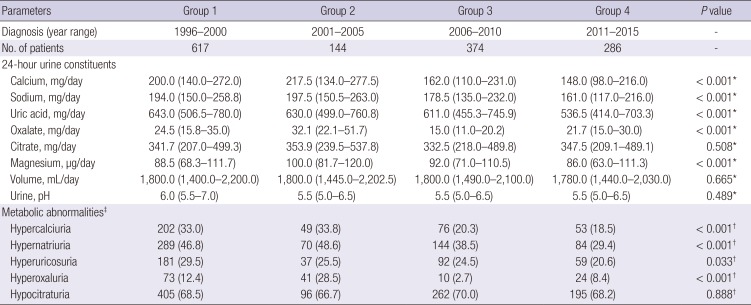
The data are shown as median (IQR) or number (%) of patients.
IQR = interquartile range.
*P values were obtained from Kruskal-Wallis tests; †P values were obtained from Fisher's exact tests; ‡Hypercalciuria was defined as excretion of ≥ 300 mg/day in men and ≥ 250 mg/day in women, hypernatriuria was defined as excretion of ≥ 200 mg/day, hyperuricosuria was defined as excretion of ≥ 800 mg in men and ≥ 750 mg in women, hyperoxaluria was defined as excretion of ≥ 45 mg/day, hypocitraturia was defined as excretion of < 450 mg/day. Analysis of 24-hour urine constituents was available for 1,421 patients (34.9% of the total cohort).
Chronological trends in stone composition over the study period of 20 years
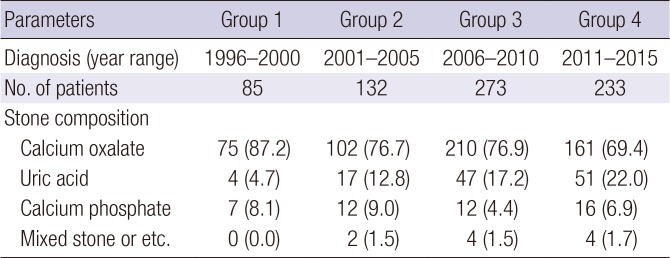
Analysis of stone composition was available for 723 patients (17.7% of the total cohort). The proportions of calcium oxalate and calcium phosphate stones decreased, whereas the proportion of uric acid stones increased with time (P = 0.015) (Table 3).
Table 3
Chronological trends of stone composition in patients with urolithiasis diagnosed over 20 years
DISCUSSION
The present study assessed the chronological trends in clinical and metabolic features in Korean urolithiasis patients over a period of 20 years. In summary, BMI and age at diagnosis increased, whereas urinary excretion of lithogenic constituents and the incidence of urinary metabolic abnormalities decreased over the study period.
The prevalence and incidence of urolithiasis has been reported to depend on the geographic locations and socioeconomic characteristics of different populations (15). The incidence of urolithiasis in Korea has progressively increased, in a manner similar to that seen in other developed countries (31617). A nationwide population-based study reported that the annual incidence of urolithiasis in Korea was 457 per 100,000 population in 2009, which was higher than that of Iran (145.1 per 100,000 population) and Japan (134.0 per 100,000 population), but lower than a range of values (from 0.5% to 1.5%) in western countries (3418). Possible explanations for rise in the prevalence of urolithiasis in Korea include improvements in diagnostic procedures in the past 20 years, thereby increasing the detection of urolithiasis so that stones are now diagnosed earlier, often at the stage of asymptomatic calculi (19). In addition, Korea has a mandatory National Health Insurance system that includes biannual health checkups, free of charge. Because this healthcare plan covers almost everyone in the country (accounting for 97% of the population), nephrolithiasis is frequently detected (20). Increasing industrialization and Westernization of lifestyles in Korea contributes to the prevalence and incidence of urinary stones. Westernization of diets and increasingly sedentary lifestyles have coincided with a rise in obesity and components of the metabolic syndrome, such as hypertension, dyslipidemia, and diabetes mellitus (721). The epidemiological link between obesity and urolithiasis has been confirmed (22). Obesity affects urinary homeostasis through changes that promote stone formation, such as reduction in urinary pH, and increases in urinary excretion of calcium and uric acid (23). The metabolic syndrome, commonly associated with obesity, results in altered renal acid-base metabolism, leading to low urine pH and a risk of uric acid stone disease (24). The age-adjusted prevalence of the metabolic syndrome in Korea has increased significantly, from 24.9% in 1998, to 29.2% in 2001, 30.4% in 2005, and 31.3% in 2007 (6). In agreement with the findings of an epidemiological study, our results showed increasing BMI and prevalence of the metabolic syndrome (indicated by hypertension and diabetes mellitus) in the past 2 decades. As a result of increasing levels of risk factors for urolithiasis, such as old age, high BMI, and the metabolic syndrome, urinary lithogenic constituents are also expected to rise. Surprisingly, our results showed the opposite trend; urinary excretion of lithogenic constituents and the incidence of urinary metabolic abnormalities decreased significantly in the past decade. Our observation that incidentally detected uric acid renal stones have become more prevalent in recent years suggests that the increasing incidence of urolithiasis in Korea might be the result of frequent health-checkup imaging rather than increasing urinary lithogenic risk. The lack of similar reports of chronological trends of urinary metabolic features in urolithiasis patients makes it difficult to definitively interpret our results. Notably, over the past 2 decades, public-health mass-media campaigns have promoted a wide variety of health behaviors, including changes in dietary habits (such as the adoption of low-salt diets, increasing consumption of fruit and vegetables, and reducing dietary fat, animal protein, and cholesterol-rich food) and lifestyle modification (including the promotion of physical activity and weight control) (7252627). Dietary modification and weight control might lead to correction of abnormal urine-metabolite levels. Another factor to consider is that stone composition seems to have changed during the study period. In our groups, the proportions of calcium oxalate and calcium phosphate stones decreased, whereas the proportion of uric acid stones increased with time. Further research is now needed to confirm our observations and to determine the causes of these changes.
Limitations of this study include its retrospective design, which may have introduced sampling bias. Another concern is that metabolic analysis and stone analysis were performed only in selected patients who were considered likely to benefit from a metabolic evaluation, and this sample would not, therefore, represent the general population. However, despite these limitations, this is one of the first studies reporting the chronological trends of urinary lithogenic risk in Korean patients with urolithiasis. Our results provide important information that can be used to establish appropriate public-health strategies for stone prevention.
In conclusion, incidentally detected uric acid renal stones have become increasingly prevalent in the past 20 years, whereas urinary excretion of lithogenic constituents and the incidence of urinary metabolic abnormalities have undergone significant reductions. Better understanding of the chronological trends of clinical and metabolic features is critical to establish appropriate public-health strategies for stone prevention.
 XML Download
XML Download