

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Zika virus (ZIKV) was first isolated in 1947 from the blood of a sentinel rhesus monkey in the Zika forest, Uganda (1). It is a flavivirus transmitted by various species of Aedes mosquito (23). The first human infection was reported in 1954 in Nigeria, and only sporadic cases of infection occurred in Southeast Asia and sub-Saharan Africa until the outbreak of 2007 on Yap Island, the Micronesia (456). In October 2013, another outbreak started in French Polynesia in the South Pacific where Guillain-Barré syndrome occurring immediately after the viral infection was seen for the first time (78). The outbreak of ZIKV is ongoing since March 2015 and it started in Camaçari, Bahia, Brazil (9). Cases of microcephaly have been increasingly reported in association with viral infection in ZIKV-affected areas (10). Accordingly, on February 1, 2016, the World Health Organization (WHO) declared a Public Health Emergency of International Concern. As of December 15, 2016, 58 countries have experienced the outbreak from 2015 onwards, 13 countries have reported evidence of person-to-person transmission and 29 countries or territories have reported microcephaly and other central nervous system malformations potentially associated with ZIKV, or suggestive of congenital infection (11).
The first case of ZIKV infection in Korea was reported in March 2016 (12). By October 2016, 14 patients had been reported; all of the affected patients had visited areas with ZIKV. The aim of this study was to identify the epidemiological and clinical characteristics of ZIKV infection imported into Korea.
MATERIALS AND METHODS
Patients who had visited risk areas in the 2 weeks before the onset of symptoms and tested positive for ZIKV reverse transcriptase polymerase chain reaction (RT-PCR) in blood, urine, or saliva specimens were included. Risk areas were identified from the Zika situation report of the WHO (11).
Epidemiological evaluations, routine checks for symptoms, and physical examinations were carried out on these patients along with complete blood counts, liver function tests, blood urea nitrogen (BUN)/creatinine measurements and urinalysis. Blood, urine, and saliva samples were collected for the ZIKV RT-PCR; semen samples were collected from male patients. ZIKV RT-PCR of blood, urine, and saliva samples were performed once weekly until the results were negative. After that, the RT-PCR were performed once more a week later. The RT-PCR of semen samples were performed at initial presentation, and 8 weeks after the onset. The RT-PCR was carried out using a commercial kit, the genesig ZIKV polyprotein standard kit (PrimerDesign Ltd., Southhampton, UK), as well as in-house RT-PCR reported by Lanciotti et al. (13).
RESULTS
From March to October 2016, 14 patients with ZIKV infections were reported in Korea; 11 were male and 3 were female. The median age was 34 years (19–64 years) and most of the patients were in their thirties or forties (Table 1). Ten patients had been exposed in Southeast Asia (5 in the Philippines, 3 in Vietnam, 2 in Thailand) and 4 in Latin America (1 each in Brazil, Dominican Republic, Guatemala, and Puerto Rico); 12 had been temporary visitors and 2 were long-term residents (in the Dominican Republic and Guatemala). Nine of the patients recalled being bitten by mosquitos. The incubation period was estimated to be 0 to 27 days (Table 1). A total of 14 persons were in company with patients and one of them was confirmed to be infected with ZIKV despite being asymptomatic (case 3, Table 1).
Table 1
Epidemiologic findings of patients infected with ZIKV in 2016

Rash occurred in 13 patients (92.9%; 13/14, Table 2), and its median duration was 3 days (2–8 days). It appeared as erythematous eruptions and was distributed over face, trunk, back, upper and lower extremities, and palms (Fig. 1). Myalgia was seen in 7 patients (50.0%), arthralgia in 4 (28.6%), and 3 (21.4%) presented with fever. Conjunctivitis appeared in 2 patients (14.3%), and headache in 1 (7.1%) patient. One patient was asymptomatic. No patients had neurological symptoms and none were pregnant. Blood tests showed no abnormalities in leukocytes, red blood cells, and platelet counts and liver enzyme levels. Urinalysis also revealed normal findings.
Table 2
Clinical manifestations of patients infected with ZIKV (+: positive, −: negative)
Fig. 1
Erythematous rash of ZIKV infection. (A) Rash found on the trunk. (B) Rash found on left arm.
ZIKV = Zika virus.

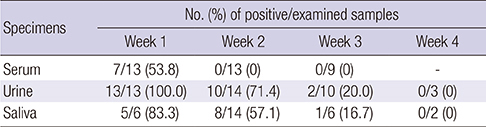
RT-PCR positivity rates in serum, urine, and saliva were 53.8% (7 out of 13), 100.0% (13 out of 13) and 83.3% (5 out of 6) in the first week of symptoms, respectively (Table 3). In the second week, the positivity rate for RT-PCR in serum fell to zero, while the rates for urine and saliva were 71.4% (10 out of 14) and 57.1% (8 out of 14), respectively. Positivity rates for urine and saliva dropped to 20.0% (2 out of 10) and 16.7% (1 out of 6), respectively, by the third week of symptoms. In the case of semen, 100.0% (4 out of 4) of the patients were positive in the first week and 80.0% (4 out of 5) in the second week. One out of 2 patients tested in their 9th week showed positive result.
Table 3
Positivity rates of RT-PCR for ZIKV in the serum, urine, and saliva of patients
DISCUSSION
A total of 14 patients with ZIKV infections were reported from March to October 2016 in Korea; 10 patients were exposed to the virus in Southeast Asia and 4 in Latin America. All symptomatic patients showed mild degree of illness and there were no neurologic abnormalities. None of the patients was pregnant. All but 1 patient suffered from rash, which was distributed over the face, trunk, upper and lower extremities, and palms. Findings of blood and urine tests were normal. RT-PCR tests of serum samples were positive only in the 1st week after symptom onset, but they were positive in urine and saliva until the 3rd week. In the semen specimen RT-PCR was positive up to the 9th week.
It has been reported that the majority of the patients with ZIKV infection are asymptomatic and clinical presentations of symptomatic patients are mild and self-limiting (14). The most common clinical features of ZIKV infection are rash, myalgia, arthralgia, fever, fatigue, and conjunctivitis. Although clinical presentations are mild, ZIKV infection has become a public health concern now because it can cause complications including congenital microcephaly and Guillain-Barré syndrome (715). ZIKV transmitted mostly via the bite of infected mosquito. Few cases of person to person sexual transmission have been reported and ZIKV RNA has been detected in semen of infected male. In this study ZIKV RNA was detected in 1 male patient 9 weeks after the onset of symptoms. ZIKV infection should be suspected in clinically compatible patients without travel history, because ZIKV could be transmitted via sexual intercourse with infected partners.
In Asia, ZIKV was first isolated from Aedes aegypti in Malaysia in 1966 and the first human infection was reported in 1977 in Indonesia (3). Until 2013, sporadic isolation was reported among residents in, and travelers to, Southeast Asia, but no definite outbreak occurred (5). Two cases of ZIKV infection imported from French Polynesia were reported in Japan in 2014, and, following the declaration of a ZIKV pandemic in 2016, ZIKV cases were reported in numerous Asian countries such as Taiwan, Indonesia, China, and Vietnam (16). There are 2 major lineages of ZIKV, African and Asian, which were identified by phylogenetic analyses (217). The strain which provoked epidemics on Yap Island of the Micronesia and in South America is classified in the Asian lineage (14). On August 27, 2016, the first local transmission of ZIKV in Singapore was identified and the strain appeared later to be of Asian lineage and distinct from that circulating in the Americas (18). In September 2016, the first Asian case of Zika-linked microcephaly was confirmed in Thailand (11).
ZIKV was first isolated from Aedes africanus in 1948, but Aedes aegypti is the major vector for the virus in Asia and South America (21920). There has been a longstanding suspicion that Aedes albopictus, an important vector for chikungunya fever, might be a vector as well, and the first ZIKV detection in Aedes albopictus was reported in 2014 (19). Since Aedes albopictus is the species found in Korea, concerns about the influx of, and colonization by, ZIKV have been raised (2122). Although the competence of Aedes albopictus to transmit ZIKV has been reported to be much lower than that of Aedes aegypti, the possibility of ZIKV colonization in Korea needs to be closely monitored (232425).
In conclusion, 14 patients with ZIKV infection were reported in Korea by October 2016 and all the patients had mild or no clinical symptoms.
 XML Download
XML Download