

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
It is estimated that, worldwide, half a billion new controllable sexually transmitted infections (STIs) such as syphilis, chlamydia, and gonorrhoea occur annually, with the highest rates observed among young persons aged 20–24 years, followed by those aged 15–19 years (12). Adolescents are potentially at greater risk of STIs as they tend to have multiple sex partners and engage in unprotected intercourse using condoms inconsistently because of delayed or inadequate sex education (34). STIs can lead to serious health problems including ectopic pregnancy, pelvic inflammatory disease, infertility, congenital infection, and cervical carcinoma (15). Most infected adolescents do not seek treatment due to financial and time constraints (16). Thus, adolescents are more vulnerable to the complications of STIs; this can affect public health.
Adolescents who attend correctional facilities tend to engage in risky sexual behaviours and do not readily engage with medical services (789). The United States' Centers for Disease Control and Prevention (CDC) estimated that the prevalence of chlamydial infection was 15.7% among female adolescents and 7.4% among male adolescents in juvenile correctional facilities in 2011 (10), markedly higher than the prevalence of 1.8% in the general population of adolescents reported in 2014 (11); adolescents in correctional facilities are at a higher risk of STIs. Currently, there is one reported prevalence survey of STIs targeting adolescents under probation in correction facilities in Korea. That survey, conducted by Lee et al. (12) in 2004, reported that the prevalence of Chlamydia trachomatis among adolescents attending youth shelters was 12.6%. Thus, the prevalence among adolescents at higher risk in Korea was similar to that reported in the United States. However, there is no screening system for and no recent prevalence data on STIs in Korea.
As most STIs may be asymptomatic, it is important to screen for and prevent them (6). Prevalence surveys are essential for the establishment of screening and preventive strategies. Therefore, we examined the prevalence of STIs involving the following causative pathogens: C. trachomatis, Neisseria gonorrhoeae, herpes simplex virus (HSV), Treponema pallidum, human immunodeficiency virus (HIV), and Trichomonas vaginalis among Korean adolescents under probation. Some studies have suggested that mycoplasma and ureaplasma can contribute to genitourinary infection and infertility (131415161718). However, studies have only investigated the prevalence of Mycoplasma genitalium in adolescents (1920). Therefore, we investigated the prevalence of Mycoplasma hominis, M. genitalium, Ureaplasma parvum, and Ureaplasma urealyticum. This study also examined current sexual behaviours, circumstances, and socioeconomic factors related to STIs.
MATERIALS AND METHODS
Study design and participants
We conducted a prospective, cross-sectional study among adolescents aged ≤ 19 years who were under probation in two cities in Korea. One juvenile-delinquent centre protecting male adolescents and five probation offices participated. The study took place from April to November 2014.
Data collection
An anonymous, self-administered, structured questionnaire prepared in Korean was used to collect data on the socioeconomic status of participants (age, residence type, economic status, and weekly allowance), behavioural factors (smoking, alcohol use, hallucinogen use, and runaway experience), sexual practices (age of sexual debut, condom use, number of sex partners over the preceding 3 months, and date of most recent sexual intercourse), and history of STIs. Weekly allowance was converted into United States dollar (USD) at the exchange rate of May 2, 2017. To evaluate sexual knowledge, 45 questions were included in the questionnaire regarding safe sex and STIs. The questionnaire about sexual knowledge was administered in combination with a previously published sexually transmitted disease knowledge questionnaire (STD-KQ) and a Korean sex knowledge questionnaire developed for adults (21). The STD-KQ was translated into Korean and the questionnaire was distributed to all subjects. Correct answers were scored as 1 and “do not know” or incorrect answers were scored as 0. The total score was calculated by adding the scores for all questions.
Urine specimens (50 mL of the first void) were collected in sterile screw-cap plastic bottles, and serum samples (10 mL) were obtained. A code number linked the urine and serum specimens to the questionnaire. All results were reported to participants. All participants who received positive results requested treatment.
Laboratory tests and methods
The urine specimens were analysed to detect the presence of C. trachomatis, N. gonorrhoeae, T. vaginalis, M. hominis, M. genitalium, U. urealyticum, and U. parvum by nucleic acid amplification tests using multiplex real-time polymerase chain reaction (PCR) (Anyplex™ II; Seegene, Seoul, Korea). Multiplex real-time PCR showed sensitivity as 100% for C. trachomatis, N. gonorrhoeae, T. vaginalis, M. genitalium, and M. hominis and 97.8% for U. urealyticum. Specificity of that was as follows: 100% for C. trachomatis and M. genitalium, 99.9% for T. vaginalis, 99.3% for M. hominis and U. urealyticum and 99.2% for N. gonorrhoeae (22). PCR was performed using a real-time PCR instrument (CFX96 Real-time PCR System; Bio-Rad, Hercules, CA, USA) according to the manufacturer's instructions, as follows: 1) primary denaturation at 95°C for 15 minutes; 2) 50 cycles of denaturation at 95°C for 30 seconds, annealing at 60°C for 1 minutes and extension at 72°C for 30 seconds; and 3) final cooling down at 55°C for 30 seconds. The results were analysed using Seegene software, which interpreted results as positive or negative. Positive results were confirmed by single PCR using the Seeplex STD kit (Seegene).
The 10 mL serum samples were used for rapid plasma reagin (RPR) testing for syphilis, HSV-1 and HSV-2 immunoglobulin (Ig) G, and HIV antigen/antibody combination testing. Samples were tested by the Department of Laboratory Medicine in Hallym University Kangnam Sacred Heart Hospital. Syphilis was diagnosed based on RPR performed by latex suspension (Hitachi, Tokyo, Japan). Mediace RPR ≥ 1.0 RU was considered positive. HIV antibodies were detected by the chemiluminescent micro-particle immunoassay (Abbott Architect i2000SR; Abbott Laboratories, Chicago, IL, USA) and positive results were confirmed by western blot. HSV IgG was tested by chemiluminescent immunoassay (DiaSorin Inc., Stillwater, MN, USA) entrusted to Green Cross Laboratories, Korea.
Statistical analysis
The prevalence of STIs was calculated using positive rates, computed as the total number of positive tests divided by the total number of subjects tested. The association between STI positivity and risk factors was assessed using χ2 tests. If the expected frequency was < 5% for ≥ 20% of categories, Fisher's exact test was performed. Risk factors were examined in sex-experienced subjects. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Variables with a P value < 0.3 were included in a multivariate logistic regression model. In the model, a P value of < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS software, version 20 (IBM SPSS Inc., Armonk, NY, USA).
RESULTS
A total of 237 adolescents (208 male and 29 female adolescents) were enrolled. The mean age of participants was 16.1 ± 1.5 years (range, 12–19 years) (Table 1). Overall, 223 (94.1%) participants lived with their parents and eight (3.4%) lived in a day-care center. Most participants (32.1%, n = 76) received a weekly allowance of 10,000–30,000 won (8.8–26.5 USD); followed by those receiving > 50,000 won (44.2 USD) (26.2%, n = 62) and < 10,000 won (8.8 USD) (22.8%, n = 54). Overall, 186 (78.5%) adolescents reported having drunk alcohol, 211 (89.0%) had experienced smoking, and 104 (43.9%) had dropped out of school. Twenty participants (8.4%) had used hallucinogens and 27 (11.4%) had experienced running away from home. Despite the fact that almost 60% (n = 142) of participants had received sex education, the average sexual knowledge score was 11.0 ± 7.7 points on a 45-point scale. A total of 152 (64.1%) participants had a history of coitus. Of these, 103 had had sexual intercourse within the preceding 6 months, representing 67.8% of sex-experienced subjects (Table 2). Most adolescents (55.3%, n = 84) reported an age of sexual debut between 15 and 16 years. The majority (75.7%, n = 115) of participants had had a single sex partner over the preceding 3 months, although 24.3% (n = 37) had had multiple sex partners. Only 27.6% (n = 42) always used a condom during sexual intercourse; 16.4% (n = 25) never used a condom. There was no homosexual. Twenty-six (17.1%) participants gave a history of having had a STI.
Table 1
Baseline characteristics of enrolled adolescents (n = 237)

Table 2
Sexual practices in sex-experienced adolescents (n = 152)

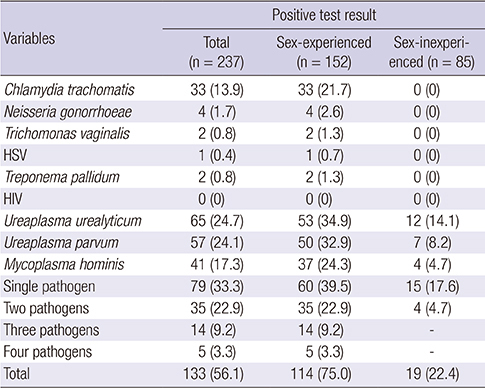
In total, 133 (56.1%) participants had at least one of the microorganisms tested for detected in their genitourinary tracts (Table 3). The most prevalent STI pathogen was U. urealyticum (24.7%, n = 65), followed by U. parvum (24.1%, n = 57), M. hominis (17.3%, n = 41), and C. trachomatis (13.9%, n = 33). There were four cases (1.7%) of N. gonorrhoeae but no reported cases of HIV. The prevalence of T. vaginalis and HSV was 0.8% (n = 2) and 0.4% (n = 1), respectively. Two participants (0.8%) tested positive for Treponema pallium. At least one pathogen was detected in the 114 (75.0%) participants who were sex-experienced. U. urealyticum was found in 53 (34.9%) of these participants' specimens, followed by U. parvum (32.9%, n = 50) and M. hominis (24.3%, n = 37). The total number of participants who had more than two pathogens was 54 (35.5%). Among these participants, 35 (22.9%) and 14 (9.2%) tested positive for two different pathogens and three pathogens simultaneously. Five participants (3.3%) had four different pathogens. Table 4 showed the distribution of microorganism positive with multiple pathogens. Among the sex-inexperienced participants, 19 tested positive for at least one pathogen: 12 (14.1%) were positive for U. urealyticum, seven (8.2%) for U. parvum, and four (4.7%) for M. hominis. There were no cases of C. trachomatis, N. gonorrhoeae, T. vaginalis, HIV, HSV, syphilis, and M. genitalium among sex-inexperienced subjects. Four participants (4.7%) were positive with two pathogens simultaneously. Three (3.5%) were positive with M. hominis and U. urealyticum and one (1.2%) was U. parvum and U. urealyticum.
Table 3
Distribution of microorganism detection according to sex experience
Table 4
Distribution of microorganism in positivity with multiple pathogens in sex-experienced adolescents (n = 54)

Factors associated with STIs in sex-experienced adolescents are shown in Table 5. In the univariate analysis, only STI history differed significantly between those with a STI relative to those without (OR, 4.5; 95% CI, 1.02–20.30; P = 0.032). We did not find any statistically significant differences in the variables relating to sexual practices, such as age of sexual debut, number of sexual partners in the preceding 3 months, and condom use during sexual intercourse. Previous sex education experience and sex knowledge scores were not significantly associated with the presence of an STI. No significant difference was found according to other socioeconomic and behavioural factors such as residence type, runaway history, smoking, alcohol use, hallucinogen use, and history of having dropped out of school. On multivariate analysis, we found no significant independent variable associated with the presence of microorganisms causing STIs. We also evaluated factors in participants that tested positive according to multiple pathogens and single pathogen (Table 6). In the univariate analysis, we did not find any statistically significant differences in the variables relating to sexual practices, other socioeconomic and behavioural factors.
Table 5
Associations between variables and STIs in sex-experienced adolescents
Values are presented as number (%).
CI = confidence interval, STI = sexually transmitted infection, OR = odds ratio, aOR = adjusted odds ratio, USD = United States dollar, Ref = reference category.
*Chi-square tests and Fisher's exact test. †Logistic regression model adjusted for dropped out of school, aged < 16 years at sexual debut and STI history.
Table 6
Associations between variables and multiple infection in STI positive adolescents (n = 114)
DISCUSSION
Currently, the only available data on the prevalence of STIs among adolescents under probation in Korea comes from a single prevalence survey conducted in 2004 among homeless adolescents attending a shelter (12). That study reported that 54.9% of adolescents had engaged in sexual intercourse and that 36.5% were younger than 16 years old at sexual debut. In our study, 152 (64.1%) participants had experienced sexual intercourse, and half of them had experienced their first sexual intercourse aged younger than 16 years. Sexual intercourse experience was comparable to the 2004 study of homeless adolescents, but the proportion of adolescents reporting an earlier sexual debut was higher in the present study. A Korean study involving general middle and high school students revealed that approximately 4.2% adolescents had experienced sexual intercourse from 2007 to 2013 (23). Compared with the general population, a greater proportion of adolescents under probation had engaged in sex.
In the 2004 study, the prevalence of C. trachomatis and N. gonorrhoeae was 12.6% and 15.4%, respectively (12). Based on a self-administered questionnaire, experience of any previous STI was 7.4% among boys and 7.5% among girls attending general middle or high school during 2007 to 2013 (23). In the present study, the prevalence of C. trachomatis and N. gonorrhoeae was 13.9% and 1.7%, respectively. Compared with the 2004 study on adolescents attending a shelter, the prevalence of C. trachomatis in the present study was similar while the prevalence of N. gonorrhoeae was lower. The prevalence of STIs in adolescents under probation is considerably higher than in the general population.
In the United States, the CDC estimated that the prevalence of C. trachomatis among female and male adolescents in juvenile correctional facilities was 15.7% and 7.4%, respectively, in 2011 (10), and the prevalence of N. gonorrhoeae was 1.2% and 4.4% among male and female adolescents, respectively. The prevalence of C. trachomatis and N. gonorrhoeae in our study was similar to that reported in the United States. The CDC recommends the screening of all sexually active women younger than 25 years for C. trachomatis and N. gonorrhoeae. Despite the high prevalence of STIs among adolescents under probation, there is no screening system for STIs targeting adolescents under probation in Korea. Although up to 80% of women and 50% of men infected with C. trachomatis are asymptomatic or have few symptoms, these infections can result in long-term sequelae, such as infertility and cervical cancer (124). Diagnosis by means of a screening process is essential. Considering the high prevalence of STIs among adolescents under probation, it is advisable to screen such adolescents for STIs when they are admitted to correctional facilities.
Some studies have suggested that mycoplasma and ureaplasma can contribute to the development of genitourinary infection and infertility (13141518). Despite studies on potential STI causative pathogens, there are no established guidelines on when to use diagnostic tools and when to treat mycoplasma and ureaplasma. Furthermore, few prevalence surveys of mycoplasma and ureaplasma have been conducted among adolescents and no prevalence studies of adolescents under probation have been performed to date. To our knowledge, this is the first study researching the prevalence of STIs, including infection with mycoplasma and ureaplasma, in adolescents under probation. In this study, the prevalence of M. hominis, M. genitalium, U. urealyticum, and U. parvum was 17.3%, 4.2%, 27.4%, and 24.1%, respectively. There is no comparable study targeting the general adolescent population in Korea. However, according to a study involving female adolescents aged 14–21 years in the United States, the prevalence of M. genitalium was 22.4% (19). A Korean study involving asymptomatic adults attending a clinic for a checkup found that the prevalence of M. genitalium was 1.0% and the prevalence of U. urealyticum was 11.8% (25). In a comparable study targeting asymptomatic Korean adults, the prevalence of M. hominis, M. genitalium, and U. urealyticum was 11.6%, 0.3%, and 22.1%, respectively (26). Compared with studies conducted abroad, the prevalence of M. genitalium among Korean adolescents under probation was lower; however, compared to asymptomatic adults in Korea, the prevalence was higher. Interestingly, 22.4% of adolescents who had not experienced sexual intercourse also tested positive for mycoplasma and ureaplasma. It is possible that adolescents under probation tend to hide their sexual intercourse experience due to Korean culture which considers sexuality among adolescents as taboo. It is also possible that mycoplasma and ureaplasma, considered causative pathogens for STIs, can colonize the genital tract at birth (following passage through the maternal vaginal tract). Therefore, it is difficult to decide when to consider the organisms as true pathogens and, thus, to decide when or whether to commence treatment. We must be cautious of treating all adolescents who test positive for mycoplasma or ureaplasma. It may be appropriate to use a diagnostic tool to detect mycoplasma or ureaplasma and to commence treatment if there is no clinical improvement following treatment for common pathogens. However, further studies investigating the timing of investigating and treating these pathogens are needed.
We found no association between the variables investigated in this study and STI positivity. The distribution of variables considered to be risk factors for STIs, such as residence type, weekly allowance, having run away from home, alcohol use, smoking, and having dropped out of school (2728), were similar in both groups. As we compared risk factors within a population of adolescents under probation, who by definition engage in higher-risk habits and live in riskier circumstances than the average adolescent, we could not identify any meaningful risk factors in this study. The sexual knowledge score was not significantly different. Furthermore, the sexual knowledge score was very low, despite > 60% of adolescents having received sex education. According to the middle school education regulations, it is mandatory to provide at least 15 hours of sex education per year. However, in practice, this class is substituted for personal study time. Also, it is doubtful that adolescents under probation are focused on education. Providing sex education in correctional facilities may be an effective strategy, but it is important to improve the content of sex education programmes. Surprisingly, > 20% of the adolescents who reported that they always used condoms during sexual intercourse tested positive for at least one examined STI pathogen. Although adolescents under probation reported that they knew how to use condoms correctly, our results suggest that their knowledge was inadequate. A more practical approach is warranted, including information on the use of contraceptive devices, methods to prevent STIs, and the symptoms of STIs.
There is also gap between theoretical knowledge and the practical application thereof. In Korea, it is difficult for adolescents to obtain contraceptives such as condoms. According to the Korean Youth Protection Act, there is no restriction on purchasing condoms and it is possible to buy them at convenience stores or pharmacies. However, in practice, many adolescents cannot purchase condoms because of sales refusal and the surrounding attention received. Contraceptives should be accessible to adolescents in environments such as schools or public health centres. In addition, it is difficult for adolescents to make use of medical institutions specializing in STIs for cultural reasons. Despite recognizing the symptoms of an STI, adolescents are likely to miss the appropriate timing for treatment. There is a need to establish medical services that are free for adolescents and that are able to provide accurate information and treatment for STIs. Because the prevention and treatment of STIs in adolescents is crucial, it is important to understand adolescent sexuality and behaviour and to publicize activities to raise awareness of STIs.
Our study has some limitations. First, we included only 29 (12.2%) female adolescents. However, according to the 2014 Crime Prevention Policy Bureau statistics, of the 140,572 adolescents under probation, 124,385 (88.5%) were male and 16,187 (11.5%) were female (29). This male-to-female ratio coincides with the ratio in our study. Second, sexual intercourse experience might be underestimated because most adolescents avoid making their experience known due to social attention. Third, we could not collect data about the reason for entering the probation office. It might act as a risk factor according to some crime types such as sex crime but it was not investigated. Finally, we included probation offices and juvenile delinquent centres in only two metropolitan areas in Korea. Hence, our findings cannot reflect the general Korean regional characteristics. Thus, further surveys that include all regional Korean adolescents under probation should be performed.
In conclusion, the prevalence of STIs among adolescents under probation is high, and adolescents are currently exposed to more STI risks than they were in the past. More systematic screening policies, use of more practical sex education, and the provision of appropriate treatment for STIs are essential for the prevention and management of STIs in adolescents, particularly among those at risk. Furthermore, increased societal focus on adolescents is important.
 XML Download
XML Download