

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Out-of-hospital cardiac arrests (OHCAs) are a major problem that has become a global health burden. The global average incidence of emergency medical services (EMSs)-assessed OHCA is 55 adults per 100,000 person-years. The incidence varies among continents, from 52.5 for Asia to 112.9 for Australia (1). OHCAs of non-cardiac etiology vary in their epidemiologic features, with different incidence rates and outcomes (234).
One of the major non-cardiac etiologies of OHCAs is poisoning. An Asian country reported an incidence of OHCAs with non-cardiac origin of 28% (10.58 per 100,000 person-years). Of these, cases caused by intoxication represented 6.7%. The survival to discharge rate for OHCAs with a poisoning etiology was approximately 2.7%, which is lower than that of other etiologies, such as asphyxia (8.5%) and drowning (2.9%) (5). In other countries, the incidence of poisoning-induced out-of-hospital cardiac arrest (P-OHCA) varies from 1.8% in Sweden to 3.1% in Finland (678). Based on many case reports, some of these poisoning cases occurred by chance, and some were intended to induce OHCA as a form of suicide (9).
P-OHCAs may be preventable through primary prevention interventions. To avoid fatal exposures to poison or to prevent suicide by drugs, the causative agents should be identified and tested for their associations with patient outcomes. Previous studies have found that the causative agents of P-OHCA were associated with the survival to admission and survival to discharge rates (10). However, in many cases, the causative agent was unknown (34.6%) or the classification of the agents was insufficient, which can lead to difficulty making decisions regarding an emergency antidote. Antidote therapy and gastrointestinal decontamination that are targeted to a specific agent will save more lives in cases of P-OHCA (111213).
It is unclear whether specific agent groups are associated with outcomes in P-OHCA. The study aimed to classify poisons into specific agent groups and to compare the outcomes for these groups.
MATERIALS AND METHODS
Study setting
Most OHCA patients are transported by single-tiered, government-based public EMS programs from the sixteen provincial headquarters of the national fire department (14). The Korean EMS is available 24 hours a day, 365 days a year, and provides a basic to intermediate level of ambulance services to approximately 50 million people residing in an area of approximately 100,000 km2. There were approximately 1,400 ambulance stations throughout the nation in 2010 (15). In the case of a patient with P-OHCA, ambulance crews administer cardiopulmonary resuscitation (CPR) at the scene and during transport with automatic external defibrillation. The resuscitation should be continued until the declaration of death by a physician (16). Grade 1 emergency medical technicians can offer advanced airway techniques, including airway insertion, endotracheal intubation and laryngeal mask airway insertion. They also can access a venous line and provide 0.9% normal saline solution under direct medical control. However, medications for advanced cardiac life support are usually not available (17). Antidote therapy and gastric lavage, which are necessary specifically for poisoned patients, cannot be provided in the pre-hospital stage. Ambulance crews collect information about the causative agent and the time/amount/route of intake at the scene and inform the emergency medicine (EM) physicians.
All emergency departments (EDs) are formally designated as level 1 to 4 by the government based on their available human resources, essential instruments, equipment, and service level, such as the availability of certain specialists. Level 1 (n = 20) and level 2 (n = 110) EDs have more resources and better facilities for emergency care and must be staffed by emergency physicians 24 hours a day, 365 days a year, by law. Level 3 EDs (n = 330) are basically equipped and can be staffed by general physicians. Level 4 denotes a non-ED facility. The status of all EDs is evaluated annually by an audit committee under the EMS Act (18).
At the hospital, primary stabilization of the patient is provided, followed by a determination of the causative agent, and antidote therapy is administered as soon as possible; decontamination, hemofiltration, and hemodialysis follow. As the protocol is not standardized, the physicians follow individual hospital-based protocols. Post-return of spontaneous circulation (ROSC) care, such as mild therapeutic hypothermia, and active cardiac care, including percutaneous coronary intervention, coronary artery bypass surgery and the insertion of an implantable cardioverter-defibrillator/pacemaker, are provided according to the hospital's protocols.
Data source
A national OHCA registry database was constructed in two steps based on databases from the Fire and Disaster Headquarters and the Korea Centers for Disease Control and Prevention (CDC). First, the national registry was generated based on a primary EMS database on OHCA from the Fire and Disaster Headquarters, which collects data from ambulance run sheets and the cardiac arrest registries completed by ambulance crews. Most of the Utstein factors, such as bystander CPR, witnessed condition, place, region, and elapsed time intervals were collected from the EMS database. Values were fully recorded by the EMTs except for a few factors, such as public versus private location (17% unknown). The EMS variables were not cleaned by the quality management committee (QMC).
This step was followed with the addition of information from medical record reviewers from the Korea CDC regarding the hospital outcomes, patient comorbidities, and hospital care procedures. This additional information was based on the medical records of approximately 700 hospitals, to which the OHCA patients were transported by ambulance. Medical records in this study setting are very critical for national health insurance claims. All diagnosis codes (using the International Classification of Disease, 10th version [ICD-10]) and all procedure codes (using the International Classification of Disease, 9th version [ICD-9] clinical modification) must be recorded in discharge summary for reimbursement purposes. Most hospitals submit claim data to the national insurance authority for reimbursement. The duty physicians' records provide the basis for the electronic submission by hospitals. Therefore, the medical record review sources are relatively clear. In particular, the insurance program provides special discounts for rare diseases, including sudden cardiac arrest. This discount is very important for patients. The records are usually clear for these reasons.
Medical record reviewers were educated and trained using the medical record review guidelines prior to joining the project, and a data QMC worked to maintain the data quality. The QMC provided monthly meetings to obtain feedback on the quality of the data obtained by the medical record reviewers. The QMC has two roles regarding data quality. The first role is to test internal reliability by comparing the descriptive statistics of each reviewer's cases. If an outlier was found in the comparison, the QMC reviewed the cases that were reviewed by that reviewer. The second role is to provide advice for unclear cases. For example, a case with a hopeless discharge might be discussed in terms of neurological recovery. The QMC reviewed the cases and provided the level of neurological recovery based on the clinical information provided in the record. When reviewers were uncertain about the exact coding during their work, they could consult a person in charge in the QMC in real time. The QMC consists of statistical experts, epidemiologists, a cardiologist, EM specialists, and medical record review experts (18).
Study population
In this study, EMS-treated patients of all ages with OHCA due to confirmed or presumed poisoning from 2008 to 2013 throughout the country were included. A case was defined as having a confirmed or an undetermined causative agent of poisoning, as recorded on the medical record review by the clinician. Poison agents were classified according to the ICD-10. Cases involving patients with an unknown final outcome or who were not treated by the EMS and ED were excluded.
Main exposure
In this study, poisoning included both chemical poisoning and drug intoxication. Chemical poisoning includes intentional or unintentional intoxication by agents that are not normally consumed: carbon monoxide, toxic gas, industrial alcohol (methyl alcohol), ethylene glycol (antifreeze), pesticides, etc. Drug intoxication includes intentional or unintentional poisoning by prescribed medicines, drugs or alcohol. The etiology of the poisoning as an exposure variable was further categorized into the following groups according to the ICD-10: X40 X60 Y10 (non-opioid analgesics, antipyretics, and antirheumatics), X41 X61 Y11 (antiepileptic sedative-hypnotic, anti-Parkinsonism, and psychotropic drugs), X42 X62 Y12 (narcotics and psychodysleptics [hallucinogens]), X43 X63 Y13 (drugs primarily affecting the autonomic nervous system), X44 X64 Y14 (other and unspecified drugs, medications and biological substances), X47 X67 Y17 (other gases and vapors), X48 X68 Y18 (pesticides), X45 X65 Y15 (alcohol), X46 X66 Y16 (organic solvents and halogenated hydrocarbons and their vapors), and X49 X69 Y19 (other and unspecified chemicals and noxious substances) (Available at http://apps.who.int/classifications/icd10/browse/2016/en#). As there were too few cases in some of the causative agent categories to analyze, we re-categorized them into five groups: group 1 (medically prescribed drugs; X10–X14, X40–44, Y10–Y14), group 2 (vapors or gases; X17, X47, Y17), group 3 (pesticides; X18, X48, Y18), group 4 (alcohol or organic solvents; X15–X16, X45–X46, Y15–Y16), and group 5 (other unspecified; X19, X49, Y19).
Variables
Additional variables included age, gender, witness (yes or no), region (rural/urban vs. metropolis), place of the event (public, private, or unknown), bystander CPR (yes or no), prehospital defibrillation (yes or no), initial electrocardiogram (ECG) (ventricular fibrillation/ventricular tachycardia, pulseless electrical activity, asystole, and unknown), response time from call to ambulance to arrival at the scene, scene time from arrival at scene to departure to the ED, transport time from departure of scene to arrival at the ED, level of ED (level 1, level 2, level 3, and level 4 classifications), and prehospital ROSC (yes or no).
Outcome measurement
The primary outcome measure was survival to discharge. Survival to discharge was defined when a patient was normally discharged or transferred to another facility, such as a rehabilitation center. We considered a case as a survival to discharge when it was described in a discharge summary or in other documentation. Discharge summaries and other documents were drafted by inpatient physicians and reviewed for greater validity by the hospital medical record review team, as these documents are usually used for national health insurance claims data after discharge. The secondary outcome measure was the patient's cerebral performance outcome. All patients with survival to discharge were classified using the cerebral performance categories (CPCs) of 1 (good recovery), 2 (moderate disability), 3 (severe disability), 4 (coma or vegetative state), and 5 (brain death). A good neurological status was defined as a CPC score of 1 or 2. Medical record reviewers from the Korean CDC categorized and coded this outcome under the supervision of the project QMC, and codes were decided via on- and off-line consultation when the CPC category of the case was controversial. The outcome measures were determined by the same record reviewer who performed the review for poison source code.
Statistical analysis
The demographic characteristics of the poisoning agent groups were compared using χ2 tests for categorical variables. We compared the clinical outcomes according to clinical process (did not survive to ED, survived to ED but died in the ED, survived to admission but died on the ward, survived to discharge with bad CPC, and survived to discharge with good CPC) by poison group.
We developed a multivariable logistic regression analysis model to test the association between causative agents and hospital outcomes while adjusting for confounding factors known to be associated with the outcomes. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated. The elements with a significant difference were selected and included in the multivariable model. P values were based on a two-sided significance level of 0.05. The final confounding factors included age, gender, region, location, bystander CPR, witness status, initial cardiac rhythm, time interval from the call to EMS to the arrival on the scene (response time interval), time interval from the arrival on the scene to departure to the ED (scene time interval), and time interval from departure from the scene and arrival to the ED (transport time interval). No collinearity for elapsed time interval factors was detected among the variables when the condition index was less than 10 in the multivariable regression model for co-linearity diagnosis. All statistical analysis was performed using SAS software, version 9.4 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Demographic findings
Of 139,848 EMS-assessed OHCAs, 2,444 were P-OHCA. Resuscitation attempts by either EMS or the ED provider occurred for 2,084 patients. Of these, 2,083 cases were eligible for the assessment of final outcomes (Fig. 1). Of these 2,083 patients, each poisoning group was present in the following percentages: prescribed drugs (10.3%), pesticides (52.9%), vapors or gases (23.6%), alcohol or organic solvents (1.4%), and other poisons (13.2%; Table 1). Children (younger than 15 years) were more represented in the gaseous agents group (46.7%), and elderly people (older than 65 years) were more likely to be exposed to pesticides (58.8%; P < 0.001). Residence in a metropolis was significantly more common in the medically prescribed drug group (48.1%), and rural/urban residence was more prevalent in the pesticides group (23.3%; P < 0.001). The presence of a witness, bystander CPR, and primary ECG differed significantly among poisoning groups (all P < 0.001). The rates of survival to discharge and good neurological recovery were 3.3%/1.3% for all patients, 10.3%/5.6% for the prescribed drugs group, 2.2%/1.0% for the alcohol or organic solvents group, 2.4%/0.4% for the pesticides group, 6.9%/3.4% for the vapors and gases group, and 3.3%/2.4% for other poisons (all P < 0.001; Table 2).
Fig. 1
Study participants.
EMS = emergency medical service, OHCA = out-of-hospital cardiac arrest, P-OHCA = poisoning-induced out-of-hospital cardiac arrest, CPC = cerebral performance category.

Table 1
Frequency and percentage of poisoning agent by group
Table 2
Demographic characteristics of the study population by poisoning agent group

Values are presented as number (%). Group 1 (medically prescribed drugs; X10–X14, X40–44, Y10–Y14), group 2 (vapors or gases; X17, X47, Y17), group 3 (pesticides; X18, X48, Y18), group 4 (alcohol or organic solvents: X15–X16, X45–X46, Y15–Y16), and group 5 (other unspecified; X19, X49, Y19).
CPR = cardiopulmonary resuscitation, ECG = electrocardiogram, VF/pulseless VT = ventricular fibrillation/pulseless ventricular tachycardia, PEA = pulseless electrical activity, EMS = emergency medical service, ED = emergency department, ROSC = return of spontaneous circulation, CPC = cerebral performance category.
The proportion of patients who did not survive to the ED was 74.3% in group 1 (prescribed drugs) and 93.9% in group 2 (vapors and gases). The proportion of patients who survived to admission but died on the ward was 15.0% in group 1 (prescribed drug) and 3.9% in group 2 (vapor and gases; Table 3).
Table 3
Clinical outcomes according to poison group

Values are presented as number (%). Group 1 (medically prescribed drugs; X10–X14, X40–44, Y10–Y14), group 2 (vapors or gases; X17, X47, Y17), group 3 (pesticides; X18, X48, Y18), group 4 (alcohol or organic solvents: X15–X16, X45–X46, Y15–Y16), and group 5 (other unspecified; X19, X49, Y19).
CPC = cerebral performance category, ED = emergency department, ROSC = return of spontaneous circulation.
Main analysis
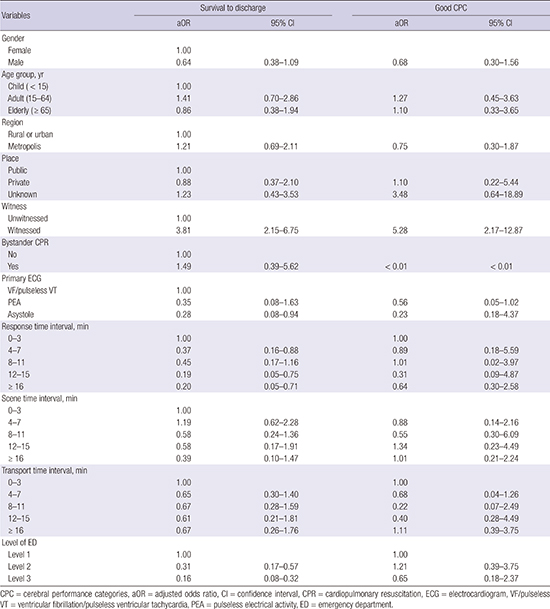
The aORs (95% CIs) of the pesticides, alcohol or solvents, and other poisons groups compared with the prescribed drugs group for survival to discharge were 0.34 (0.17–0.68), 0.33 (0.14–0.77), and 0.31 (0.13–0.77), respectively, compared with 0.47 (0.09–2.51) for the vapors and gases group. The odds ratio (OR) (95% CIs) for good neurological recovery was significant only in the pesticides group (0.07 [0.02–0.26]; the ORs for the other groups were 0.30 (0.09–1.04) for gases and vapors, 0.45 (0.05–4.48) for alcohol and sorbents, and 0.36 (0.12–1.11) for other poisons (Table 4). Appendix 1 shows the aORs (95% CIs) of potential risk that were used in the final model.
Table 4
Multivariable logistic regression analysis of hospital outcomes of P-OHCA by poisoning agent group
Values are presented as number (%) or OR (95% CI). Group 1 (medically prescribed drugs; X10–X14, X40–44, Y10–Y14), group 2 (vapors or gases; X17, X47, Y17), group 3 (pesticides; X18, X48, Y18), group 4 (alcohol or organic solvents: X15–X16, X45–X46, Y15–Y16), and group 5 (other unspecified; X19, X49, Y19).
P-OHCA = poisoning-induced out-of-hospital cardiac arrest, OR = odds ratio, CI = confidence interval, ECG = electrocardiogram.
*Adjusted for age, gender, region, place, witness, bystander cardiopulmonary resuscitation, primary ECG, response time interval, scene time interval, transport time interval, and level of emergency department.
DISCUSSION
We categorized poisoning agents into five groups and determined the differences among them and the outcomes of OHCAs by group. Of the causative toxic agents, pesticides/herbicides represented the largest proportion of OHCAs (52.9%), which is consistent with previous studies performed in Korea — 48.6% reported by Park et al. (10) and 50.9% by Shin et al. (19). The previous study extracted the poison source from the medical records. However, this study used the information from a review form designed according to International Classification of External Causes of Injuries poison group to reduce the misclassification bias. Although many unknown values remained in this study, more cases were precisely classified using the data-variable dictionary for poison group.
We found that P-OHCA caused by pesticides/herbicides occurred mostly in older people living in rural areas. Because of industrialization, many young people have moved to major cities, while older farmers have remained in rural areas. Consequently, elderly individuals residing in rural areas are more readily exposed to agricultural agents than younger people (20).
Because of the widespread availability of pesticides/herbicides, they have become the most commonly used agent for suicides in developing countries, whereas opioid analgesics are the most commonly used agent in the United States (202122). Patients in group 3 also had the lowest bystander CPR rate, which suggests that they mostly lived alone, without family, and that rural populations may have a low level of knowledge of CPR. As metropolitan areas accommodate more individuals, the transport time interval was shorter.
Of the various causative agents of P-OHCA, the rates of survival to discharge and good neurological recovery were better for medically prescribed drug-induced OHCAs than for OCHAs induced by other causative groups: gaseous agents, pesticides/herbicides, and others. A previous epidemiological study found that the survival to discharge rate of P-OHCA patients was related to the causative agent and that prescribed drugs (sedatives, psychotropics) showed the highest survival to discharge rate (14.3% and 7.7%, respectively), which is consistent with our results (10.3%) (10).
In a report on 5,529 cases of individuals intoxicated by recreational drugs and new psychoactive substances in Europe, 69.5% of these individuals went to the hospital by ambulance, 56.9% of whom were medically discharged from the ED; only 35 (0.6%) presented with cardiac arrest (23). In Germany, a report using poison data from ambulance services found that 10.8% of the 91,285 patients has dysrhythmia, and 111 (0.1%) had cardiac arrest (24). We could not directly compare our findings with the cardiac arrest survival rate of this study due to the lack of information on survival. Previous studies on poisoning and cardiac arrest outcomes have mostly been case reports on specific agents. A systematic report form for P-OHCAs will help compare the etiology and outcomes by community.
Recent medical technology can help clinicians save more lives from poisoning through extracorporeal membrane oxygenation (ECMO) devices. An intoxicated patient who had collapsed after amlodipine and metoprolol use was treated with ECMO and showed intact neurologic function. (2526) Furthermore, a patient recovered fully from 82 minutes of no and low flow during arrest and resuscitation after receiving ECMO therapy and hypothermia (27). Our data include a very small number of patients (n = 6) who received ECMO treatment (2.3% of 266 survivals to admission). Hypothermia treatment was more common (n = 41 cases, 15.4% of survival to admissions) in our study. This new technology and temperature management should be considered to improve the outcomes after P-OHCA.
We did not include OCHAs caused by poisoning with natural toxins from snakes, bee stings, or foods, which could not be clarified in the clinical setting. Those toxins are not obvious or can be confused with anaphylaxis and followed by OHCA. Further studies are needed regarding those natural toxins and OHCA outcomes. We re-categorized the alcohol and organic sorbent materials in this study. Of 10 alcohol-induced and 19 organic sorbent-associated cardiac arrest cases, only 1 person survived with good CPC. We did not separate the patient groups in these categories due to the small sample size. Further studies on these specific poisons are needed.
In this study, only 11.8% of the sample had OHCA due to an unspecified poison. All others had an identified poison source. If we had known the exact poison at the prehospital stage, we could have applied an antidotal therapy. The most common poison sources were pesticides and herbicides in this study setting (52.9%). Several pesticides have exact antidotes that can be used in an emergency setting. For several prescribed drugs, we can also supply EMS providers with specific antidotes to restore cardiac function. This study highlights the need for contemporary confirmation of poison sources and the probable availability of antidotal therapy in the field during resuscitation.
Our study found a greater proportion of pesticide-associated OHCAs than has been reported in other communities. To prevent pesticide overuse or suicide, accessibility to pesticides should be reduced by legal control, technical methods, behavioral changes, and public health efforts.
The study has several limitations. First, we only included EMS-transported P-OHCA patients and excluded patients with unknown final outcomes. Some patients may have died without any resuscitation efforts due to prolonged cardiac arrest. Additionally, some patients may not have been identified with P-OHCA due to a lack of information or bystanders. These cases could have biased the association between poisoning group and outcomes. The total number of deaths due to poisoning reported during the same study period (2008–2013) by the National Death Certificates was 29,519. Our study collected a total of 2,444 poisoning-associated OHCAs, comprising approximately 8.3%. The other 91.7% died without EMS transportation or died during clinical treatment without any prehospital cardiac arrest in the field. Therefore, we could not estimate the exact proportion of P-OHCA patients who were not enrolled in this study. Second, based on the ICD-10 codes for poisoning agents, we re-categorized the patients into five groups (medically prescribed drugs, gaseous agents, pesticides/herbicides, and other) to obtain a sufficient number of cases for the logistic regression analysis. This categorization may have blurred the effects of each specific causative agent on hospital outcomes. Due to a lack of details regarding the brand names of pesticide or herbicides, we did not analyze the specific effects of the poisons. Third, as the study was performed in the context of basic to intermediate levels of EMS, the study findings should be generalized with caution to other EMS environments.
From a nationwide OHCA registry, we found that survival to discharge and good neurological recovery after P-OHCA were the highest for the prescribed drugs group and the lowest for the pesticides group, followed by the vapors or gases group.
 XML Download
XML Download