

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
To ensure successful implant-based restoration, various factors must be taken into account before implant placement, such as bone quality, alveolar bone height/width, implant fixture position, esthetics, and dental occlusion [12]. Among these considerations, correct placement of the implant fixture is especially important for accurate prosthesis restoration and oral hygiene. After tooth extraction and implant-based restoration, well-healed alveolar bone is a good indication of correct dental implant placement [34]. Severe vertical alveolar bone loss often occurs due to severe chronic periodontitis and necessitates tooth extraction. In some cases, this can lead to a height difference with the adjacent alveolar bone, and vertical bone augmentation is necessary to recover normal ridge height [56].
With the introduction of short implants, many patients might not receive proper ridge reconstruction, because the surgical procedure has been simplified and it is difficult to elongate the soft tissue enough to cover the augmented bone. When the implant is to be placed in a low ridge position, the fixture platform must be located at a lower level. As a result, the platform may obstruct the continuity of the alveolar ridge [7], necessitating a large, relatively long implant prosthesis with a short-length fixture. This, in turn, results in a hypsodont-shaped restoration resembling an herbivore tooth (Figure 1A-C) [8]. In contrast to hypsodont morphology, normal human teeth have a brachydont shape (Figure 1D-F) [9]. With progressive vertical bone loss, a stepped crown margin develops under the adjacent tooth that is difficult to clean in daily life. Eventually, such implants are prone to dental plaque accumulation, which induces inflammation and peri-implantitis [710]. Therefore, clinicians must perform vertical bone augmentation to re-establish favorable inter-arch relationships for the maintenance of oral hygiene. To achieve the proper alveolar ridge level and ideal restoration, ridge reconstruction should be considered before implant placement, as should delayed implant placement with bone augmentation [1112].
Figure 1
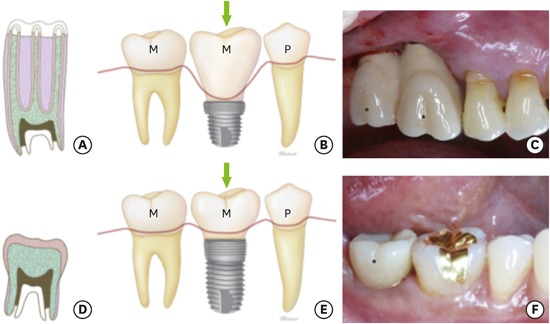
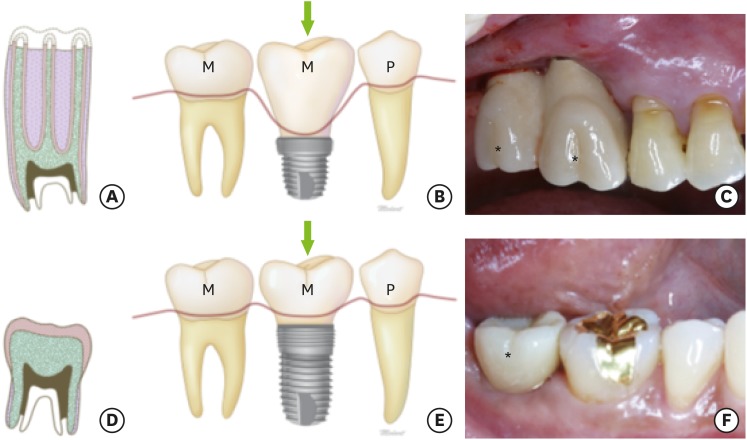
The terms ‘hypsodont’ and ‘brachydont.’ (A-C) ‘Hypsodont’ describes a tooth with large crowns. A schematic drawing of a hypsodont-like implant-based restoration is shown (marked with an arrow), as well as a clinical photo (marked with asterisks). (D-F) The term ‘brachydont’ refers to low-crowned teeth. A schematic drawing of a brachydont-like implant-based restoration is shown (marked with an arrow), as well as a clinical photo (marked with asterisks).
M: molar, P: premolar.
In the present report, we describe a case series of flap preparation procedures using a novel K-incision technique (named by Y.K.) for vertical bone augmentation. This technique allows dental surgeons to recover the proper alveolar ridge, to create a healthy periodontal region, and to increase dental implant longevity.
CASE DESCRIPTION
This retrospective study was approved by the Institutional Review Board (IRB No. S-D20180006) of Seoul National University School of Dentistry, Republic of Korea.
Population
The present study involved 3 patients, none of whom; 1) had relevant medical or dental histories, 2) were smokers, 3) had any contraindications for periodontal surgery, or 4) had taken medications known to interfere with periodontal tissue healing.
Surgical procedure
All surgical procedures were performed by a single operator (Y.K.), and all involved extraction of a periodontally compromised tooth followed by vertical bone augmentation using a K-incision at the healed, low-level alveolar ridge. Specifically, the teeth were diagnosed as hopeless, with severe alveolar bone defects caused by chronic periodontitis. They were extracted under local anesthesia (lidocaine HCl; 2% injection [1:100,000], Huons, Seongnam, Korea), meticulous debridement of the socket was carried out, and the area was thoroughly cleaned using sterile saline (0.9% sodium chloride). After a soft tissue healing period of around 2 months, guided bone regeneration (GBR) was performed before implant placement. In the missing tooth site with a vertical bone defect (Figure 2A), a partial-split K-incision was made using a Kirkland knife to split the gingival flap into 2 equal parts (Figure 2B). The denuded cortical bone was drilled using a round bur to ensure decortication and to promote osteogenesis from the bone marrow (Figure 2C) [13]. A microscrew (Jeil Medical Corp., Seoul, Korea) was used as a tent pole to support the augmented bone height. GBR was carried out using inorganic bovine bone mineral (OCS-B®, NIBEC, Jincheon, Korea) and a titanium-reinforced (TR), high-density polytetrafluoroethylene (Gore-Tex®, W. L. Gore & Associates Inc., Newark, DE, USA) or collagen membrane (Bio-gide®, Geistlich Pharma AG, Wolhusen, Switzerland) was used (Figure 2D). The soft tissue was extended for as long as it was divided in half, and the buccal vestibular depth was not changed, securing the keratinized gingiva (Figure 2E).
Figure 2
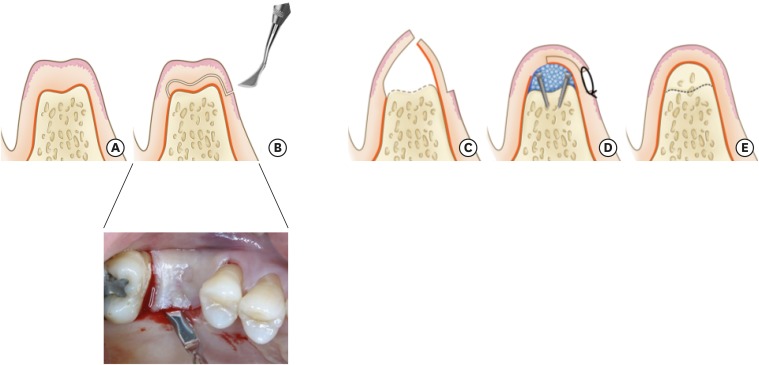
Schematic illustration of the K-incision. (A) Alveolar ridge showing a vertical bone defect. (B) A K-incision is performed using a Kirkland knife to split the gingiva into 2 parts. (C) After elevation of the gingival flap, decortication is performed to promote osteogenesis. (D) The microscrews are used as tent poles, and bovine bone mineral and membrane are applied. The divided gingival flap is then sutured. (E) After a 4-month healing period, the alveolar ridge shows vertically recovered bone with sufficient keratinized gingival tissue and an unchanged mucogingival junction level; the ridge is ready to receive an implant.
Case 1
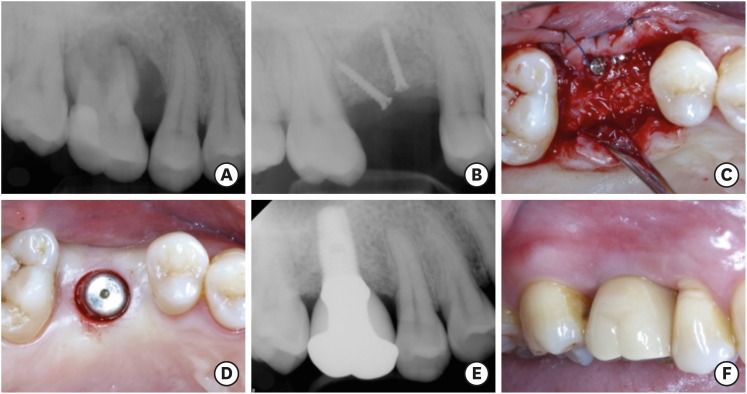
A 59-year-old woman presented with periodontally compromised maxillary molars (teeth #2 and #3) and severe bone resorption. The teeth were extracted (Figure 3A). The woman showed severe vertical bone loss, and microscrew-retained GBR was thus planned before implant placement (Figure 3B). To this end, a partial-split K-incision was performed, and inorganic bovine bone mineral and a TR membrane were applied. The flap was then sutured (Figure 3C and D). The elongated soft tissue portion was extended by approximately 4–5 mm (Figure 3D). After 4 months, an External Hex RESTORE® RBM implant (4.0 mm in diameter×10.0 mm in length MAUSA, Keystone Dental, Inc., Burlington, MA, USA) was successfully placed in the proper position without any sinus bone graft, and the denuded connective tissue was fully covered using keratinized gingiva (Figure 3E). The radiograph in Figure 3F shows a moderate length of the implant prosthesis, and the alveolar bone around the dental implant was well maintained during 5 years of periodic follow-up.
Figure 3
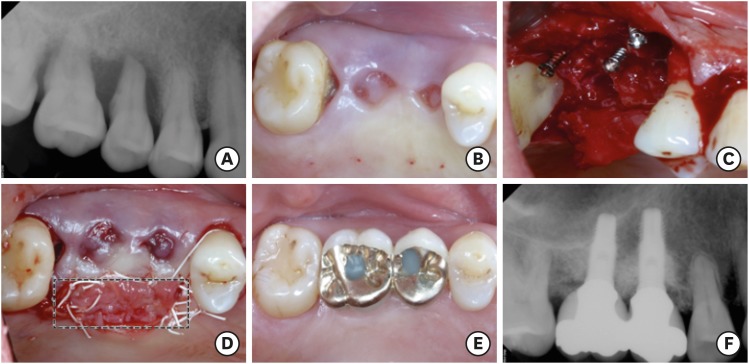
Case 1. (A) A periapical radiograph showing alveolar bone resorption around the teeth (#2 and #3). (B) An occlusal view of the tooth extraction site (teeth #2 and #3) after a 2-month healing period. (C) The microscrews were used as tent poles during guided bone regeneration. (D) The soft tissue extended by the K-incision is marked with a black tetragon. (E, F) A clinical photo (E) and radiograph (F) show the stable implant restoration with sufficient keratinized gingival tissue and alveolar bone over a 5-year periodic-recall follow-up period; no specific complications were observed.
Case 2
The maxillary molar (tooth #3) of a 47-year-old man was scheduled for extraction after a diagnosis of chronic periodontitis. The clinical and radiographic examinations showed severe vertical bone loss (Figure 4A), so a microscrew-retained GBR was planned before the implant placement (Figure 4B). After 4 months of GBR, sufficient bone height and width were achieved to place the implant fixture (Figure 4C). A dental implant (RESTORE® RBM, 4.0 mm in diameter×10.0 mm in length) was successfully placed in the proper position (Figure 4D). During a 3-year follow-up after installation of the implant prosthesis, a stable augmented bone condition was observed (Figure 4E); around the implant prosthesis, there was proper keratinized gingiva and a healthy periodontal region (Figure 4F).
Figure 4
Case 2. (A) A periapical radiograph showing alveolar bone resorption around tooth #3. (B) Guided bone regeneration with microscrews in the vertically resorbed alveolar ridge. (C) Flap re-opening to remove the microscrews and to place the implant. (D) Sufficient keratinized gingiva around the implant. (E) A radiograph and (F) clinical photo showing the stable implant-based restoration over the 3-year periodic-recall follow-up period.
Case 3
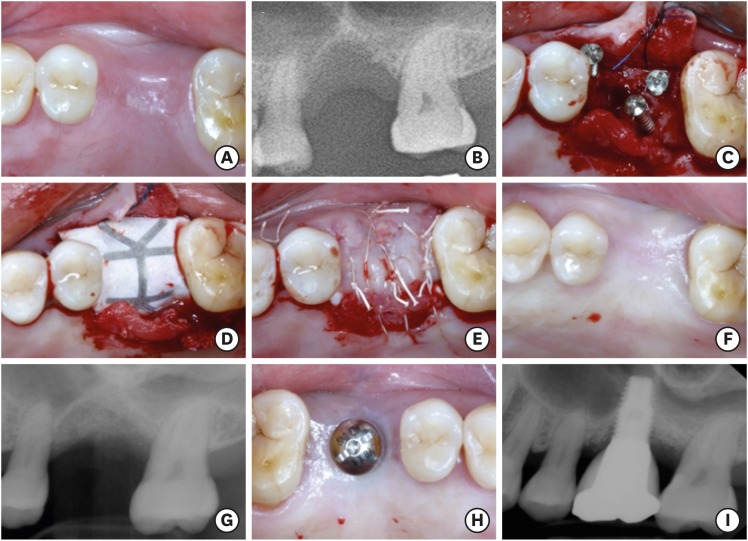
A 63-year-old man was referred from a local clinic because implant placement was impossible at the site of a previously extracted tooth (#14) without a sinus bone graft. A narrow, saucer-like alveolar ridge was observed upon an oral examination (Figure 5A), and the radiograph from the local clinic showed deficient bone healing and a sinus septum at the center of the site of the missing tooth (Figure 5B). We performed microscrew-retained GBR (Figure 5C-E) with a K-incision using inorganic bovine bone mineral and a TR membrane. We could see the extended soft tissue in the palatal site (Figure 5E). After 4 months, the surgical site was well healed and showed sufficient recovery of alveolar bone width and height, so the microscrews were removed (Figure 5F). The augmented bone was well maintained (Figure 5G), and the implant fixture (RESTORE® RBM, 4.0 mm in diameter×10.0 mm in length) was successfully placed in the correct position using a sinus septum without any sinus bone graft (Figure 5H). After installation of the implant prosthesis, the augmented bone was well maintained during 2 years of periodic follow-up (Figure 5I).
Figure 5
Case 3. (A) Occlusal view and (B) radiograph showing alveolar bone resorption around tooth #14 after a 3-month healing period. (C) The microscrews were used as tent poles, (D) inorganic bovine bone mineral particles and a titanium-reinforced membrane were applied, and (E) the flap was sutured with no tension. (F, G) The surgical site healed well, with proper alveolar bone width and height. (H) The dental implant was placed in the correct position. (I) A radiograph showing stable implant-based restoration over a 2-year periodic-recall follow-up.
DISCUSSION
The present article reports a case series in which GBR with a K-incision was used to treat severe vertical alveolar bone defects, enabling optimal implant-based dental restoration. The use of short implants makes it easier to restore missing tooth sites that show vertical bone loss. However, this procedure usually worsens the balance with the surrounding natural teeth, which is important for maintaining the condition of the peri-implant tissue.
We used the terms ‘brachydont’ and ‘hypsodont’ because they are precisely defined and allow a clear comparison of 2 distinct types of tooth morphology (Figure 1). A hypsodont-like implant-based restoration is unavoidable on vertically resorbed alveolar ridges without vertical bone augmentation. Patients may subsequently exacerbate pathological peri-implant conditions in daily life with inappropriate tooth-brushing. Indeed, we often encounter patients with hypsodont-like implant-based restorations who complain of difficult and painful tooth-brushing.
Peri-implant pathology is primarily associated with biological and biomechanical factors [14]. There are many risk factors for peri-implantitis, such as a history of periodontitis [15], deficiency of keratinized gingiva [1617], and a shallow buccal vestibule [18]. With the exception of periodontitis, almost all these risk factors involve the implant itself — that is, the implant fixture position, prosthesis shape, and so on [14]. These aspects are fully controlled by the dentist. Therefore, dentists must endeavor to create precise, brachydont-like implant-based restorations.
In this regard, GBR is a basic procedure for recovering normal alveolar bone anatomy and ensuring the correct positioning of implant fixtures. The periosteal releasing incision is a common GBR procedure that allows complete coverage [19]. However, pulling the flap to the augmented site can change the buccal mucosal level, inducing a deficiency in the keratinized gingiva and resulting in a shallow buccal vestibule. The double-flap incision was introduced to advance the flap to enhance tension-free primary closure [20]. However, it can change the buccal mucosal level, and is difficult to regenerate the keratinized gingiva. In contrast, our K-incision has the following advantages over the releasing incision: conservation of buccal vestibular depth, maintenance of the keratinized gingiva after extension over the connective tissue portion, and regeneration of the keratinized gingival tissue. Technically, in this type of split incision, the Kirkland knife allowed easier control of the flap than other types of blades, which could reduce unexpected lacerations. All these factors are important for preventing complications of GBR procedures and maintaining peri-implant health. Although GBR requires more treatment time than implant placement alone, the procedure allows brachydont-like implants to be made and is conducive to oral hygiene. In most cases of GBR, there is no need to perform a sinus bone graft, and an incidental guided tissue regeneration (GTR) effect can be observed in the peripheral teeth.
In the present case series, representative regenerative aspects were seen on the mesial side of tooth #1 and on the distal side of tooth #4 in case 1. This is the natural result of root planing in adjacent teeth. Previously, we reported that untreated periodontitis in an adjacent tooth had a negative effect on the osseointegration of dental implants [21]. The present results indicate that GTR can be performed concomitantly with GBR using root planing, and confirm that thorough debridement of the contaminated root surface is important for regenerative therapy.
Despite its many advantages, the K-incision technique may be limited in that it requires a highly trained dental surgeon to split the thickness of the gingiva. Furthermore, the procedure requires a long period of discomfort caused by missing teeth. Further long-term follow-up and a large-scale randomized clinical investigation should be performed to evaluate the feasibility of this technique.
 XML Download
XML Download