

 PDF
PDF Citation
Citation Print
Print



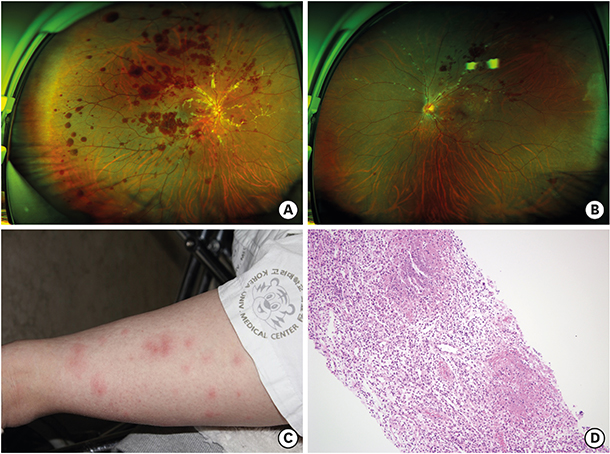
A 29-year-old female visited the emergency room with sudden visual loss in the right eye started on the same day. She had been suffering from fever for two days. A best-corrected visual acuity (BCVA) was 0.5/0.7 in the Snellen chart. Fundus examination (Fig. 1) showed multiple retinal hemorrhages. Severe vascular sheaths around the optic disc area were present in the right eye. Candle-wax-dripping sign in the superior hemisphere were found in the left eye.
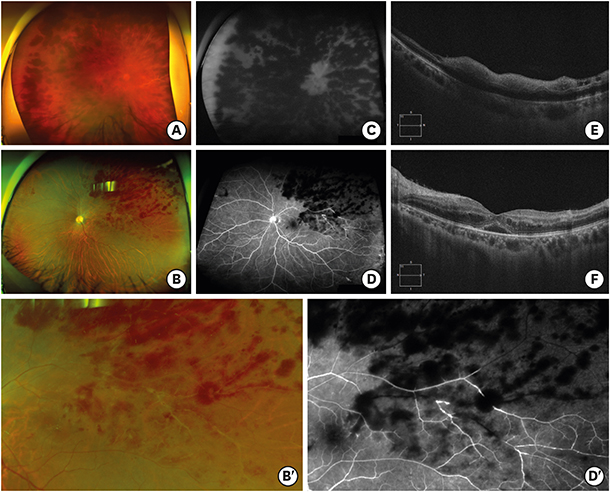
On systemic examination, erythema of the lower extremities (Fig. 1C) and right inguinal lymph node enlargement were discovered. With systemic doxycycline (100 mg) and gentamicin (90 mg) administration, fever subsided after three days. Bartonella infection was confirmed after 10 days with in-house indirect immunofluorescent assay (IFA) analysis (immunoglobulin G; cutoff points for seropositive titer at 1:64).1 Lymph node biopsy showed necrotizing granulomatous lymphadenitis (Fig. 1D). On the same day, the BCVA decreased to hand motion in the right eye. When asked, she could not specify when the vision loss began. The candle-wax-dripping sign in the left eye had progressed to vascular sheath with flame-shaped hemorrhages. Fluorescein angiography shows a rack of filling of the retinal arteries. Blocked fluorescence by retinal hemorrhage was found in the whole area of right eye and in the superotemporal quadrant of left eye. Inner-retinal hyper-reflectivity of the right eye and cystoid macular edema in the left eye were revealed (Fig. 2). The impression was central retinal artery and vein occlusion for the right eye and branch retinal artery and vein occlusion for the left eye, associated with severe vasculitis secondary to Bartonella infection. The patient was treated with a systemic methylprednisolone 500 mg, anticoagulant (Enoxaparin sodium 60 mg) and Rifampin (300 mg). Three month after disease onset, the BCVA in the right eye improved to 0.1. For photographs and medical records that consisted possible identification of the patient, a consent form was obtained from the patient for use of publication.


 XML Download
XML Download