

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bladder tumors are rarely found in the first two decades of life. Transitional cell carcinoma (TCC), which is commonly found in adults, is rare in patients ≤ 20 years of age and accounts for only 0.1%–0.4% of all TCC cases.12 In addition, TCC is much more rare in the first decade of life, with reported incidence rates of only –20% of patients ≤ 20 years of age.34 Moreover, it is very difficult to diagnose bladder cancer due to limitations in the methods of diagnosis that can be applied to patients of this age. Nevertheless, there is no guideline for pediatric bladder cancer, so clinicians are planning treatment according to the guideline of adult. Since the tumor types found in the bladder vary based on age, it is important to understand which bladder tumors commonly occur in patients ≤ 20 years of age.5 However, few studies have reported the clinical characteristics of bladder tumors in patients ≤ 20 years of age. Furthermore, most previous studies were based on bladder tumors in Western populations, with reports based on Eastern populations limited to only case studies.678910111213 Accordingly, it is not possible to comprehensively compare pediatric bladder tumors between Western and Eastern populations. In this study, we investigated the clinicopathological characteristics of urinary bladder tumors in patients < 20 years from a patient cohort in Korea.
METHODS
We retrospectively reviewed the charts of 21 patients, aged 20 years or younger, who received bladder surgery at one of two institutions (Asan Medical Center and Ulsan University Hospital), between July 1996 and January 2013. We analyzed the demographic data, chief complaints at first visit, cystoscopic findings, pathology results, and clinical follow-up data. In cases of TCC, pathologic slides were retrieved and reclassified using the 2004 WHO system.14 In cases of rhabdomyosarcoma, we analyzed the primary site (bladder or prostate), tumor size, pathologic type, staging, and clinical group according to the Intergroup Rhabdomyosarcoma Study,15 were analyzed.
RESULTS
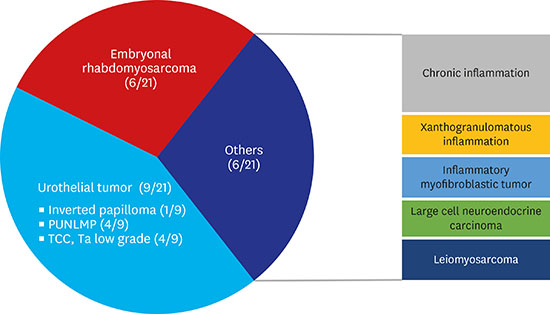
The mean patient age at initial diagnosis was 12 years (range, 1–20 years) and the male-to-female patient ratio was 4.25:1.00. The median follow-up duration was 76 months. Pathology revealed 9 urothelial tumors, 6 rhabdomyosarcomas, 1 low-grade leiomyosarcoma, 1 large cell neuroendocrine carcinoma, 1 inflammatory myofibroblastic tumor, and 3 cases of chronic inflammation without tumors (Fig. 1).
Fig. 1
The pathologic findings of patients with bladder tumors.
PUNLMP = papillary urothelial neoplasms of low malignant potential, TCC = transitional cell carcinoma.

In the 9 patients with urothelial tumors, the mean patient age was 16 years (range, 5–20 years) and the male-to-female ratio was 2:1. All patients were teenagers, except for 1 (Table 1). Of these patients, 6 had gross hematuria as the chief complaint and 3 patients presented no symptoms. Voided urine cytology was examined in all patients, with the results found to be negative in all cases. The characteristics of urothelial tumors showed that all tumors were relatively small in size (mean size, 1.9 cm; range, 0.7–3.0 cm) and were solitary and polypoid lesions with stalks (Fig. 2). All patients underwent transurethral resection of bladder tumor (TURB) for treatment. Of the 9 patients with urothelial tumors, 1 had inverted papilloma, 4 had papillary urothelial neoplasms of low malignant potential (PUNLMP), and 4 had TCC (pathological stage Ta low-grade). Of the 4 cases of TCC, recurrence occurred in 1 case, in which the tumor was incompletely resected and TURB was then performed again 5 months later. All patients had a follow-up with ultrasonography and computerized tomography imaging, without cystoscopy. All of these patients remain alive and recurrence-free, with a mean follow-up duration of 89 months (range, 24–215 months).
Table 1
Patients of urothelial tumors
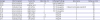
Fig. 2
Urothelial tumor.
The patient was a 13-year-old girl who presented with gross hematuria. The urothelial tumor was diagnosed as papillary urothelial neoplasm with low malignant potential. (A) On ultrasound, a single solitary mass is seen near the right ureteral orifice (arrow). (B) Cystoscopic view of same tumor shows a papillary mass with a stalk.
In 6 patients with rhabdomyosarcoma, the mean age was 5 years (range, 1–14 years) and the male-to-female ratio was 5:1 (Table 2). One patient was 14 years old at the time of diagnosis and all others were under the age of 5 years. Two out of 5 boys had rhabdomyosarcoma from the prostate (Fig. 3). Three of these patients complained of voiding difficulty or bladder distention, with the remaining patients complaining of gross hematuria without voiding symptoms. The histologic findings of all patients were of embryonal type. Characteristics of rhabdomyosarcoma showed that all tumors were relatively large in size and had a broad base. To determine the primary diagnosis of rhabdomyosarcoma, 1 patient underwent sonography-guided needle biopsy, 3 patients received cystoscopic biopsies, and 2 patients underwent TURB. All the stage 2/group I rhabdomyosarcomas were diagnosed by cystoscopic biopsy, and were treated with chemotherapy and subsequent TURB. Among the 3 patients with stage 3/group III rhabdomyosarcoma, 2 received chemotherapy and radiotherapy, and another patient, who was 1 year old, underwent a radical cystectomy after chemotherapy without radiotherapy. The patient who underwent a radical cystectomy died 14 months after surgery and the 2 patients who underwent chemotherapy and radiotherapy were alive and recurrence-free, with a follow-up duration of 53 and 108 months, respectively. One of these previously mentioned patients underwent a radical cystectomy, owing to uncontrolled radiation-induced hemorrhagic cystitis, and no residual tumor was found in the excised bladder.
Table 2
Patients of embryonal rhabdomyosarcoma
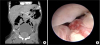
Fig. 3
Rhabdomyosarcoma.
The patient was a 2-year-old boy who presented with voiding difficulty. (A) On computed tomography, a mass of 5 cm in size is located on the prostate. (B) Cystoscopic view shows tumor invading the bladder neck.
Three patients were diagnosed with chronic inflammation. Gross hematuria was the main symptom in these patients, with ultrasonography used to diagnose the bladder tumor. After receiving treatment with TURB, a single 19-year-old patient was diagnosed with xanthogranulomatous inflammation; no other pathologic findings were discovered in any of these 3 patients.
In a 13-year-old patient with leiomyosarcoma, gross hematuria was the chief complaint. A computed tomography scan revealed a 5-cm solid and cystic mass, located at the anterior urinary bladder wall. Partial cystectomy was performed as the initial treatment. This patient is alive and recurrence-free for approximately 10 years.
In the 13-year-old patient presenting with an inflammatory myofibroblast tumor, gross hematuria was the chief complaint. A computed tomography scan revealed a 4.8-cm solid mass at the bladder dome. A transurethral resection was performed, followed by a partial cystectomy. He is alive and recurrence-free for 65 months.
DISCUSSION
Tumor of the urinary bladder is a very rare disease in patients aged 20 years and younger.16 In addition, it is difficult to diagnose these patients since there are many limitations in diagnostic examination, such as cystoscopy or computerized tomography imaging. Therefore, identifying the clinical characteristics of bladder tumors diagnosed at this age is crucial information for the planning of patient management. There have been numerous studies of bladder tumors in patients aged under 40 years, but most of these patients were older than 20 years of age.61718 Since these studies showed that there were many differences in tumor characteristics, even in patients between 20 and 30 years old, it is difficult to understand the characteristics of bladder tumors for patients under 20 years of age, based on these previous reports.319 While previous studies have examined bladder tumors in patients aged under 20 years old, the analyzed patients were from Western populations; studies investigating bladder tumors in Eastern populations, under 20 years of age, are currently scarce.
In this study, urothelial tumors and rhabdomyosarcoma were found to be the most common bladder tumor types among patients 20 years of age and younger. Our distribution of bladder tumor type is similar to that observed by Alanee and Shukla,5 which was based on data from the Surveillance, Epidemiology and End Results (SEER) database (urothelial tumors including PUNLMP, 60%; rhabdomyosarcoma, 36.4%). In particular, our study showed that rhabdomyosarcoma occurred in children under 10 years of age; and urothelial tumors were most common in patients aged 10 years or older, which is consistent with the results of previous study.5
For patients in this study, urothelial tumors were mostly a single lesion, which comprised of a papillary shape and stalks. The most common manifestation was gross hematuria, but many cases were associated with an incidental mass. In most cases, diagnosis was often delayed because it is difficult to diagnose bladder tumors.2021 In spite of these features, bladder tumors are rarely diagnosed as high-grade or invasive urothelial carcinoma, even when diagnosed in a late stage to present with gross hematuria; this has led to the practice of not pursuing aggressive diagnoses, since these tumors rarely progress.316192021222324
Bladder tumors rarely recur in pediatric patients.1624 Therefore, performing cystoscopy every 3 months to detect small recurrent lesions, which is standard practice for adult patients, is not necessary for pediatric patients with urothelial tumors, and follow-up using sonography alone may be an optimal choice. Since TCC is typically a low-grade malignancy that rarely recurs, voided urine cytology is typically not useful in the diagnosis and follow-up of bladder tumors in this age. As seen in this study, if the first transurethral resection is not sufficient, tumors may recur. Therefore, proper resection is very important to eradicate these tumors.
For patients under 10 years old with bladder tumors, the incidence of rhabdomyosarcoma was higher than urothelial tumors, and previous studies have reported similar findings.5 In the cases of rhabdomyosarcoma, the genitourinary tract is the second most common site,22 with preference for the prostate and bladder.23 In the case of rhabdomyosarcoma, symptoms may be different depending on tumor location. Bladder outlet obstructive symptoms were reported by patients with tumor on prostate, but gross hematuria was the chief complaint among patients with tumor on bladder.25 However, as shown in the present study, there were many cases in which children were present before the end of voiding training, which showed palpable mass-like lesions in the lower abdomen due to bladder distention caused by retention, rather than complaints of bladder outlet symptoms. Rhabdomyosarcoma cases showed a huge mass with unclear boundaries, unlike urothelial tumors, which present as small and papillary shaped with stalks. Previously, exenteration was performed in patients diagnosed with bladder and prostate rhabdomyosarcoma.2225 However, treatment with the Intergroup Rhabdomyosarcoma Study (IRS)-III and IV protocol, which used more chemotherapy and radiotherapy preoperatively, showed improved survival, while preserving the bladder.2325 Since these tumors are often unresectable, due to localization in the prostate or bladder trigone, as well as being chemosensitive, chemotherapy has been performed first after biopsy, with radiotherapy or surgical resection being subsequently performed for the remnant tumor. As a result, only 9% of patient with IRS-IV protocol underwent radical cystectomy and their survival rate was as high as 82%.23 As shown in the present study, complete resection of the remnant tumor by transurethral resection after chemotherapy showed no recurrence of tumor, when the tumor could be resected completely. In addition, it was confirmed that radiotherapy alone for remnant tumors after chemotherapy can provide sufficient therapeutic results for unresectable tumors.26 One patient that underwent radical cystectomy after chemotherapy and radiotherapy had no rhabdomyosarcoma tumor cells in their resected bladder. This finding suggests that chemotherapy and radiotherapy can achieve sufficient therapeutic effect for rhabdomyosarcoma.
The first limitation of the present study was the diagnosis of chronic inflammation in 2 patients. These patients were younger than 5 years of age and their tumors did not show a papillary pattern, suggesting that rhabdomyosarcoma was suspected, but pathologic lesions were not observed. These results imply that there either were no pathologic lesions, or the entire pathologic lesion was ablated during TURB. After treatment, there was no recurrence found at follow-up for more than 1 year, but the exact tumor pathology could not be confirmed. The second limitation of this study was the fact that patients were collected from 2 centers, which cannot be considered to completely represent the tendency of pediatric bladder tumors in Korea. In particular, in the case of the remaining tumors except for urothelial tumors and rhabdomyosarcoma, it is difficult to predict their tendency since only 1 case was diagnosed for each respective tumor type. It may be necessary to investigate the data of several other institutions regarding pediatric bladder tumors.
In conclusion, urothelial tumors are the most common type of pediatric bladder tumors, with embryonal rhabdomyosarcoma being the second most common. Urothelial tumors in pediatric population have specific characteristics, including solitary and polypoid features, and are common in relatively older age pediatric patients. Since urothelial tumors in children show a good prognosis and rarely recur, TURB is the choice of treatment for these patients. Moreover, embryonal rhabdomyosarcomas are common in younger aged patients, and have a broad base and diffuse features. Since embryonal rhabdomyosarcomas are typically chemosensitive, combined treatment with chemotherapy and radiotherapy typically administered for bladder preservation. However, surgical resection may be considered if tumors can be completely resected after chemotherapy.
 XML Download
XML Download