

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Penile squamous cell carcinoma (PSCC) is a rare malignancy with a highly variable incidence.1 Annually, PSCC accounts for 0.4%–0.6% of all malignant neoplasms occurring in men in the USA,2 although rates as high as 10% have been reported among men in developing countries within Asia, Africa, and South America.3 In 2013, the Korea Central Cancer Registry recorded that PSCC accounted for 0.1% of all newly diagnosed malignancies in men.4 Despite the very low incidence, PSCC has disappointingly high mortality and morbidity rates. Adjuvant treatments (ATs), including chemotherapy (AC) or radiotherapy (AR), have been administered to patients with high-grade penile tumors in the same manner as for other solid cancers, with the aim of improving the poor prognosis. However, sufficient data are not available to support decision-making about the use of AT.
Currently, there is no consensus regarding standardized treatment for PSCC management. Given the absence of high-level evidence regarding this rare disease, the National Comprehensive Cancer Network (NCCN) relied on the experience of penile cancer experts when setting guidelines.5 Although recent studies reported the efficacy of AT for PSCC,67 additional data may help to standardize the management of this malignancy.5 Therefore, this study aimed to present a composite of the outcomes of treatment, including AT, among patients with PSCC who were treated at multiple Korean institutions.
METHODS
Study population and data collection
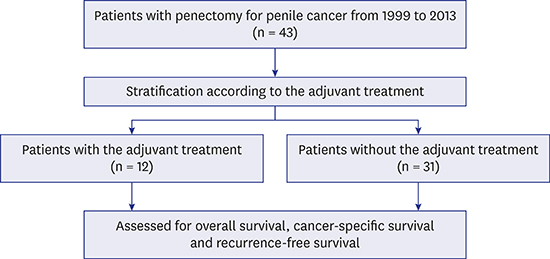
We reviewed the medical records of all cases diagnosed with PSCC and treated at three hospitals between 1999 and 2013. A total of 43 patients received treatment at Sinchon Severance Hospital, Gangnam Severance Hospital, and the National Health Insurance Service Ilsan Hospital. Patients' characteristics, including clinico-pathologic data such as the age at diagnosis, clinical history and physical examination, disease staging, and primary treatment options, and the presence of AT, were reviewed.
PSCC diagnoses were made according to the clinical history, physical examination, and biopsy results. Primary treatment for PSCC included partial or radical penectomy with concomitant inguinal lymph node dissection (ILD), which included ipsilateral or ilioinguinal lymphadenectomy via contralateral superficial inguinal or ilioinguinal dissection according to the clinical condition. After treatment of the primary tumor, the decision to proceed to ILD was based on the European Association of Urology (EAU) guidelines of 2002, 2004, and 2009.8910
Clinical staging was performed according to international guidelines and was based on data from a physical examination and cross-sectional computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)-CT. Tumor staging was standardized using the American Joint Committee on Cancer (AJCC) system,11 and tumors were graded as well, moderately, or poorly differentiated. All surgical specimens were analyzed by uropathologists at each institution.
Postoperative follow-up evaluations were conducted at 3-month intervals during year 1, 6-month intervals during year 2, and annually thereafter, with laboratory and imaging studies as clinically indicated. Death certificates were used to assess causes of death, which were corroborated via chart review.
Assessment of adjuvant treatment
AT was defined as the performance of AC, AR, or both within 12 months after penectomy. AC comprised cisplatin, methotrexate, and bleomycin (CMB) administered at respective doses of 100 mg/m2 over 1 hour, 25 mg/m2, and 10 mg/m2 over 1 hour, respectively. Four AC cycles were scheduled at intervals of 21 days. Carboplatin was substituted for cisplatin in patients with a serum creatinine clearance rate < 50. Patients treated with at least two cycles of chemotherapy were considered to have received AC. The treatment protocols and follow-up schedules were surgeon-dependent. Tumors were not routinely staged postoperatively prior to AT.
Statistical analysis
Patients were divided into two groups according to the presence of AT (AC, AR, or both): AT (+) (n = 12; 27.9%) and AT (−) (n = 31; 72.1%). Categorical associations were evaluated using the Mann-Whitney test. A review of the clinical notes facilitated a calculation of survival rates and construction of Kaplan-Meier curves, and significant differences were determined using the log-rank test. A multivariable analysis was performed using a Cox proportional hazards model that included the AJCC disease stage and tumor grade as covariates. Analyses were performed using SPSS 23.0 (SPSS, Inc., Chicago, IL, USA). All P values were two-sided, and a P value < 0.05 was considered to indicate statistical significance.
RESULTS
Table 1 presents the basic characteristics of patients diagnosed with PSCC at the participating institutions from 1999 to 2013. The median age at diagnosis was 67.0 years (interquartile range: 53.1–72.0), and patients were followed up for a median of 26.4 months (12.0–62.8). The majority of primary lesions presented on the glans (n = 26; 60.5%) and occasionally involved both the glans and adjacent structures (urethra [n = 9; 20.9%], shaft [n = 8; 18.6%]). Partial penectomy was performed in the majority of cases (n = 37; 86.0%). Twenty-four (55.8%) patients were diagnosed with pT stage ≥ T2 disease. The proportion of histologically well to moderately differentiated cases was 76.7%. At diagnosis, 24 (55.8%) patients had palpable inguinal lymph nodes. ILD was performed in 27 patients, and positive nodes were found in 20 patients. The presence of AT was found to correlate significantly with higher pathologic stage (pT, pN, cM, and AJCC stage ≥ III), but did not correlate with age, histologic grade, or type of surgery.
Table 1
Patient characteristics
The overall survival rate was 69.8% (n = 30), and the penile cancer-related mortality rate was 14.0% (n = 12); furthermore, one patient died of unknown causes. The 3- and 5-year cancer-specific survival (CSS) rates were 79.0% and 33.0%, respectively. AJCC stage ≥ III disease and AC administration were identified as potential prognostic factors in the univariate analysis. However, in a multivariable analysis, only AJCC stage ≥ III was identified as an independent predictor of CSS (hazard ratio [HR], 10.59 [1.230–91.219]; P = 0.032) (Table 2). AT and AC administration were not significant prognosticators for CSS.
Table 2
Univariate and multivariable analyses of CSS

Thirteen (30.3%) patients developed recurrence within a median of 9.5 months (4.6–24.9). The administration of AT and AC and an AJCC stage ≥ III were significantly associated with RFS in a univariate analysis. Again, only AJCC stage ≥ III remained an independent predictor of recurrence-free survival (RFS) in the multivariate analysis (HR, 7.56 [2.254–25.373]; P = 0.001) (Table 3). Surgical treatment of the primary lesion (partial penectomy vs. total penectomy) and ILD were not significantly associated with CSS or RFS.
Table 3
Univariate and multivariable analyses of RFS

DISCUSSION
To our knowledge, this report describes the first large, multi-institution PSCC case series in Korea. As Korea represents a microcosm of the shifting demographics in rapidly developing countries, such studies are urgently needed to help characterize the populations at risk for PSCC. We found that in contrast to the high PSCC incidence rates in other Asian countries, the annual incidence rate in Korea was similar to rates in developed countries.12
The incidence of PSCC tends to increase markedly during the sixth decade of life.1314 A recent study found that the median age of patients with penile cancer in Los Angeles is younger than ages reported elsewhere in the US.1516 However, our observation of a median age of 67.0 years was similar to that in previous studies. Known risk factors for penile cancer include a history of phimosis, poor hygiene, smoking, human papilloma virus (HPV) infection (particularly HPV types 16 and 18),17 and especially, a lack of circumcision during childhood, which increases the risk by threefold. The situation of circumcision in Korea is unique. Notably, this population has undergone the most rapid increase in circumcision since the introduction of this procedure in 1945, with a circumcision rate > 100% of male births during the period from 1980–2000 was reported.18 Although the circumcision rate of 75.1% in 2012 was 16.9 percentage points lower than the 92.0% value reported in 2002, it remained much higher than rates reported in other countries.1920 Therefore, this important study not only compares the PSCC incidence rates in the Korean population over a 10-year period, but also allows a comparison of disease characteristics.
Regarding treatment for PSCC, in recent years, there has been progress in both the methods used to treat primary lesions (partial vs. radical penectomy vs. radiotherapy) and perform ILD. Most penile cancers are detected as small and distal tumors. Accordingly, the primary lesion can usually be managed by glans excision or partial penectomy with reconstruction.21 Partial penectomy is a feasible primary surgical method with similar oncological outcomes (i.e., RFS) as radical penectomy.10 In our study, we observed no significant differences in prognosis between patients treated with partial and radical penectomy. Moreover, partial penectomy for primary tumors was recommended to minimize the psychological and functional effects on patients. Accordingly, a recent report described a high rate of conservative primary treatment, with almost 60% of patients undergoing primary penis-conserving treatment, mainly radiotherapy with or without local excision.22
Previous studies emphasized an association of high-grade disease with an increased probability of lymph node metastasis.232425 However, the significant morbidity associated with ILD precludes its use as a prophylactic treatment in patients at low risk of lymph node metastases, although the modern modified approaches might reduce the complication rates.232627 In our cohort, the performance of ILD did not significantly improve patient outcomes. Several risk factors for lymph node metastases have been identified, particularly high grade and T2 disease,2627 and a positive inguinal lymph node is a significant negative prognosticator of survival in patients with PSCC.28 Consistent with a previous report, the present study identified correlations of an AJCC disease stage ≥ stage III (≥ pT1-3pN1cM0) with an unfavorable CSS and RFS.14 Therefore, our study re-confirmed the significant association of the lymph node status with survival.
No standardized AT (including AR, AC, or both) has been found to confer a survival benefit after penectomy in patients with PSCC. The use of AR may provoke lymphedema in patients who have already undergone extensive groin and pelvic dissection.29 However, AR was associated with improved survival and decreased recurrence in a recent multi-institution study of 92 patients who received AR for positive pelvic lymph nodes.7 AC has been recommended as an additional treatment option for such high-risk cases,8 as it is less likely to contribute to lymphedema and increase related morbidity. Although previous studies have used CMB and taxol, ifosfamide and cisplatin (TIP), the efficacies of these regimens remain controversial in cases involving substantial and significant morbidity and mortality. Furthermore, the curative efficacy of AC comprising CMB for advanced penile cancer is low.30 Similarly, AC with CMB did not improve the outcomes of patients with advanced PSCC in our study. The 2017 NCCN guidelines recommend 5-fluorouracil + cisplatin, which has been used historically for metastatic penile cancer, as an alternative to TIP.5 However, the efficacy of AC after penectomy will remain unclear until the results of randomized trials are obtained.
Urologists select treatment plans for rare diseases such as PSCC after referring to several guidelines, such as those published by the NCCN and EAU. However, most published studies often describe a low incidence of these diseases in Western countries, and the conclusions that can be drawn from the results are limited. Our retrospective analysis included three hospitals wherein the treatment outcomes of 43 patients with PSCC who underwent penectomy and received AT were evaluated. Therefore, our data are meaningful.
Nonetheless, the present study had several limitations. First, because of the retrospective and non-randomized study design, this study could not definitively identify the efficacy of the AT for PSCC. The present study reported that AT seems not to be effective in Asians, and a well-designed study may help to clarify whether AT is effective for Asians. Second, several factors affected the heterogeneity in the results, including the small size cohort and the decisions of multiple physicians leading to variability in surgical techniques, surveillance methods, and pathological interpretations. However, as differences in practice patterns across institutions might be reflective of a real-world setting, the conclusions of the present study may be more generalizable. Finally, although our study analyzed oncologic outcomes after penectomy and AT, we have not provided new solutions.
AJCC stage ≥ III disease, which mainly reflects positive lymph nodes, was significantly associated with survival prognoses in patients with penile cancer treated at multiple Korean institutions. However, AT did not appear to affect CSS and RFS.
 XML Download
XML Download