

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Biological disease-modifying anti-rheumatic drugs (bDMARDs) have emerged as an available therapeutic option to treat inflammatory rheumatic diseases including rheumatoid arthritis (RA) and axial spondyloarthritis including ankylosing spondylitis (AS),12 combined with and without conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs). The profiles of safety and tolerability of bDMARDs frequently used in RA and AS have been approved to be generally acceptable in clinical studies during the past several decades, although the frequency of some adverse effects including injection site reaction, infection, cardiovascular disease, and hematologic diseases has been gradually increasing.34
Some evidence has suggested that the use of bDMARDs might be related to a beneficial or adverse effect on renal function. Although there is a small number of renal abnormalities caused by bDMARDs, autoimmune renal parenchymal diseases have been reported after therapeutic uses of bDMARDs such as tumor necrosis factor (TNF) inhibitors, cytotoxic T lymphocyte antigen 4 (CTLA4)-immunoglobulin, and interleukin-6 (IL-6) receptor antagonist.56789 In contrast, some studies have shown that TNF inhibitors were not associated with worsening renal function even in patients with impaired renal function.1011 In another study, TNF inhibitors improved the annual change of estimated glomerular filter rate (eGFR) in RA patients with chronic renal disease.12 Nevertheless, debate about the effect of bDMARDs on renal function continues. There is still the possibility that bDMARDs cause the change of renal function before the occurrence of overt renal diseases in subjects with normal renal function.
In our previous analysis, bDMARDs did not influence renal function based on analysis of the interaction between TNF inhibitors and renal function in patients with RA from the Korean College of Rheumatology Biologics (KOBIO) registry from 2012 to 2016.13 However, eGFR in RA patients treated with bDMARDs gradually declined over time. Until now, there has been a lack of data related to risk factors for the change in renal function in patients after initiation of bDMARDs. Here, we retrospectively assessed the risk factors related with the change in renal function using eGFR in RA and AS patients treated with diverse kinds of bDMARDs.
METHODS
Subjects
This study retrospectively enrolled 373 patients who met the 1987 American College of Rheumatology revised classification criteria for RA14 and 139 patients who met the modified New York criteria for AS15 and who were treated with bDMARDs such as TNF inhibitors (infliximab, etanercept, adalimumab, and golimumab) or non-TNF inhibitors (abatacept and tocilizumab) from January 2007 to November 2017. At the time of initiation of bDMARDs, patients with renal insufficiency (< 60 mL/min/1.73 m2 of eGFR) or overt chronic kidney disease (CKD) with/without glomerulonephritis were not enrolled in this study. Among initially enrolled patients, 49 patients with RA were excluded in this study due to discontinuation by adverse effects or clinical improvement (n = 13), follow-up loss (n = 21), and uses of tofacitinib (Janus kinase inhibitor) or rituximab (monoclonal anti-CD20 antibody; n = 15) (Fig. 1). In addition, 31 RA patients who experienced switching between TNF inhibitors and non-TNF inhibitors were also excluded. In patients with AS, 14 patients were also not included due to discontinuation and follow-up loss. Among patients treated with bDMARDs during the same period. Patients with other rheumatic diseases including systemic lupus erythematosus, Sjogren's syndrome, psoriatic arthritis, systemic sclerosis, adult-onset Still disease, inflammatory myositis, and Behcet's disease were excluded. During bDMARDs therapy, participation of patients who experienced switching between TNF inhibitors or between non-TNF inhibitors was allowed. However, patients performed switching between TNF inhibitors and non-TNF inhibitors were also excluded.

Collection of clinical information
The study used the standardized case record form. The form was recorded by an experienced research nurse to minimize the errors and bias of the data and also verified by two researchers (Kim SK and Choe JY). The case form collected information regarding clinical and laboratory data from patients with RA and AS at the time of initiation of bDMARDs or last visit such as age, gender, disease duration, duration of bDMARD use, blood urea nitrogen (BUN), creatinine, erythrocyte sediment rate (ESR), and C-reactive protein (CRP). In RA, rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibody and disease activity score 28-ESR (DAS28-ESR) were identified at the time of initiation of bDMARDs and last visit. The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and HLA-B27 positivity was also recorded in patients with AS. csDMARDs including methotrexate, hydroxychloroquine, sulfasalazine, and leflunomide used at the time of initiation of bDMARDs were identified. We also recorded the use of corticosteroid and nonsteroidal anti-inflammatory drugs (NSAIDs).
Estimation of renal function
Renal function was estimated by the MDRD equation using the variables serum creatinine, age, and gender. The equation was as follows: eGFR (mL/min/1.73 m2) = 175 × (serum creatinine)−1.154 × (age)−0.203 × (0.742 if women).1617 The annual change of eGFR was calculated as (eGFR at last visit −eGFR at initial visit)/(time elapsed between initial and last visits).12 In this study, positive annual change in eGFR is defined as improvement of eGFR in renal function during bDMARDs treatment.
Sample size
The design of this study was to analyze the difference of dependent variable (annual change of eGFR) in a single study population with inflammatory rheumatic diseases such as RA and AS treated with bDMARDs. To explore sample size estimations in this study using the formula below, we applied 0.025 of α/2 (significance level), 0.200 of β (power), 20.000 of standard deviation and 2.500 of δ Estimated sample size was 502.3 patients. If 0.010 of drop rate in estimated sample size is applied, total sample size is 558.1 patients.

Statistical analysis
Kolmogorov-Smirnov and Shapiro-Wilk tests were used to assess the normal distribution for all clinical and experimental data, which revealed non-normal distribution of all assessed parameters. The data were described as median ± interquartile range (IQR) for continuous variables and number and percentage (%) for non-continuous variables.
The correlations between clinical variables and change in eGFR were assessed by Spearman's correlation coefficient method. Independent-sample Mann-Whitney test was used to assess the difference in the change of eGFR between two groups (men vs. women, RA vs. AS, and TNF inhibitors vs. non-TNF inhibitors). An independent-sample Kruskal-Wallis test was used to compare the change in eGFR among all bDMARDs. To determine the risk factors associated with positive annual change of eGFR, univariate linear regression was applied between clinical and laboratory parameters and change of eGFR. To the next step, multivariate linear regression analysis was performed to identify candidate variables for positive annual change of eGFR using covariates such as age, gender, disease duration, duration of bDMARDs use, BUN, creatinine, or ESR. A P value less than 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of enrolled subjects
The baseline characteristics of enrolled patients are illustrated in Table 1. There was a total of 418 patients (283 women, 67.7%) including 293 RA (261 women, 89.1%) and 125 AS (22 women, 17.6%) patients. The disease duration and duration of bDMARD use in enrolled subjects were a median of 11 years (IQR 7.0, 16.3) and 4 years (IQR 2.0, 6.0), respectively. Laboratory markers of BUN, creatinine, ESR, and CRP and disease activity indexes pf DAS28-ERS for RA and BASDAI for AS were recorded at the time of initiation of bDMARDs. Any medications currently used were also identified. TNF inhibitors including infliximab, etanercept, adalimumab, and golimumab accounted for 69.4% (n = 290) of medications. Across all patients, 56.3% of RA (n = 165) patients and 100% of AS patients (n = 125) were treated with TNF inhibitors.
Table 1
Baseline characteristics in enrolled patients treated with bDMARDs

Data are described as median ± interquartile range or number (%) and calculated by Student's t-test for continuous variables and χ2 test for categorical variables.
bDMARDs = biological disease modifying anti-rheumatic drugs, RA = rheumatoid arthritis, AS = ankylosing spondylitiss, RF = rheumatoid factor, CCP = cyclic citrullinated peptide, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, DAS = disease activity score, BASDAI = bath ankylosing spondylitis disease activity index, csDMARDs = conventional synthetic disease modifying anti-rheumatic drugs, NSAIDs = non-steroidal anti-inflammatory drugs.
aOne patient did not assess anti-CCP antibody.
Comparison of annual changes in renal function
First, the annual change in eGFR among bDMARDs in total patients irrespective of disease entity was compared (Fig. 2A). We found no significant difference in annual change in eGFR among all patients (P = 0.634). In addition, there was a similar annual change in eGFR between patients treated with TNF inhibitors and those treated with non-TNF inhibitors (−0.415 [IQR −5.378, 3.848] vs. −0.352 [IQR −8.715, 5.733], P = 0.946; Fig. 2B). In patients with RA, the change in eGFR from TNF inhibitors (n = 165) was not different from that induced by non-TNF inhibitors (n = 128) (−0.335 [IQR −4.538, 3.850] vs. −0.352 [IQR −8.715, 5.733], P = 0.475).
Fig. 2
Comparison for annual change of eGFR according to kinds of bDMARDs.
eGFR = estimated glomerular filtration rate, bDMARDs = biological disease-modifying anti-rheumatic drug, TNFi = tumor necrosis factor inhibitor.

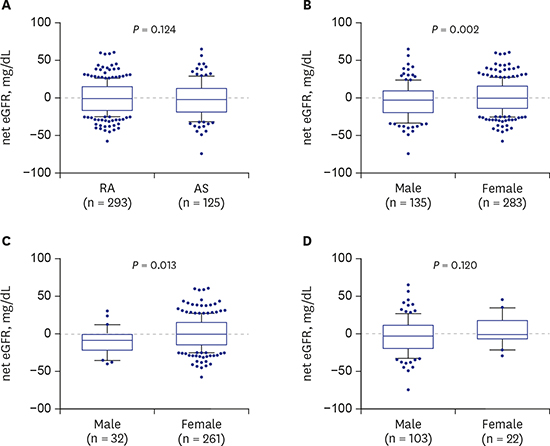
The annual change in eGFR in RA patients treated with bDMARDs was similar to that in AS patients (−0.343 [IQR −6.475, 5.173] vs. −0.654 [IQR −5.784, 3.537], P = 0.127; Fig. 3A). Fig. 3B shows that a smaller annual change in eGFR was noted in woman patients compared to man patients (−0.342, [IQR −5.745, 5.501] vs. −0.700, [IQR −8.019, 1.708], P = 0.004). In RA patients, change in renal function in women was significantly less than that in man patients (−0.335 [IQR −5.785, 5.431) vs. −2.411 [IQR −9.179, −0.252], P = 0.038; Fig. 3C). However, there was no difference in change in eGFR between man and woman AS patients (P = 0.126; Fig. 3D).

Determination of risk factor for annual change in renal function
In the assessment of association between clinical variables and change in renal function, disease duration, duration of bDMARD use, BUN, creatinine, and ESR were significantly associated with positive annual change in eGFR in the total patients (Table 2). RA patients with high BUN and creatinine levels and lower ESR level showed an increasing trend for annual change in eGFR (P = 0.010, P < 0.001 and P = 0.030, respectively). Longer disease duration and duration of bDMARD use and high creatinine level were associated with positive annual change in eGFR in AS patients (P < 0.001 of all).
Table 2
Correlation analysis between variables and positive annual change in eGFR
The statistical analysis was performed by Spearman's correlation analysis.
eGFR = estimated glomerular filter rate, RA = rheumatoid arthritis, AS = ankylosing spondylitis, bDMARDs = biological disease modifying anti-rheumatic drugs, BUN = blood urea nitrogen, RF = rheumatoid factor, CCP = cyclic citrullinated peptide, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, DAS = disease activity score, BASDAI = bath ankylosing spondylitis disease activity index.
aVariables are the baseline values at the initiation of bDMARDs except for disease duration and duration of bDMADs use.
In the determination of risk factors related to annual change of eGFR by multivariate linear regression analysis, gender, age, serum creatinine, and ESR level at baseline in total patients were considered risk factors for positive annual change in eGFR (Table 3). RA patients with younger age and lower ESR level showed an increasing tendency for annual change in eGFR (P = 0.013 and P = 0.022, respectively). Women and increased creatinine in patients with RA and AS was associated with positive annual change in eGFR.
Table 3
Determination of the risk factors for positive annual change in eGFR

The statistical analysis was performed by multivariate linear regression analysis. Data were expressed as correlation coefficient (β) and P values for selected clinical variables.
eGFR = estimated glomerular filter rate, RA = rheumatoid arthritis, AS = ankylosing spondylitis, CI = confidence interval, bDMARDs = biological disease modifying anti-rheumatic drugs, BUN = blood urea nitrogen,ESR = erythrocyte sedimentation rate.
aVariables are the baseline values at the initiation of bDMARDs except for disease duration and duration of bDMADs use.
DISCUSSION
There is growing interest in determining whether bDMARDs used in patients with RA and AS affect renal function or the development of renal diseases. One study of RA patients with CKD demonstrated that bDMARDs contributed to improvement in annual change of eGFR.12 However, it was noted that the trend toward eGFR decline is persistent over time even after administration of bDMARDs in patients with RA.1318 In other way, there is a lack of data on the effect of bDMARD therapy on change in renal function in patients with AS. In the present study, we confirmed the statistical tendency of eGFR decline in RA patients treated with bDMARDs, although bDMARD therapy has a beneficial effect on renal function in some patients. Similar to RA, this study found decreased eGFR in AS patients before and after administration of TNF inhibitors, which showed a worse change in eGFR from bDMARDs in AS than RA. Although it does not provide sufficient information on the interrelationships between bDMARDs and the change of eGFR, it may suggest that bDMARDs have at least a partial effect on renal function.
The prevalence of renal disorders or impaired renal function in RA and AS was not accurately identified. Renal diseases in 5%–50% of RA patients were variably reported dependent on study population and design,19 whereas prevalence of renal disorders in AS was lower than 10%.2021 The main causes of renal diseases have been found to be related with analgesic-induced nephropathy, chronic inflammation, secondary renal amyloidosis, and immune-mediated glomerulonephritis in patients with RA192223 and AS.202124 It was found that the use of bDMARDs irrespective of therapeutic target molecules (e.g., TNF, CTLA4, and IL-6) was associated with development of overt renal disorders in patients with various rheumatic diseases including RA, AS, Sjogren's syndrome, and psoriatic arthritis.56789 Although development of these autoimmune-mediated renal diseases after use of bDMARDs is rare, most events occurred in patients treated with TNF inhibitors. The pathogenic mechanisms for bDMARD-induced renal disorders have not been identified. But, some have suggested the hypothesis that immune complex deposition or upregulation of autoantibody and inflammatory cytokine production can produce renal tissue damage.5 Especially, it has been proposed that there is an increase in TNF inhibitors due to autoantibodies such as ANA and anti-dsDNA produced as part of the shift to the Th-2 immune system.25 Molecular mimicry by increased susceptibility to infection after TNF inhibitors was also suggested as a causative mechanism.26 In addition, development of biologics-related renal disorders has rarely been reported in relatively new bDMARDs (non-TNF inhibitors) such as abatacept and tocillizumab.89 Non-TNF inhibitors may be more favorable with regard to change in renal function than TNF inhibitors. However, a previous study demonstrated that the change in eGFR between TNF inhibitors and non-TNF inhibitors was not different in the KOBIO data from 2012 to 2016.13 In our present study, the annual change in eGFR in all patients or all RA patients was also similar among bDMARDs. In contrast, some studies have demonstrated that TNF inhibitor therapy improves renal abnormalities including proteinuria and AA amyloidosis in RA and AS.212728 Further research is needed to determine whether the type of bDMARDs affects the phenotype or severity of renal diseases.
In the present study, we estimated the risk factors affecting annual change in eGFR in patients with RA and AS. Interestingly, this study showed more eGFR decline in man patients than woman patients after bDMRAD therapy. In general, renal diseases in man subjects were more prevalent than in woman subjects.29 It is known that gender can influence the progression of renal disease including CKD.30 Sex hormones are involved in gender-specific differentiation and homeostasis of various organs including kidney, resulting in differences in renal function.31 The precise mechanism for gender-related nephrotoxicity has not been elucidated. TNF and TNF receptors may be relevant to inflammatory injury and immune regulation of kidneys, supporting a rationale for TNF blocking therapy in some nephropathy.32 Estrogen-depleted female mice significantly increased expression of the renal inflammatory cytokines including TNF and monocyte chemotactic protein-1 and tubular injury compared to estrogen-supplemented ovariectomized mice.33 Cyclosporin A was noted to result in renal TNF expression that was attenuated in female rats, but not in male rats.34 This result might suggest that the renal effect of bDMARDs might be associated with gender-specific nephrotoxicity.
In the present study, positive annual change in eGFR was observed in patients with younger age and lower ESR level at the time of initiation of bDMARDs. Aging is a crucial determinant for progressive structural change and functional decline of kidney.35 With aging, decreased production of nitric oxide (NO) and enhanced oxidative stress through decreased endothelial NO synthase was noted, suggesting that bDMARDs in patients with lower grade inflammation at younger age rather than older age are more likely to have improvement in renal function. Oxidative stress has been considered a potent therapeutic target in chronic inflammatory arthritis including RA and AS. Infliximab markedly suppressed oxidative molecule markers such as malondialdehyde + 4-hydroxyalkenals and protein carbonyls in patients with RA, AS, and psoriatic arthritis.36 Another risk factor related to annual change of eGFR in our present study was serum creatinine level at baseline. Interestingly, patients with increased creatinine level at baseline showed improvement in renal function with an increase in annual eGFR. This finding suggests the possibility of recovery of renal function after treatment with bDMARDs. Treatment with TNF inhibitors in RA with CKD was found to be associated with positive annual change in eGFR.12 In contrast, another study showed no significant difference in change in eGFR in RA with renal insufficiency.13 Considering this evidence, we suggest that bDMARDs contribute to protective effects on renal function.
There were some limitations in this study. First, this study was retrospectively performed, because regular follow-up of changes in renal function may give more confidence to the results. In this study, the use of data only from the initiation of bDMARDs to the beginning of the study can be evaluated as a weak point. However, this is thought to be overcome by using data for a relatively large number of patients. Second, the covariates related with renal function included comorbidities such as hypertension, hyperglycemia, dyslipidemia, body mass index, and lifestyle factors. These confounding factors were not considered in the analysis of this study. To overcome these issues, further prospective study including all covariates that can affect renal function will be needed in a larger study population.
Until now, there has been a lack of data about crucial risk factors for annual change in eGFR in the course of bDMARD administration. The main finding of this study is that gender might be associated with annual change in eGFR in patients treated with bDMARDs, and man patients treated with bDMARDs were found to be more susceptible to worse renal function. Further study is needed to determine if gender-specific nephrotoxicity might contribute to renal outcome in patients treated with bDMARDs.
 XML Download
XML Download