

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Percutaneous vertebroplasty (PVP) is a minimally invasive surgical treatment for patients with osteoporotic vertebral compression fracture (OVCF). This procedure can rapidly alleviate pain, enhance mobility, and stabilize the vertebrae.123 Cement extravasation is a frequent complication of vertebroplasty and is observed in 30% to 65% of OVCF patients, with venous leakage occurring in up to 24% of cases.4 Intra-cardiac cement embolism, a relatively rare but fatal complication, is mostly removed through open heart surgery.5 We report a case of a large intra-cardiac cement embolism that developed after PVP without any specific chest symptoms. The embolism was successfully removed by a combination of endovascular procedure and an inferior vena cava (IVC) exploration in this case.
CASE DESCRIPTION
A 55-year-old female presenting with lower back pain was admitted for evaluation and treatment on May 7, 2017. She had hypertension for 5 years and diabetes mellitus for 8 years. She had a history of spinal fusion (from T5 to T12) and PVP (L1 and L2) due to multiple unstable burst fractures and OVCFs. A neurological examination revealed no pathologic reflex, sensory, or motor changes in her lower extremities. In the simple lumbar radiograph, 5% and 30% height loss findings were observed in L4 and L5, respectively (Fig. 1A and B). On magnetic resonance imaging, increased signal intensity was observed at the L4 and L5 vertebrae (Fig. 1C), and bone mineral density measured by dual-energy X-ray absorptiometry showed a mean T-score of −2.9 in her lumbar vertebrae. Eventually, she was diagnosed with acute OVCF at L4 and L5 vertebral levels. Conservative treatments for 2 weeks were not effective, so PVP was performed. Under general anesthesia in a prone position, 6 mL and 7 mL of commercial polymethylmethacrylate (PMMA) (CMW3; Depuy CMW, Blackpool, UK) were injected into L4 and L5, respectively, through a transpedicular approach (Fig. 1D). The patient's lumbar pain improved after the surgery. However, the patient developed ventricular premature beats frequently during the surgery and developed atypical chest discomfort for a few minutes immediately after the surgery. No abnormalities were found in electrocardiography except that the troponin-I level was mildly elevated to 0.38 ng/mL (upper normal limit 0.04 mg/mL) and increased further to 0.81 ng/mL the next day. Then, patient developed no more chest symptoms.
Fig. 1
The diagnosis and treatment of acute osteoporotic vertebral compression fracture.
(A) A preoperative radiograph shows compression fractures at L4 and L5. (B, C) Sagittal images of lumbar spine magnetic resonance show signal change in L4 and L5 vertebral bodies. (D) A postoperative radiograph shows vertebral bodies at L4 and L5 after vertebroplasty.

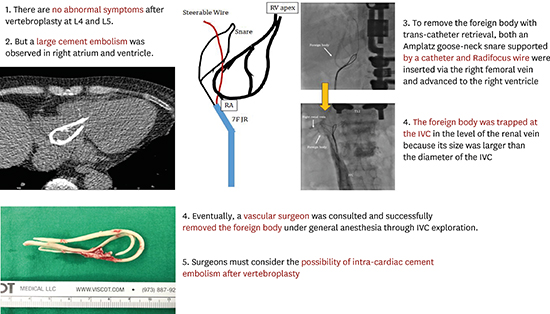
After consultation with a cardiologist, she underwent coronary angiography (CAG) and echocardiography 7 days after PVP. No stenosis or occlusion was observed in the coronary arteries but a strange radio-opacity was observed inside the cardiac brush border under fluoroscopy during CAG (Fig. 2A). Echocardiography also revealed a highly echogenic fiber-like structure inside the right atrium and ventricle (Fig. 2B). Cardiac computed tomography (CT) scan identified a large hair-pin-like foreign body with a bone-like density measured to 2.5 × 8 cm in size inside the right atrium and ventricle (Fig. 2C). Based on the radiology tests, we concluded that intra-cardiac cement embolism had occurred through the vertebral veins after PVP. After discussion in a multi-disciplinary team consisting of an interventional cardiologist, a cardiac surgeon, a vascular surgeon and an orthopedic surgeon, the patient was decided to undergo a hybrid procedure of an endovascular foreign body retrieval and a vascular surgery. During the endovascular procedure, the foreign body was caught using an Amplatz goose-neck snare (20 mm; Cook Medical, Bloomington, IN, USA) and a 35 milli-inch hydrophilic wire (Radifocus; Terumo Medical, Tokyo, Japan) supported by a 7-Fr multipurpose (MP) catheter (Cordis Corp., Milpitas, CA, USA). The snare was placed in the right atrium and the hydrophilic wire crossed the round-shape part of the foreign body and the snare loop sequentially in the right atrium. Then the snare and the wire were simultaneously withdrawn toward the MP catheter opening to fasten the foreign body between the snare loop and wire. The foreign body was successfully captured (Fig. 3A) and gently retracted from the right heart down to the IVC until there was some resistance during the retraction. The foreign body was retracted to the IVC at the level of the renal veins because its size was larger than the diameter of the IVC (Fig. 3B). Then, the foreign body was successfully removed through IVC exploration under general anesthesia without any mechanical circulatory support. The removed foreign body was identified as a solidified cement material of 2.1 × 6.3 cm (Fig. 3C). The patient did not develop any more chest symptoms after surgery, the troponin-I level returned to normal, and chest CT images revealed no remnant cement materials in the right atrium and ventricle. The patient was discharged without sequelae.
Fig. 2
The evaluation of the foreign body. (A) Fluoroscopy during coronary angiography shows radio-opaque lesion (arrowhead). (B) Echocardiography shows a highly echogenic fiber-like structure (arrows) in the right ventricle and atrium. (C) Chest computed tomography shows U-shaped high attenuating material (arrows) in the right ventricle and atrium.

Fig. 3
The removal of the foreign body. (A) The foreign body (arrowheads) was captured by the Amplatz goose-neck snare and a radifocus wire. (B) Venography shows the foreign body (arrowheads) which was trapped in the IVC at the level of the renal vein. (C) Clinical photo shows 2.1 × 6.3 cm long U-shaped cement materials which were finally removed by IVC exploration.
IVC = inferior vena cava.

DISCUSSION
Intra-cardiac cement embolism develops very rarely as a complication of PVP, but it can be fatal.6 It develops when PMMA injected through the transpedicular approach is not sufficiently polymerized, leaks into the external vertebral venous plexuses, and then migrates to the IVC. Since its size is relatively small, pulmonary embolism eventually develops once the PMMA migrates into the pulmonary artery.7 As intra-cardiac embolism can cause perforation, pericardial tamponade, and pericardial perforation,5 early recognition and prompt treatments are required.
Studies on the risk factors of intra-cardiac cement embolism have not been actively conducted, but cement leakage into the IVC is known as the only risk factor for pulmonary cement embolism.8 In previous studies on cement leakage after PVP, intravertebral cleft, cortical disruption, low cement viscosity, and high volume of injected cement have been suggested as important risk factors, whereas age, gender, fracture type, operation level, and surgical approach were reported to be insignificant.9 Cement leakage is an important complication in other spine surgeries as well as PVP. According to Janssen et al.,10 intravasal cement leakage developed in 64.8% of patients with cement-augmented pedicle screw instrumentation (CAPSI). The authors predicted that the higher frequency of intravasal cement leakage than PVP was due to the higher amount of cement injected and the higher number of levels treated, which can be considered as possible risks of PVP. In this case, the cement viscosity and volume were appropriate, but the patient's severe osteoporosis might have caused cortical disruption.
Intra-cardiac cement embolism can result in symptoms including chest pain, dyspnea, and shock,5 but in this case, no postoperative chest symptoms were observed despite the large cement embolism. Prokop et al.11 reported a surgical case performed due to cardiac perforation that developed 2.5 years after kyphoplasty without chest symptoms. It is challenging to make an early diagnosis of intra-cardiac cement embolism in the absence of early symptoms. Although rare, intra-cardiac cement embolism can be fatal. Therefore, any cement leakage must be identified early during surgery,412 patient symptoms must be closely monitored after surgery, and basic postoperative cardiac work-ups including electrocardiography and troponin-I might be required.
The endovascular procedure is frequently used to remove intra-cardiac or pulmonary foreign bodies. In previous reports, relatively small intra-cardiac cement emboli were successfully removed using endovascular procedure,1213 but there have been no reported cases of a 13 cm or larger cement embolism. In cases with a large intra-cardiac cement embolism as ours, a cardiac surgery with a median sternotomy and extracorporeal circulatory support has been most frequently performed to remove the cement material.5 Nevertheless, we tried the endovascular procedure to capture the cement material and move it to the point as distal as possible to minimize the surgical procedure. To minimize invasive procedures and obtain the best outcome, well-organized multi-disciplinary team efforts are important in case of intra-vascular foreign body embolism. In our case, we also decided to perform a hybrid procedure after a thorough discussion in a multi-disciplinary team consisting of an interventional cardiologist, a cardiac surgeon and a vascular surgeon. Although the patient had to undergo an IVC exploration, the risk of perioperative complications and prolonged hospital stay may have been reduced by a hybrid approach of the endovascular procedure and the IVC exploration.
In conclusion, large cement embolism after PVP was diagnosed and successfully removed by a combination of endovascular procedure and an IVC exploration. Surgeons must consider the possibility of intra-cardiac cement embolism after PVP. A hybrid approach of an endovascular procedure and a vascular surgery may be a reasonable treatment option to minimize the surgical procedure in cases of a large intra-cardiac cement embolism.
 XML Download
XML Download