

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the fourth most common cancer in women worldwide, with a high incidence rate (15.7 per 100,000 women) in developing countries.1 In Korea, the incidence of cervical cancer decreased from 32.9 per 100,000 women in 1993 to 15.9 per 100,000 in 2012. However, the incidence and mortality rate among young women have increased.2 Generally, locally advanced cervical cancer is treated with a combination of concurrent chemotherapy and external beam radiation therapy (EBRT), followed by intracavitary radiotherapy (ICR).3456 ICR can effectively deliver higher radiation doses to the tumor during or after EBRT and has shown significant survival benefits of ICR.7
Traditionally, ICR was planned using 2-dimensional (2D) X-ray images and was based on the Manchester system, which was standardized by the International Commission on Radiological Units (ICRU) report 38 in 1985 and subsequently by the American Brachytherapy Society in 2007. However, because this system does not consider the characteristics of individual tumors or the anatomy of individual patients, the radiation dose to the actual tumor or normal organ was difficult to predict precisely. An increasing number of institutions have started to utilize 3-dimensional (3D)-based ICR planning, based on computed tomography (CT) or magnetic resonance imaging (MRI).89 Although 3D-based ICR is expected to provide better tumor coverage and to reduce doses to normal structures, many institutions find it practically difficult to adopt 3D-based ICR or to switch from 2D to 3D-based ICR, because of reduced availability of planning software/hardware, financial constraints, and lack of optimal training/expertise.101112 A 2015 survey found that only 16% of facilities in Japan had adopted 3D-based ICR.11 Although similar data are not available for facilities in Korea, it is likely that many institutions still perform 2D-based ICR for reasons related to cost and the national insurance program.12
Our institution has been performing 3D-based ICR planning using CT images since 2015. This study compared 2D-based and 3D-based ICR treatment plans in patients with locally advanced cervical cancer. The aim of this study was to identify patients who would significantly benefit from 3D-based planning for brachytherapy and for whom 3D-based ICR should be strongly considered.
METHODS
Patient selection
This retrospective dosimetric analysis involved 20 consecutive patients with histopathologically diagnosed uterine cervical cancer who underwent curative radiotherapy with (n = 18) or without (n = 2) concurrent weekly cisplatin chemotherapy between January 2015 and October 2016. All patients underwent EBRT followed by 3D-based ICR. The median patient age was 67 years (range, 32–82 years), with one, fifteen, three, and one of these patients having International Federation of Gynecology and Obstetrics (FIGO) stages IB1, IIB, IIIA, and IIIB tumors, respectively. The mean initial tumor size was 4.98 cm (range, 2.74–6.53 cm) and the mean tumor size at the time of brachytherapy was 4.01 cm (range, 2.65–5.25 cm). Patient characteristics are detailed in Table 1.
Table 1
Patient characteristics (n = 20)

Radiotherapy technique
All patients underwent whole pelvis 3D conformal EBRT using the four-field box techniques. The prescribed dose (PD) of EBRT to the entire pelvis was 50.4 Gy in 28 fractions, using a midline block measuring 4 cm in width and 8–10 cm in height after irradiation of 45 Gy.
ICR was started within 1 week after the completion of EBRT with a MultiSource® HDR Brachytherapy Afterloader (Eckert & Ziegler BEBIG, Berlin, Germany). The ICR dose prescribed was 24 Gy in 6 fractions. Remote-controlled HDR-ICR was performed using an Ir-192 source and a CT/magnetic resonance (MR)-compatible Fletcher applicator (Eckert & Ziegler BEBIG). Each intracavitary applicator was inserted in the lithotomy position. Foley's catheters were placed in the bladder and rectum, and 7 mL of contrast medium was injected into the balloon to facilitate identification of ICRU reference points. After insertion of the tandem-ovoid applicator set, orthogonal X-ray images were taken to confirm whether it had been inserted correctly. The vagina was packed with gauze to secure the applicator firmly while increasing the distance between the radiation source and the rectum. All patients were moved to the CT room and the pelvis was scanned at 3 mm slices (LightSpeedTM; GE Medical Systems, Milwaukee, WI, USA).
All targets and organs at risk (OARs) were contoured according to the Groupe Européen de Curiethérapie and the European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) guidelines.1314 High risk clinical target volume (HR-CTV) was defined as the volume with a high probability of tumor spread, including spread to the entire cervix and presumed extra-cervical tumor extension at the time of brachytherapy. Intermediate risk clinical target volume (IR-CTV) was defined as the volume with a significant probability of microscopic tumor spread, encompassing the HR-CTV, with a safety margin of 5–15 mm, as well as the initial tumor.14 After completion of CT simulation and contouring of target volumes and OARs (rectum, bladder and sigmoid colon), brachytherapy was planned using the HDR plus 3.0.7 (sonoTech GmbH, Neu-Ulm, Germany) treatment planning system (Fig. 1). The procedure was optimized by manually adding or removing stopping positions and adjusting the dwell times at each given source position. The system graphic optimization tool was used to optimize dose distribution by dragging/adjusting isodose lines. Dose-volume histogram (DVH) parameters for HR-CTV, rectum, bladder, and sigmoid colon were calculated.
Fig. 1
Examples of the dose distribution in reconstructed sagittal CT images. (A) 3D-optimized plans and (B) conventional 2D plans. Dashed lines indicate the HR-CTV (red), rectum (orange), bladder (blue), and sigmoid colon (green). The 125%-, 100%-, and 90%-isodose lines are shown as orange, red, and dark blue solid lines, respectively.
3D = 3-dimensional, 2D = 2-dimensional, CT = computed tomography, HR-CTV = high risk clinical target volume.

We focused primarily on the D90 value when interpreting the target coverage. HR-CTV D90 is the minimum dose covering 90% of the HR-CTV. HR-CTV D90 was more stable than HR-CTV D100 due to decreased sensitivity to variations in contouring. The dose delivered to the OAR was evaluated using D2cc and Dmax. D2cc is the minimum dose in the highest irradiated 2 cc area, and Dmax is the maximum point dose in the OAR. All values were obtained from the cumulative DVH analysis.
The treatment plan was optimized to meet the following requirements based on trial and improvement approach: 1) HR-CTV D90 should be 100% of the PD, 2) D2cc were 75 Gyα/β=3 (80% of PD) for the rectum and sigmoid colon and 80 Gyα/β=3 (94% of PD) for the bladder. The α/β ratio is defined as the dose at which cell deaths due to the linear and quadratic components are equal. It is derived from the cell survival curve after irradiation.15 An α/β value of 3 was used for late-responding tissues and 10 was used for early-responding tissues or tumors. Total EBRT and ICR dose was calculated by biologically equivalent dose in 2 Gy fractions (EQD2) with α/β = 10 for tumors and α/β = 3 for OARs.
Comparison of 2D- and 3D-based ICR plans
On the basis of the orthogonal X-ray images that were acquired to verify the positions of the tandem and ovoids, re-planning was performed to generate new 2D-based ICR plans.1617 The manual optimization of the 2D plans started with the standard loading patterns and dwell times. The minimum interval of dwell position was 5 mm. Tandem optimization points were approximately 1 cm inferior to the first position (superior-most) and allowed to pass over the surface point of the vaginal appliance. The dwelling times and positions were optimized to minimize the dose to ICRU rectal and bladder points (< 80% of PD). The ICRU rectal point was defined on the lateral film as 5 mm behind the posterior vaginal wall. The ICRU bladder point was located at the most posterior part of the Foley catheter balloon. A dose of 4 Gy was prescribed to point A. Point A was specified at 2 cm superior to the flange and 2 cm lateral from the axis of the intrauterine tandem. After completion of 2D-based ICR planning, several dosimetric parameters were acquired from the DVH and compared to those from the 3D-based plan. To investigate the relationship between tumor size and tumor coverage, the longest diameter of the tumor was measured in the axial slices of the initial MRI and the MRI taken at the time of brachytherapy.
Statistical analysis
Differences in DVH parameters were assessed using paired t-test, with a two-sided P value < 0.05 considered statistically significant. The bivariate correlation was used to assess the relationship between variables, and Pearson's correlation coefficient was computed for these relationships. Scatter diagrams were drawn to visually represent these relationships. All statistical analyses were performed using SPSS software (Version 21.0 for Windows; SPSS Inc., Chicago, IL, USA).
RESULTS
Comparison of 2D- and 3D-based ICR plans
The mean HR-CTV was 46.3 cm3 (range, 10.6–93.6 cm3) and the mean IR-CTV was 132 cm3 (range, 67–217.3 cm3). The mean value of the target coverage parameters (HR-CTV D90 and D100, and IR-CTV D90 and D100) and the mean rectal, bladder, and sigmoid D2cc are shown in Table 2. The target coverage (for both HR-CTV and IR-CTV) was better in the 3D-based than in the 2D-based plan. The HR-CTV D90 was 88.4% in 2D-based plans and 97.7% in 3D-based plans, although the difference was only marginally significant (P = 0.068). The IR-CTV D90 and D100 were statistically significantly better in 3D-based plans. Although the rectal D2cc was lower in the 2D-based plans, the sigmoid D2cc was higher in the 2D-based plans.
Table 2
Overall dosimetric comparisons between 2D- and 3D-based planning

Target coverages by tumor size
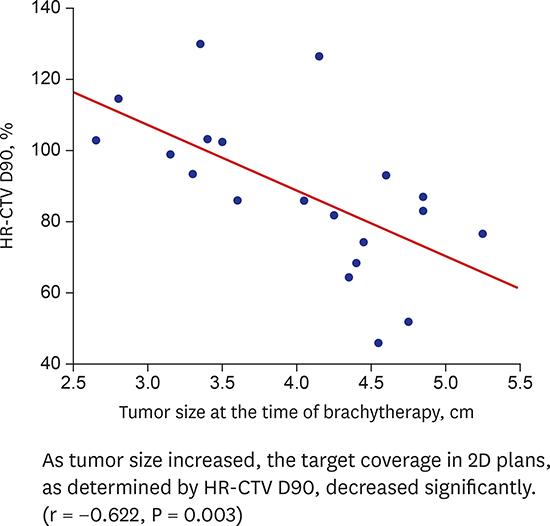
Table 3 shows target coverage in both the 2D- and 3D-based plans of tumors ≤ 4 cm and > 4 cm, as measured by MRI at the time of brachytherapy. Tumor coverage by both plans did not differ in patients with tumors ≤ 4 cm at the time of brachytherapy, with all tumor coverage parameters (HR-CTV D90 and D100, and IR-CTV D90 and D100) being similar for the 2D- and 3D-based plans. In contrast, tumor coverage by 3D-based plans was better in patients with tumors > 4 cm. Mean HR-CTV D90 was significantly greater for 3D than 2D plans (96.0% vs. 78.1%, P = 0.017), as were HR-CTV D100, IR-CTV D90, and IR-CTV D100. As tumor size increased, the target coverage in 2D plans, as determined by HR-CTV D90, decreased significantly (r = −0.622, P = 0.003; Fig. 2).
Table 3
Difference in tumor coverage between 2D- and 3D-based planning by tumor size at the time of brachytherapy

Fig. 2
Scatter diagram showing tumor coverage (HR-CTV D90) according to tumor size at the time of brachytherapy in the 2D-based plans (r = −0.622, P = 0.003).
2D = 2-dimensional, HR-CTV = high risk clinical target volume.
Table 4 shows the target coverage in both plans based on initial tumor size, before the start of EBRT. Tumor coverage by both 2D and 3D plans did not differ in patients with initial tumors ≤ 5 cm in size. In contrast, target coverage of tumors > 5 cm was lower with 2D- than 3D-based plans, although the statistical significance was not as great as for tumor size measured at the time of brachytherapy. Fig. 3 shows also the correlation between the initial tumor size and HR-CTV D90 in the 2D plans (r = −0.404, P = 0.077).
Table 4
Difference in tumor coverage between 2D- and 3D-based planning by tumor size at the time of diagnosis

OAR doses
We found that the rectal D2cc dose was lower in conventional 2D than in 3D plans (59.2% PD vs. 71.1% PD) (Table 2), due to differences in dose constraints during the planning procedures (< 80% PD to the rectal reference point in 2D plans versus < 80% PD to rectal D2cc in 3D plans). Fig. 4 shows that the correlations between the ICRU rectal point dose and rectal Dmax (r = 0.643, P = 0.002) and D2cc (r = 0.560, P = 0.010) doses in 2D plans were statistically significant. The mean ICRU point dose of 70% PD could be converted to 82.7% PD (range, 52.2% – 110.2% PD) at Dmax and to 59.2% PD (range, 39.2%–78% PD) at D2cc. The sigmoid D2cc was higher in 2D than in 3D plans (67.5% PD vs. 58.8% PD) because the dose to the sigmoid colon could not be considered in 2D-based plans. Therefore, six of the 20 (30%) patients would have received higher doses than the dose constraints (80% PD sigmoid).

DISCUSSION
Traditionally, brachytherapy to treat cervical cancer has involved a 2D planning method based on orthogonal X-ray images.18 In particular, 2D planning based on the Manchester system is very simple, has sufficient reproducibility for worldwide use, and is still used by many institutions. However, this method has several limitations because it sets the dose for a specific point regardless of the patient's anatomy or tumor characteristics.19 This problem may be solved by 3D image-based brachytherapy using CT or MRI, as recommended by GEC-ESTRO.10 However, some institutions may be unable to adopt a 3D-based brachytherapy planning system because of the reduced availability of planning software/hardware, financial constraints, and the lack of optimal training/expertise.101112 These problems are likely much more serious in South Korea, as many institutions are reluctant to implement 2D-based brachytherapy because it may not be covered by the national insurance system.12 Comparing the tumor coverage and OAR protection determined by 3D- and 2D-based ICR may help identify who would greatly benefit from 3D-based ICR.
Except for three patients, whose tumors were very close to the rectum, the HR-CTV D90 in all patients was higher than 95%. In 2D-based planning, however, the mean HR-CTV D90 value was 88.4%, or about 10% lower, indicating that 2D plans result in much less tumor coverage than 3D plans, and that the former have large variability.
This finding, was not applicable to patients with small tumors (≤ 5 cm initially or ≤ 4 cm at the time of brachytherapy); in these patients, 2D- and 3D-based ICR provided similar tumor coverage. However, in patients with larger tumors (> 5 cm initially or > 4 cm at the time of brachytherapy), the tumor coverage was significantly poorer in 2D- than in 3D-based plans.
Similar results were reported in a study comparing tumor coverage and OAR protection, as determined by MRI-based 3D and 2D plans in eight patients.19 That study found that 2D-based plans may represent overtreatment of small tumors but insufficient dose distribution for larger tumors. However, the number of patients was too small to determine a cut-off value or the statistical significance of tumor sizes.19
In our study, we selected the cut-off value to determine which patients needed 3D-based ICR. At the time of ICR, 4 cm was selected based on the receiver-operating characteristic (ROC) curve analysis. Tumors larger than 4 cm at the time of ICR could benefit from 3D-based ICR with 90.9% sensitivity and 77.8% specificity. The area under the curve (AUC) value was 0.909. On the other hand, the initial tumor size of 5 cm was selected based on the study by Potter et al.20 because the ROC curve showed no significant result. A retrospective evaluation of 145 cervical cancer patients treated by EBRT and ICR found that the local control rate prior to implementation of MRI-based 3D ICR in 2001 was 64% in patients when the initial tumors were larger than 5 cm. However, following the implementation of MRI-based 3D ICR, the local control rate increased to 82% (P = 0.09).20
When evaluating OAR protection, we found it difficult to identify high risk patients who could benefit from 3D-compared with 2D-based ICR. In patients whose ICRU rectal point was close to achieve proper tumor coverage with 2D-based plans, it was difficult to achieve proper tumor coverage by 3D-based plans. In our study, the rectal D2cc was significantly lower in conventional 2D than in 3D plans, likely because the dose constraints for the rectum were the same in both plans, despite the dose constraints in the 2D and 3D plans being point- and volume-based, respectively. Because we observed a considerable correlation between 2D- and 3D-based rectal doses in our study, tumor coverage in 2D plans may be increased by using different rectal dose constraints.
An evaluation of ICR plans for 229 patients found a significant correlation between ICRU rectal point and D2cc, using the equation D2cc = 0.902 × ICRU point dose + 0.984, although ICRU may underestimate D2cc.21 In contrast, an analysis of ICR plans for 20 patients found that the ICRU bladder point could be a reasonable surrogate for D2cc, whereas the ICRU rectal point could not.22 Taken together, these studies yield conflicting results about whether the 2D-based ICRU rectal point is sufficiently reliable for OAR protection. In addition, conflicting results were observed in studies evaluating whether rectal dose was lower with 3D-based ICR or with 2D-based ICR.2324
The main advantage of 3D-based ICR was its ability to evaluate and reduce the dose to the sigmoid colon. The sigmoid point was found to receive a significantly higher dose than the rectal point, with 3D image-based planning of ICR being necessary to document and to reduce sigmoid doses.25 Additional rectal and sigmoid points, other than ICRU points, were required to identify the most commonly appearing high-dose regions in the rectum and sigmoid colon. The mean ICRU and additional distal, proximal, and sigmoid point doses were 486, 527, 401, and 838 cGy, respectively, with the sigmoid point dose being the highest.25
Although there have been several reports suggesting the dosimetric and clinical benefits of 3D-based ICR, to date no dosimetric studies have suggested a specific tumor size criteria for 3D-based ICR. Large tumor size criteria at the time of diagnosis or brachytherapy in which HR-CTV D90 is significantly reduced by approximately 20% in 2D-based ICR may be used as a simple factor in considering patients requiring 3D-based ICR in clinical practice.
However, this study had several limitations. First, the number of patients was small, limiting its statistical power. Additional studies, involving larger numbers of patients, are needed to confirm the cut-off values. Second, since this was a dosimetric study, it is unclear whether its results will lead to clinical benefits. Long-term follow up is therefore needed. Third, because we only included patients who underwent 3D-based ICR based on CT images, caution should be exercised when applying our results to 3D-based ICR planning based on MRI images. Although the GEC-ESTRO suggested that MRI could offer superior tissue contrast, and studies have shown that MRI results in superior dosimetry compared with CT in the planning of cervical cancer brachytherapy, routine MRI in most countries is limited because of the lack of availability and because of financial constraints.
In conclusion, 3D-based ICR could improve tumor coverage while satisfying dose constraints for OARs during brachytherapy in patients with cervical cancer. 3D-based ICR may offer better tumor coverage than 2D-based ICR, especially in patients with tumors > 5 cm initially or > 4 cm at the time of brachytherapy. Therefore, patients with large cervical masses should undergo 3D-based ICR or be referred to centers where 3D-based ICR is available.
 XML Download
XML Download