

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary chronic total occlusion (CTO) is found in up to 30% of diagnostic catheterizations in patients with coronary artery disease.12 Recently, CTO recanalization has been attempted in many of these cases with advanced endovascular equipment and techniques. However, 20%–35% of CTO cases are not revascularized using these percutaneous coronary intervention (PCI) methods,3456 primarily due to ongoing controversy on the relative value and risks of CTO recanalization; these patients are thus managed conservatively without a revascularization strategy.26 Consequently, optimal medical therapy and risk stratification in CTO patients not revascularized is important. The clinical benefit of statin use in ischemic heart disease is well established and current American College of Cardiology Foundation/American Heart Association guidelines recommend statin as a first-line treatment in stable ischemic heart disease patients to control lipid profile (class I).7 However, the beneficial effects of statin therapy have not been established in sub-groups with coronary CTO. Therefore, we investigated the association of statin therapy with clinical outcomes and risk factors of cardiac death in stable CTO patients without revascularization.
METHODS
Study population
Between March 2003 and February 2012, a total of 2,024 consecutive patients were enrolled in the retrospective Samsung Medical Center CTO registry. The inclusion criteria for the registry were: 1) at least one CTO detected on diagnostic coronary angiography and 2) symptomatic angina and/or a positive functional ischemia study. Exclusion criteria included: 1) previous coronary artery bypass graft (CABG) surgery, 2) a history of cardiogenic shock or cardiopulmonary resuscitation, and 3) ST-segment elevation acute myocardial infarction (MI) during the preceding 48 hours. Whether to perform PCI of CTO lesion was left to the discretion of the operators, the procedure was based on clinical evidence or functional information of viability and ischemic burden in the territory supplied by the CTO as well as patient's functional performance. In this registry, we sorted patients with CTO without revascularization according to initial treatment strategy. Among these patients, we selected the study population after applying additional exclusion criteria: 1) in-hospital death, 2) patients who initially presented with acute coronary syndrome (ACS), and 3) patients with incomplete medication data.
Detail of medical treatment
Medical treatment included antiplatelet medication, aggressive lipid-lowering therapy with statin, β-blocker, calcium channel blocker, renin angiotensin system blockade, nitrates and diuretics. Patients received antiplatelet therapy with either 81 to 325 mg aspirin daily or 75 mg clopidogrel daily in the absence of reasonable contraindications. Patients were taking one or more anti-anginal medications, including a long-acting β-blocker, calcium channel blocker or isosorbide mononitrate, alone or in combination, along with either an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker and statins as standard secondary prevention. The medication regimens of all patients were considered optimal, with doses based on heart rate, blood pressure, and symptoms in the absence of justifiable relative contraindications.
Data collection
Clinical, angiographic, procedural, and outcome data were collected using a web-based reporting system. Additional information was obtained by reviewing the medical records or by telephone contact, if necessary. All baseline and procedural cine-coronary angiograms were reviewed and analyzed quantitatively at the angiographic core laboratory (Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea) with an automated edge-detection system (Centricity CA 1000; GE, Waukesha, WI, USA) using standard definitions.
Study outcomes and definitions
A CTO lesion was defined as the obstruction of a native coronary artery with a thrombolysis in myocardial infarction (TIMI) flow grade 0 for an estimated duration longer than three months. Duration was estimated based on the interval from the last episode of ACS, or in patients with no history of ACS, from the first episode of exertional angina consistent with the location of the occlusion or previous coronary angiogram.389 The primary outcome was cardiac death during follow-up. The secondary outcomes were all-cause death, non-fatal MI, any coronary revascularization and major adverse cardiac and cerebral events (MACCE). All-cause deaths were considered to be of cardiac origin unless a definite non-cardiac cause could be established. MI was defined as recurrent symptoms with new electrocardiographic changes compatible with MI or cardiac markers at least twice the upper limit of normal.10 Revascularization was a composite of target vessel revascularization and non-target vessel revascularization treated with PCI or CABG. MACCE was a composite of cardiac death, all-cause death, non-fatal MI, cerebrovascular accident (CVA) or any coronary revascularization. Renal insufficiency was defined as an estimated glomerular filtration rate (eGFR) lower than 60 mL/min/1.73 m2 (using the Modified Diet in Renal Disease equation) at initial presentation. The extent of collateral flow was assessed according to the validated Rentrop classification scale and reviewed by experienced interventional cardiologists blinded to patient data as described in previous studies.1112 We considered Rentrop grade 2 or 3 collateral flow to have high collateral flow. SYNergy between Percutaneous Coronary Intervention with TAXus and Cardiac Surgery (SYNTAX) score was calculated based on study site and angiographic core laboratory blinded to patient data.13
Statistical analysis
All statistical analyses were performed using the intention-to-treat principle. Comparisons for continuous variables were made using the t-test or Wilcoxon rank-sum test when applicable. Categorical data were tested using the χ2 test. Survival curves were constructed using Kaplan-Meier estimates and compared with the log-rank test. The Cox proportional hazard model was used to compare the risks of adverse cardiac events between the statin and non-statin groups. Propensity scores were estimated using multiple logistic regression analysis. Full non-parsimonious models were developed and included variables in Table 1. Cox regression analysis using pairs matched via a greedy algorithm and the nearest available pair-matching method among patients with an individual propensity score was also performed to evaluate reductions in outcome risk. The covariate balance achieved by matching was assessed by calculating the absolute standardized differences in covariates between the two groups. An absolute standardized difference < 10.0% for the measured covariate suggests appropriate balance between the groups. In the propensity score-matched population, continuous variables were compared with a paired t-test or the Wilcoxon signed-rank test, as appropriate, and categorical variables were compared with the McNemar's or Bowker's test of symmetry, as appropriate. The reduction in outcome risk was compared with the stratified Cox regression model using prognostic covariates with an absolute standardized difference > 10.0% used as the criterion for inclusion of variables in the multivariate models, because the combination of regression adjustment in matched samples generally produces the least biased estimate. Cumulative incidence rates of individual clinical outcomes and composite outcomes were estimated using the Kaplan-Meier method and compared using the paired Prentice-Wilcoxon test. Statistical analyses were performed with SAS 9.2 (SAS Institute Inc., Cary, NC, USA). All tests were two-tailed, and P values < 0.05 were considered statistically significant.
Table 1
Baseline and angiographic characteristics of patients with CTO without revascularization strategy

Values are presented as mean ± standard deviation or number (%).
CTO = chronic total occlusion, MI = myocardial infarction, PCI = percutaneous coronary intervention, LVEF = left ventricular ejection fraction, LAD = left anterior descending artery, ACE inhibitor or ARB = angiotensin-converting enzyme inhibitor or angiotensin receptor blockers, SYNTAX = SYNergy between Percutaneous Coronary Intervention with TAXus and Cardiac Surgery, LDL = low-density lipoprotein.
aThe 483 had an assessment of total cholesterol, excluded in propensity score matching; bThe 384 had an assessment of low-density lipoprotein, excluded in propensity score matching.
RESULTS
Among the 2,024 registered patients, 664 patients had CTO without revascularization as an initial treatment strategy; 113 of these patients were excluded based on additional exclusion criteria. Study population consisted of a single vessel disease with single CTO lesion (342 [62.1%] patients), multi-vessels disease with single CTO lesion (131 [23.7%]) and multi-vessels disease with multi CTO lesions (78 [14.2%]). Statin were prescribed at discharge to 369 patients (statin group; 67.0%) and not prescribed to 182 patients (non-statin group; 33%) (Fig. 1).
Fig. 1
Schema of group distribution in the registry.
CTO = chronic total occlusion, ACS = acute coronary syndrome.

Baseline characteristics
Baseline clinical characteristics according to use of statin are shown in Table 1. Compared with patients in the non-statin group, patients in the statin group had a higher prevalence of hypertension, prior PCI and use of aspirin, β-blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. The prevalence of left anterior descending artery CTO and current smoking were more frequent in the non-statin group. After performing 1:1 individual matching without replacement using propensity scores for the entire population, 148 matched patient pairs were created. The c-statistic of the propensity score model was 0.77.
Clinical outcomes
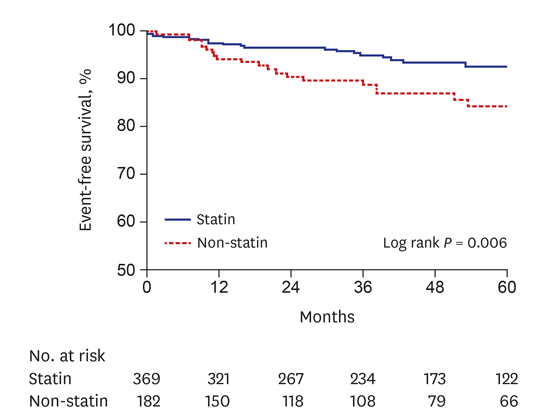
The median overall follow-up duration was 45.7 months (interquartile range [IQR]: 19.9–70.5 months); median follow-up was 46.1 months (IQR: 27.7–69.7 months) in the statin group and 43.6 months (IQR: 15.4–71.2 months) in the non-statin group. Table 2 and Fig. 2 show cumulative clinical outcomes in the overall study population and unadjusted hazard ratios (HRs) between the two groups. In Cox regression analysis, as compared with the non-statin group, the statin group had a lower incidence of cardiac death (statin vs. non-statin, 6.0% vs. 13.2%; unadjusted HR, 0.44; 95% confidence interval [CI], 0.24–0.78; P < 0.001), all-cause death (14.9% vs. 28.0%; HR, 0.51; 95% CI, 0.35–0.75; P < 0.001). There were no significant differences in the incidence of non-fatal MI, revascularization, CVA and MACCE between the statin and non-statin group. After 1:1 propensity-score matching, there were 31 cardiac deaths with a median follow-up of 44.0 months in the matched population. The statin group still had a lower incidence of cardiac death (6.1% vs. 14.9%; adjusted HR, 0.41; 95% CI, 0.18–0.85; P = 0.022), all-cause death (15.5% vs. 28.4%; adjusted HR, 0.52; 95% CI, 0.31–0.88; P = 0.010), and MACCE (26.4% vs. 40.5%; adjusted HR, 0.66; 95% CI, 0.43–0.98; P = 0.043) (Table 2 and Fig. 2).
Table 2
Clinical outcome between statin and non-statin group in total and propensity matched population with CTO without revascularization

Values are presented as number (%).
CTO = chronic total occlusion, HR = hazard ratio, CI = confidence interval, MI = myocardial infarction, CVA = cerebrovascular accident, MACCE = major adverse cardiac and cerebral events, ACE inhibitor or ARB = angiotensin-converting enzyme inhibitor or angiotensin receptor blockers.
aAdjusted covariates include male, aspirin, ACE inhibitor or ARB.

Independent predictors of cardiac death
Crude associations between clinical factors and cardiac death were determined using a Cox regression analysis model. Variables associated with cardiac death in univariate analysis were then entered into a multivariate Cox regression analysis model in a step-wise fashion and retained in the model if P < 0.10. The independent predictors of cardiac death in patients with CTO without revascularization were age > 70 years, renal insufficiency, prior MI, left ventricular (LV) ejection fraction < 40%, proximal-to-mid location of the CTO lesion and no use of statin (Table 3).
Table 3
Independent predictor of cardiac death in patients with CTO without revascularization

CTO = chronic total occlusion, HR = hazard ratio, CI = confidence interval, MI = myocardial infarction, LVEF = left ventricular ejection fraction, SYNTAX = SYNergy between Percutaneous Coronary Intervention with TAXus and Cardiac Surgery.
aAdjusted covariates include age > 70 years, renal insufficiency, prior MI, LVEF < 40%, proximal to mid location of CTO, SYNTAX score, statin use, spironolactone use.
DISCUSSION
In the present study, we investigated the association between statin therapy and clinical outcomes and sought to identify clinical factors that predict clinical outcomes in stable coronary CTO without revascularization. The major findings of this study were as follows: 1) Statin therapy was associated with a low risk of cardiac death, and this result was maintained in propensity-matched populations. 2) Independent predictors of cardiac death were age > 70 years, renal insufficiency, prior MI, LV ejection fraction < 40%, proximal-to-mid location of the CTO lesion and no use of statin.
In the management of patients with CTO, we consider many issues, such as individualized risk/benefit analysis; clinical, angiographic and technical considerations; and the associated comorbidities of patients.141516 However, 20%–35% of attempted recanalization of CTO cases are unsuccessful and canalization is never attempted in a substantial portion of cases.617 Therefore, a considerable number of patients with CTO are managed conservatively with optimal medical treatment, and risk stratification and treatment strategy may thus have important roles in the management of CTO.
Many studies have discussed the benefits of statin use as the optimal medication for reducing cardiovascular events including recurrent ischemia and cardiovascular mortality in patients suffered from ACS and stable ischemic heart disease.18 In the Scandinavian Simvastatin Survival Study and Heart Protection Study, statin therapy showed significant benefits with regard to cardiovascular mortality in patients with stable ischemic heart disease.1920 However, in patients with CTO without revascularization, limited data exist regarding clinical outcomes according to statin therapy. In the present study, we focused on a sub-group population of stable coronary artery disease with CTO without revascularization and demonstrated that statin therapy at discharge was associated with lower cardiac mortality in overall and propensity-matched populations. These results are consistent with a previous randomized trial and meta-analysis, which indicated that lowering low-density lipoprotein (LDL) cholesterol with statin therapy improved coronary heart disease mortality rates.1821 One plausible explanation of this finding is that optimal medical therapy including statin therapy for non-CTO vessels may have affected clinical outcomes. CTO is a fixed ischemic burden and usually non-CTO vessels serve as a donor for collateral circulation. The beneficial effects of statin therapy for non-CTO vessels may have a prognostic benefit in CTO patients without revascularization. In previous studies, the prognostic benefit of a well-developed collateral blood supply was demonstrated in various clinical settings.2223 Beyond decelerating the progression of atherosclerosis through the lipid-lowering effect, statins have anti-arrhythmic properties. In some studies, use of statin was associated with a reduced risk of cardiac death or ventricular arrhythmia in patients with atherosclerotic heart disease.2425 In the present study, statin therapy was associated with a low risk of non-cardiac death as well and this partly contributed to the low risk of all-cause death. This can be explained by the fact that statins exhibit a number of pleiotropic effects in the setting of non-cardiovascular events. Pleiotropic effects of statin include enhancement of anti-oxidant properties, inhibition of inflammatory response, immunomodulatory activity, and a chemopreventive effect in some site-specific cancers.2627
In the present study, clinical predictors of cardiac death in patients with CTO without revascularization were explored. In particular, among the clinical predictors, age > 70 years, renal insufficiency, prior MI, LV dysfunction and proximal location of the CTO lesion were independently associated with a high risk of cardiac death. On the other hand, use of statin was associated with lower cardiac death in CTO without revascularization. Age > 70 years and renal insufficiency are established risk factors for adverse clinical outcomes in stable ischemic heart disease.282930 Likewise, several previous studies demonstrated that LV dysfunction and prior MI were associated with poor clinical outcomes.313233 A proximal-to-mid location of CTO in the coronary artery was associated with a higher risk of cardiac death. This location represents a greater myocardial ischemia burden compared to a distal location. The relationship between myocardial ischemia burden and mortality was reported in previous several trials.3435 Verification and risk stratification of clinical factors might be helpful in the selection of patients who should undergo revascularization and could provide better information regarding long-term prognosis in CTO without revascularization.
There were some limitations to the present study. First, the study design was nonrandomized, retrospective, and observational, which may have significantly affected the results owing to confounding factors. Although we performed propensity score matching analysis to adjust for potential confounding factors, we were not able to correct for unmeasured variables. In particular, because of the retrospective analysis from the chart review, we did not have information of the reasons for making the decision not to use statin. We can suspect that it would be affected by physician preference or personalized patient characteristics, such as baseline lipid profile, underlying history of drug side effect and expected complication or compliance of medication. Second, in our study, all-cause deaths were considered to be of cardiac origin unless a definite non-cardiac cause could be established. But, we could not identify specific cause of cardiac death because of retrospective analysis with our registry. Third, the database lacked data on low-density lipoprotein cholesterol level. However, the recent American College of Cardiology/American Heart Association treatment of blood cholesterol guidelines did not mention a specific LDL cholesterol treatment target level.21 Fourth, data were not available on the intensity or duration of statin therapy. Finally, we have no information on accurate documentation of viability or ischemic burden in the territory supplied the CTO lesion or compliance with statin therapy over time.
In conclusion, statin therapy at discharge may be associated with a reduction in long-term cardiac mortality in patients with stable CTO without revascularization. Further randomized controlled trials evaluating the efficacy of statin therapy are needed in order to confirm the findings of the present study.
 XML Download
XML Download