

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Takayasu arteritis (TA) is a chronic vasculitis that mainly involves the aorta and its major branches. The renal artery is most commonly involved in childhood-onset TA (c-TA) as renal arterial stenosis (RAS), which presents with the so-called renovascular hypertension (RVH). RVH is usually clinically silent in children, which renders early diagnosis of c-TA a daunting challenge to pediatricians. What further confounds this issue is diverse involvement of many arteries, which may cause protean clinical manifestations. We describe a 14-year-old girl, with c-TA and childhood-onset moyamoya syndrome (c-MMS), presenting with stenosis of bilateral renal and cerebral arteries, which were treated stepwise with endovascular and surgical revascularization. Caveats in the diagnosis and management of c-TA will be briefly discussed.
CASE DESCRIPTION
On October 29, 2009, a 14-year-old girl was referred to our hospital with the chief complaint of systemic hypertension (200/126 mmHg), which was found incidentally by a routine check-up of blood pressure at a local pediatric clinic. At the outpatient clinic, she weighed 76 kg and her height was 165 cm. Radial and femoral pulses were bounding. Electrocardiogram, chest radiogram, and echocardiography were non-conclusive for a definite diagnosis. Hemoglobin was 10.6 g/dL, erythrocyte sedimentation rate (ESR) 54 mm/hr, renin 41.2 pg/mL, renin activity 6.22 ng/mL/hr, and aldosterone 232 pg/mL. Abdominal computerized tomography angiography (CTA) revealed the culprit to be bilateral ostial RAS (Fig. 1A). Under the impression of c-TA involving bilateral renal arteries, endovascular revascularization was deferred after control of active inflammation by corticosteroid (prednisolone; 2 mg/kg/day for 2 months followed by 1 mg/kg/day for 2 months).
Fig. 1
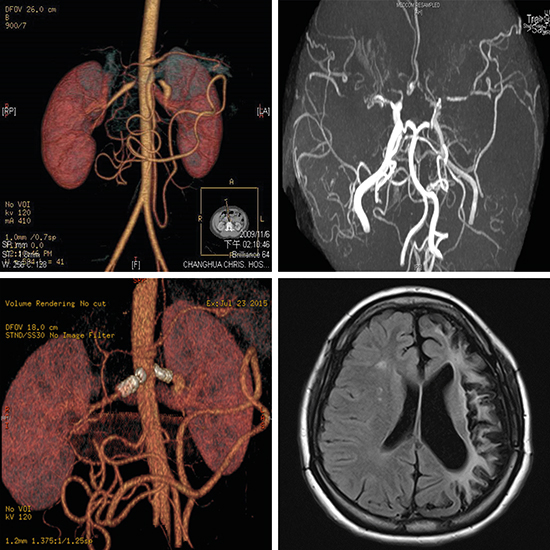
Images of the renal artery and brain. (A) Abdominal CTA showed bilateral ostial renal artery stenosis (white arrows). (B) Brain MRI showed abnormal signal intensity changes over bilateral subcortical and periventricular white matter regions of both frontoparietal lobes (white arrows). (C) Diffusion weighted imaging showed increased signal (white arrows). (D) Apparent diffusion coefficient mapping showed decreased signal (white arrows) due to restrictive diffusion following cerebrovascular ischemia or infarction. (E) Brain MRI showed prominent perforating arteries (white arrows) over bilateral basal ganglia. (F) Brain magnetic resonance angiography showed obliteration or stenosis of bilateral middle cerebral arteries (white arrows) and left anterior cerebral artery and a classic picture mimicking a puff-of-smoke (moyamoya) which indicates collateral circulations (black arrows). (G) Abdominal CTA showed stents in situ of bilateral renal arteries, without fracture, collapse, or migration. (H) Brain MRI showed residual left encephalomalacia.
CTA = computerized tomography angiography, MRI = magnetic resonance imaging.

Four months later, endovascular revascularization was performed. By cardiac catheterization, ascending aortic pressure was 195/126 mmHg. Renal angiography showed bilateral ostial RAS, with a diameter of 1.99 and 2.13 mm at the ostium of the right and left renal arteries, respectively. Heparin (5,000 units) was administrated beforehand. After stent implantation (SI) (7 × 17 mm, Express Vascular™ LD; Boston Scientific, Marlborough, MA, USA) and percutaneous transluminal renal angioplasty (PTRA) (6.0 mm × 2.0 cm, Monorail Ultrasoft™ SV; Boston Scientific, Maple Grove, MN, USA), the ostium of the right renal artery was dilated to 4.11 mm. Blood pressure dropped to 128/86 mmHg. Unfortunately, dizziness, amaurosis fugax, dysarthria, right hemiparesis, paresthesia, and facial palsy were noted one week following the procedure. Brain magnetic resonance imaging (MRI) showed abnormal signals over bilateral subcortical and periventricular white matter regions of frontoparietal lobes (Fig. 1B-D), and prominent perforating arteries over bilateral basal ganglia (Fig. 1E). Brain magnetic resonance angiography (MRA) showed stenosis of bilateral middle cerebral arteries (MCAs) and the left anterior cerebral artery, with many small collaterals indicating c-MMS associated with c-TA (Fig. 1F). After control of active inflammation, surgical revascularization was performed for cerebral artery stenosis of c-MMS four months later. The left superficial temporal artery (STA) was anastomosed to the left intracranial MCA (STA-MCA anastomosis), with a left encephalomyosynangiosis (EMS). However, another episode of right hemiparesis, dysphasia, and facial palsy ensued two days after surgical revascularization. A right encephaloduromyosynangiosis (EDMS) was performed to stop further neurological deterioration successfully. Postoperative brain time-of-flight MRA showed patent cerebral blood flow (CBF) through the STA-MCA anastomosis and collaterals. Unfortunately, aortic pressure soared up to 200/120 mmHg (1.31 years after the first SI/PTRA). Abdominal aortography showed in-stent restenosis (2.11 mm) of the right renal artery, and native ostial stenosis (1.28 mm) of the left renal artery. Cutting balloon angioplasty, using a Flextome™ Cutting Balloon (4.0 × 6 mm; Boston Scientific, Galway, Ireland), was performed to dilate the in-stent restenosis of the right renal artery. Afterward, we used two larger balloon catheters (5.0 × 14 mm, Falcon Forte™; Invatec, Roncadelle, Italy; 7.0 × 20 mm, Sterling Monorail™, Boston Scientific) to dilate the targeted right renal artery and left renal artery to 3.76 and 2.93 mm, respectively. Aortic pressure dropped to 168/108 mmHg. At the 32-month follow-up, she had headache occasionally in spite of oral medication of prednisolone, antihypertensive agent, and anticoagulants. At the 60-month follow-up, aortography showed in-stent restenosis of the right renal artery (1.78 mm) and restenosis of the native left renal artery (2.30 mm). Aortic pressure soared up to 209/120 mmHg. Heparin (5,000 units) was infused beforehand. Gradational cutting balloon angioplasty was performed to relieve the in-stent restenosis of the right renal artery, using a Flextome™ (4.0 × 10 mm; Boston Scientific) and a Peripheral Cutting Balloon (7.0 × 2.0 cm; Boston Scientific). A new stent (6.0 × 14 mm, Sterling Monorail™ Express Renal Stent; Boston Scientific) was implanted to relieve the native restenosis of the left renal artery. After the above two procedures, the in-stent restenosis of the right renal artery and the native restenosis of the left renal artery was dilated to 3.49 and 4.94 mm, respectively. Aortic pressure dropped to 135/72 mmHg.
Since the latest SI/PTRA, the patient's blood pressure was around 130–150/80–100 mmHg. ESR, renin, renin activity, and aldosterone dropped to normal levels. Right hemiplegia and dysarthria improved gradually after physical rehabilitation and linguistic training. Amaurosis fugax, dysphasia, paresthesia, and central facial palsy disappeared. She worked as a full-time cashier in a supermarket. Abdominal CTA showed stents in situ of the targeted renal arteries (Fig. 1G). Brain MRI showed residual left encephalomalacia (Fig. 1H). Brain perfusion scan showed no significant difference of CBF, cerebral blood volume, time to peak, and mean transit time between right and left cerebral hemispheres (Fig. 2), indicating patent collaterals after surgical revascularization for cerebral artery stenosis of c-MMS associated with c-TA. The results of SI/PTRA were graphically expressed in Fig. 3. The demographic data of this patient were tabulated in Table 1.
Fig. 2
Brain perfusion scan showed no significant difference of cerebral blood flow (102.21 vs. 97.08 mL/100 mL/min), cerebral blood volume (5.15 vs. 4.88 mL/100 mL), time to peak (8.05 vs. 8.16 seconds), and mean transit time (3.08 vs. 3.02 seconds) between right (denoted by 1a) and left (denoted by 1b) cerebral hemispheres, indicating good collateral arteries after surgical revascularization for cerebral artery stenosis due to moyamoya syndrome associated with childhood-onset Takayasu arteritis.

Fig. 3
Results of endovascular revascularization for bilateral ostial renal artery stenosis incriminating childhood-onset Takayasu arteritis. The stenosis ratio of the targeted renal artery is expressed in percentage, which equals 100 − (diameter of stenotic renal artery/diameter of normal renal artery).
ER = endovascular revascularization, LRA = left renal artery, Post-ER = after endovascular revascularization, Pre-ER = before endovascular revascularization, RRA = right renal artery.

Table 1
Examination and treatment of Takayasu arteritis

DISCUSSION
TA is one of the leading causes of pediatric RVH in Asia, however, 26%–70% of patients were asymptomatic and had hypertension found only incidentally.1 Brunner et al.2 demonstrated that the incidence of hypertension and elevated ESR were higher in 241 pediatric patients (82.6% and 61.0%) than in 844 adult patients (52.5% and 45.2%) with TA. Fieldston et al.3 proposed that extensive imaging of the vascular system should be performed to achieve an early diagnosis of TA in children who presented with hypertension, elevated ESR, and systemic complaints. Even though, early diagnosis of c-TA remains a daunting challenge to pediatricians. Lately, the classification criteria for c-TA has been validated, including a mandatory criterion of angiographic abnormality plus at least one of the following five criteria: pulse deficit or claudication, blood pressure discrepancy in four limbs, bruits, hypertension, and elevated acute phase reactant.4 Our patient's clinical presentations met the classification criteria of c-TA, including angiographic abnormality, systemic hypertension, and elevated acute phase reactant.
Treatments with corticosteroids, immunosuppressants, and biologics have been reported with success, however, there was no evidence showing the superiority of a single agent over another for the treatment of c-TA.56 Disease progression raises questions about the necessity of revising current therapeutic strategies for c-TA, despite that immunosuppression could be achieved by corticosteroids, immunosuppressants, and biologics.56 Corticosteroid can ameliorate active inflammation of c-TA, but it cannot cure RVH caused by RAS (RVH/RAS). Antihypertensive agents were only palliative for RVH/RAS. Because of the progressive nature of RAS, repeated PTRA has been advocated as a treatment of choice.7 SI should be reserved as a bailout procedure for childhood RAS, if there was suboptimal results or arterial dissection after PTRA.8
Although the incidence of cerebrovascular stroke in c-TA (8.5%)9 is lower than that seen in adult-onset TA (15.8%),10 it is prudent to do cerebrovascular imaging studies to screen for cerebral artery stenosis in c-TA before endovascular revascularization, even without clinical manifestations of the central nervous system.
Moyamoya disease (MMD) is referred to an idiopathic occlusion of bilateral arteries of the circle of Willis, and MMS is defined as an underlying disease having a similar angiographic feature of a puff-of-smoke (moyamoya).11 The incidence of MMS in c-TA is extremely low, and was reported only anecdotally in c-TA.1112 There are four types of presentation in MMD (ischemic, hemorrhagic, epileptic, and other), and the ischemic type is predominant in children,13 disregarding its underlying diseases. Surgical revascularization is the mainstay treatment for c-MMD, including direct procedure of STA-MCA anastomosis, indirect procedures of EMS, EDMS, and encephaloduroarteriosynangiosis, and a combination of both.13 However, surgical revascularization could be a double-edge sword, since it can improve cerebral circulation and reduce the risk of subsequent cerebrovascular stroke and transient ischemic attack, but it may also cause postoperative neurological deterioration due to cerebral watershed shift or cerebral hyperperfusion syndrome (CHS).13 CHS was defined as the presence of a significant increase in CBF at the site of the STA-MCA anastomosis which is responsible for the apparent neurologic sign.14 The incidence of CHS, after anastomosis, was 5.3% in c-MMD15 and 22.7% in adult-onset MMD,16 disregarding its underlying diseases. The risk factors for CHS were left hemisphere operation, higher postoperative CBF, and higher postoperative/preoperative CBF ratio adjusted by cerebellar CBF.16 Since CHS usually occurred 2–6 days after surgery, quantitative analysis of CBF by means of single-photon emission computed tomography, micro-Doppler ultrasonography, perfusion-weighted MRI, and time-of-flight MRA is highly recommended within 48 hours after surgery.16 What orchestrates the pathogenesis of the CHS after STA-MCA anastomosis remains uncertain. The hypothesis may be increased pro-inflammatory cytokines, molecules, and intrinsic vulnerable microvascular structure (medial thinness and abnormality of the internal elastic lamina), excessive accumulation of pro-inflammatory cytokines and molecules (vascular endothelial growth factor, matrix metalloproteinase 9, etc.) and reactive oxygen products, and finally increased permeability of the blood-brain barrier.17 Prophylactic blood pressure lowering (110–130 mmHg)17 and minocycline (200 mg/day, a neuroprotective antibiotic that may ameliorate cerebral edema/hemorrhage by blocking matrix metalloproteinase 9),18 can prevent focal neurological deterioration due to CHS. In the present case, the patient's blood pressure dropped to 128/86 mmHg after the first attempt of endovascular revascularization and was once kept in the recommended ranges of 110–130 mmHg.17 However, decreasing blood pressure by endovascular revascularization, together with the intrinsic nature of ongoing active inflammation of c-TA,19 may potentially render flare-ups of renal and cerebral artery stenosis in this patient. STA-MCA anastomosis provides favorable long-term outcomes,15 however, an up-to-date one-stage surgery, including unilateral STA-MCA anastomosis, with EDMS, and bifrontal encephalo-duro-periosteal-synangiosis, has been proposed as an alternative to prevent neurocognitive decline in c-MMD.20
In conclusion, the intrinsic nature of ongoing active inflammation of c-TA may render flare-ups of renal and cerebral artery stenosis. Decrease of blood pressure by endovascular revascularization and improvement of cerebral perfusion by surgical revascularization may have exposed the cerebral deep watershed zone to ischemia and/or CHS by a steal phenomenon (or Venturi effect), and caused focal neurological deficits in our patient. Revascularization could be a double-edge sword for concomitant cerebral and renal artery stenosis in c-MMS associated with c-TA, and should be performed with caution.
 XML Download
XML Download