

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The rate of bladder diverticulum was reported to be 0.17% (85 children, 54 boys) in pediatric genitourinary data of 5,084 children, and 34 cases were primary type.1 Primary or congenital bladder diverticulum (CBD) is caused by a congenital weakness in the bladder musculature, either unilateral or bilateral. CBD should be differentiated from acquired diverticula, which are seen in children with obstruction of the bladder outlet or with neurogenic bladder.2 Almost all cases of CBD are reported in boys, and the main clinical presentations are recurrent urinary tract infection (UTI) and urinary retention as in three reported Korean cases.345 CBD should be corrected as early as possible because of the risk of severe kidney damage.6 An unusual case of CBD has presented with sudden visual disturbance caused by hypertensive retinopathy, which was found to be the result of obstructive uropathy, at our institution.
CASE DESCRIPTION
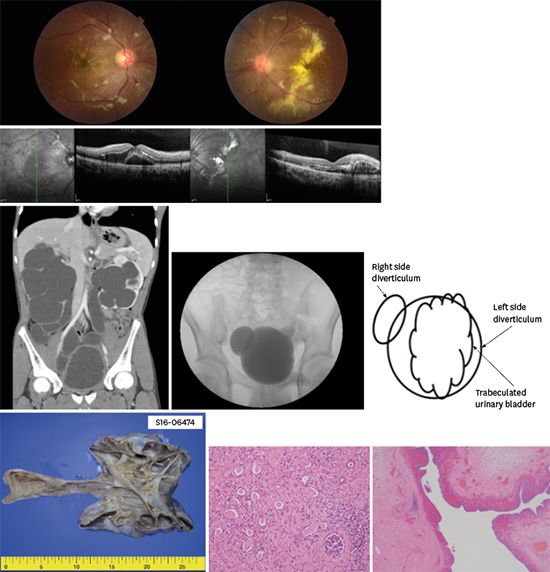
A 15-year-old male adolescent was admitted to the pediatric ward for the evaluation and management of severe hypertension on May 4th, 2016. Two weeks before, he had developed a sudden visual disturbance in his left eye. The ophthalmologic exam disclosed hypertensive retinopathy (Fig. 1). He had been suffering from intermittent headache in the left temporal region for 3 weeks. He had ignored suspicious hypertension detected on a school health exam several years before. He was delivered spontaneously at term with a birth weight of 3.1 kg. His past medical history revealed inguinal hernia operation at 1 year of age, and a UTI as an infant. The patient's family history showed no hypertension or kidney disease. His body measurements were as follows; height 175.3 cm (the 75–90th percentile), weight 53.7 kg (the 25–50th percentile), and body mass index 17.5 kg/m2 (the 5–10th percentile). His vital signs were unremarkable except high blood pressure of 189/146 mmHg. Complete blood count (CBC) showed low hemoglobin of 12.8 g/dL, normal hematocrit of 39.2%, and normal white blood cell (WBC) count of 7,200/µL. Blood chemistry showed increased blood urea nitrogen (BUN) of 20.5 mg/dL (reference 789101112131415161718), creatinine of 1.66 mg/dL (0.50–1.06), and uric acid of 9.9 mg/dL (2.5–8.3), meaning decreased renal function. Although the serum aldosterone-to-renin ratio of 4.04 in the supine position did not increase, the serum renin activity of 5.45 ng/mL/hr (supine 0.30–2.90) and the aldosterone level of 22.06 ng/dL (supine 1.0–10.5) were elevated simultaneously. Urine was straw clear in color with specific gravity of 1.015 and a pH of 5.0. Stick tests were all negative. The urine protein-to-creatinine ratio of 0.084 did not increase (protein 118 mg/day, creatinine 1,400 mg/day). The 24-hour urine vanillylmandelic acid (VMA) and metanephrine was negative. The urine culture was negative. The abdominal and pelvic computed tomography (CT) scan revealed severe hydronephrosis and hydroureter in both kidneys (Fig. 2). During the cystoscopic exam, the posterior urethral valve was not found, but trabeculation was found in the bladder. Voiding cystourethrography (VCUG) showed no evidence of vesicoureteral reflux (VUR), but revealed bilateral CBD causing obstruction of both ureters (Fig. 3). Urodynamic studies were performed to evaluate the bladder function and rule out obstruction of the bladder outlet, and detrusor overactivity with 225 mL of maximum bladder capacity was reported. Uroflowmetry showed a maximum flow rate of 46.4 mL/sec with 338 mL voided volume. We could not evaluate the postvoid residual urine volume due to urine in the diverticula. After we confirmed on the 99mTc-dimercaptosuccinic acid (DMSA) scan (left:right = 92.8:7.2) that the right kidney was nearly non-functioning, we performed a laparoscopic simple right nephrectomy, and then diverticulectomy through a lower midline incision. The left ureter was reimplanted in the bladder with the insertion of a double J stent. The surgical specimen showed atrophied renal parenchyma and a dilated ureter (Fig. 4). The diverticulum was paraureteral position. The microscopic exam showed chronic pyelonephritis (Fig. 5A), and the partial loss of the bladder musculature in the diverticular wall (Fig. 5B). The elevated pre-operative serum creatinine level (up to 3.16 mg/dL) decreased to 1.66 mg/dL after surgery. Hypertension was controlled with a combination of atenolol (β1 blocker), enalapril (angiotensin converting enzyme inhibitor), and amlodipine (calcium channel blocker).
Fig. 1
Ophthalmologic examination. (A) Retinal hemorrhage, cotton wool spot and severe exudate on fundus examination and (B) serous retinal detachment and intraretinal fluid on both eyes on optical coherence tomography.

Fig. 2
Computed tomographic findings. Severe hydronephrosis and hydroureter in both kidneys with obstructive lesion in both ureters.

Fig. 3
Bilateral bladder diverticula without vesicoureteral reflux. (A) Voiding cystourethrogram and (B) diagram.



DISCUSSION
In this case, the patient had secondary hypertension caused by a kidney problem. The obstructive nephropathy seemed to be caused by enlarged bladder diverticula, because there was no obstruction of the bladder outlet, such as a posterior urethral valve or neurogenic bladder. The classic definition of diverticulum is a mucosal herniation through the muscular wall.7 Among Pieretti and Pieretti-Vanmarcke's six cases,2 only two cases had few muscle fibers, and the other four cases had mucosa and adventitia in diverticula. Whereas, all seven cases of the Garat et al.'s diverticula cases7 for which a pathologic examination was performed had fine muscle fibers particularly at the dome of the diverticula. However, in any case, the diverticula could not contract appropriately to void into the bladder. Secondary diverticula are seen in trabeculated bladders and are usually associated with obstruction of the bladder outlet.6 Because our case had no obstruction of the bladder outlet, it was primary or congenital diverticula. However, there was a report of a bladder neck obstruction compressed by large CBD, arising from the posterior-inferior aspect of the bladder.8 The pathophysiological explanation of this diverticula was failure of detrusor due to muscle hypoplasia or the lack of a functional muscle layer.9 Almost 90% of CBD's are located near the ureteral orifice where the detrusor layer is weak at Waldeyer's sheath.10 This form of diverticula is subclassified into two types based on the location of the ureteral orifice. In a periureteral diverticulum, the separate ureteral orifice enters the bladder directly, while in a paraureteral diverticulum, the ureteral orifice is near the diverticular mouth.61011 Both types are associated with VUR and hydronephrosis, while the periureteral type has a lower rate of occurrence (15%–33%).710 The other 10% of CBD cases, termed posterolateral location, is not related to the ureteral orifice and VUR.10 These posterolateral diverticula are suggested to form in the weak embryologic junctions between the trigone (mesodermal origin) and the bladder dome (endodermal origin).12 Finally, several congenital syndromes are associated with bladder diverticula; Menke's kinky hair syndrome, Ehlers-Danlos syndrome, and Williams-Beuren syndrome.6
In the absence of the obstructed bladder outlet and VUR as in our case, how can the ureters and the kidneys be dilated? We speculated that initially VUR must have existed until the diverticula were enlarged by vesicodiverticular reflux enough to obstruct the ureters.7 The pathologic findings of chronic pyelonephritis and the history of UTI during the childhood might support the previous existence of VUR in our case. Barrett et al.13 found VUR in most cases of paraureteral diverticula, however they observed spontaneous resolution of reflux in those children due to the distortion of the ureterovesical junction by the diverticula. According to Garat et al.,7 only 4 of 11 cases were associated with VUR. Therefore, association with VUR has varied greatly from one series to another. The urinary stasis in poorly muscularized diverticula made the urinary system susceptible to UTI.14
In contrast to the two major symptoms of UTI and urinary retention reported for many cases, the hypertensive retinopathy in our case is very unusual. The pathologic findings of chronic pyelonephritis and obstruction of the upper track made the patient hypertensive, as evidenced by the increased renin and aldosterone levels in our case. Secondary hypertension caused by hydronephrosis has been described in an animal model,15 but is not commonly reported in medical literature.1617 In the hydronephrotic condition, the pathologically increased tubuloglomerular feedback system and the increased activity of renin-angiotension-aldosterone system contribute to the development of hypertension.1518
Complete surgical excision of the diverticula and ureteroneocystostomy can cure the UTI and voiding dysfunction.1314 Because our case was too long-standing and the remaining kidney also had chronic pyelonephritis, the patient's renal function and hypertension did not return to normal postoperatively.
In summary, this case shows that congenital bladder diverticula can cause latent UTI, ureteral obstruction, hydronephrosis and subsequently severe hypertensive retinopathy presenting as a sudden visual disturbance in adolescence.
 XML Download
XML Download