

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Generally, traumas associated with clinical symptoms include death and loss of significant people, abuse, violence, natural disaster, and accidents.1234 The experience of trauma is thought to lead to clinical symptoms such as re-experience of trauma, sleep disturbance, extreme fear, depression, and severe anxiety.23 Especially, the experience of serious trauma in the adolescent period has been reported to be an important predictive factor of behavior disturbance, school life maladjustment, and suicide attempts.5 During their lifetimes, 25% of adolescents have experienced trauma and show psychological symptoms of grief, depressed mood, and agitation.6 In a six-month follow-up study of Korean elementary school students who had experienced a single traumatic incident, 65.5% of the participants were reported to have one or more anxiety or depression symptoms six months after the trauma.7 Post-traumatic stress disorder (PTSD) can occur at any age, beginning after the first year of life. Symptoms usually begin within the first 3 months after the trauma.8 Therefore, recognizing the experience of trauma and assessing post-traumatic symptoms in adolescents earlier within 3 months after trauma appear to be important in the prevention of mental illness in later life.
Measures used to assess post-traumatic symptoms in children and adolescents have included the Child PTSD Symptom Scale, the Child Reaction to Traumatic Events Scale, and the Traumatic Symptom Checklist for Children.9 In response to increasing concern about the impact of trauma on children and adolescents, several assessment and screening tools have been developed in recent decades.10 The University of California, Los Angeles, Post-traumatic Stress Disorder Reaction Index (UCLA-PTSD RI) is a 22-item self-report questionnaire that assesses post-traumatic stress in children and adolescents.11 Its items were designed to reflect the PTSD symptoms described in the Diagnostic and Statistical Manual IV (DSM-IV).11 This scale has excellent internal consistency, with a Cronbach's α ranging from 0.85 to 0.90.1213 For urgent assessment of PTSD in a large population of children and adolescents, the Abbreviated UCLA-PTSD RI (Abb-UCLA-PTSD RI) has been suggested, which is simplified to only nine items and is recommended for children and adolescents aged eight years or older.4
We aimed to verify our hypothesis that the Korean version of Abb-UCLA-PTSD RI (Abb-UCLA-PTSD RI-Korean version) among Korean adolescents is useful for assessing post-traumatic stress.
METHODS
Participants
We selected one elementary school, one middle school, and one high school in Daegu for study using the random sampling service of the Korean Educational Statistics Service.14
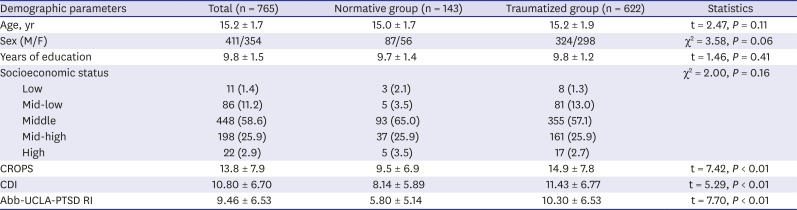
We gained informed consents from principals, parents, and students. A total of 1,254 students were recruited, representing a response rate of 97.2% (1,254/1,290). There were no differences in sex or age distribution between participants and non-participants. Missing data values were input using an expectation-maximization algorithm.3 Among 1,254 samples, 143 students had been classified in the normative group with Lifetime Incidence of Traumatic Events (LITE) 1 and 622 were in the traumatized group with LITE 4 (Table 1).
Table 1
Demographic characteristics
Measures
Demographic characteristics including age, sex, and years of education were collected. We also collected subjective status of socioeconomic status and each student marked one among low, mid-low, middle, mid-high, and high. Participants were also asked to complete the Abb-UCLA-PTSD RI-Korean version, the Child Report of Post-Traumatic Symptoms (CROPS), the LITE, and the Children's Depression Inventory (CDI). The nine-item Abb-UCLA-PTSD RI scale is a self-report measure assessing the severity of post-traumatic stress symptoms.4 Each of the nine items is rated using a five-point Likert scale from 0 (not at all) to 4 (severe). It was modified from the 22 items of the UCLA-PTSD RI scale used to screen and monitor the response to treatment in children and adolescents aged 7 to 18 years.411 The CROPS is a 26-item self-report scale measuring the severity of post-traumatic symptoms in children and adolescents aged 6 to 18 years.15 Each of the 26 items is rated using a three-point Likert scale from 0 (none) to 1 (some) to 2 (lots). The total score is calculated by summing the responses of the 26 items. Higher scores reflect more severe symptoms of post-traumatic stress. The scale has reasonable internal consistency (Cronbach's α = 0.89–0.92).1516 The LITE is a checklist assessing trauma or losses that a child or adolescent might have experienced. The LITE assesses the age at which the trauma occurred, how many times the trauma has occurred, and the severity of the child's experience of the trauma.15 The items of the LITE investigate car accidents, house fires, death of a family member, exposure to threats, sexual assaults, witness to violence, and other potentially upsetting events. The test-retest reliability of the LITE is relatively high (r = 0.80; P < 0.001). Once a child completes the LITE measure, the responses are reviewed by a clinician, and the child is rated as 1 (no trauma or loss), 2 (possible trauma/loss), 3 (probable trauma/loss), or 4 (definite trauma/loss).15 A person with LITE 1 has no trauma experience and a person with LITE 4 has definite trauma history. The CDI is a self-report scale for assessing the severity of depressive or dysthymic symptoms in children and adolescents aged 7 to 17 years.17 It consists of 27 items regarding negative mood, interpersonal problems, ineffectiveness, anhedonia, and negative self-esteem. The internal consistency of the CDI is indicated by Cronbach's α = 0.71–0.89.17 A total CDI score of 36 or higher indicates severe depression.
Data analysis
The 143 students in the normative group with LITE 1 had no trauma experiences and 622 students in the traumatized group with LITE 4 had clear trauma experiences. We included these 765 students in the analysis. The differences in demographic characteristics between the traumatized group and normative group were analyzed with χ2 test and independent Student's t-test. Confirmatory factor analysis (CFA) was performed using AMOS (IBM Corp., Armonk, NY, USA) and indicated acceptable model-fit (Comparative Fit Index [CFI] > 0.95, Tucker-Lewis Index [TLI] > 0.90, and root mean square error of approximation [RMSEA] < 0.08) and standardized root mean square residual [SRMR] < 0.05).18 To identify the best model, we performed an analysis with only the items with a factor loading greater than 0.4. As a rule of thumb, variable should have a rotated factor loading of at least 0.4 onto one of the factors in order to be considered important.19
The two-factor model was found to have the best model-fit (CFI > 0.95, TLI > 0.90, and RMSEA < 0.08). All analysis was performed using IBM AMOS SPSS Statistics version 18.0 (IBM Corp.).
RESULTS
Demographic characteristics
Of the 1,254 student participants, 143 (11.4%) had a score of LITE 1, 299 (23.8%) had a score of LITE 2, 190 (15.2%) had a score of LITE 3, and 622 (49.6%) had a score of LITE 4. Considering the purpose of the current research, we recruited the 765 students whose scores were LITE 1 or LITE 4. The mean age of the 765 participants was 15.2 ± 1.7 years (Table 1).
Reliability, validity, and descriptive statistics
The internal consistencies of the nine-item and eight-item versions of the Abb-UCLA-PTSD RI-Korean were found to be high (Cronbach's α = 0.843 and 0.842, respectively). The test-retest reliability of the nine-item version was r = 0.77 (P < 0.001), and that of the eight-item version was r = 0.85 (P < 0.001). The criterion-related validity was based on comparison of the UCLA-PTSD RI total scores between the normative and the traumatized groups. For the nine-item version, the normative group (4.5 ± 4.3) and the traumatized group (8.5 ± 5.0) scores demonstrated good criterion-related validity (t = 7.92; P < 0.001). For the eight-item version, the normative (4.6 ± 4.6) and traumatized groups (8.8 ± 6.0) demonstrated even better criterion-related validity (t = 9.26; P < 0.001) (Table 1).
Factor analysis
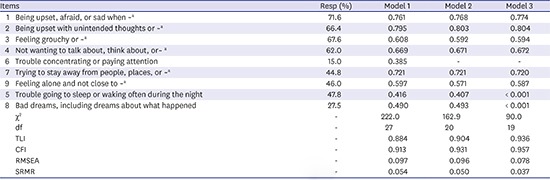
Using CFA, we analyzed three models to determine the best-fit model for the clinical sample. Model 1 was a one-factor model with nine items. Model 2 was a one-factor model with eight items. Model 3 was a two-factor model with eight items: two items regarding sleep composed the first factor, and the other six-item made up the second factor. The fit indices for Model 1 were χ2 = 222.0, P < 0.001, SRMR = 0.054, RMSEA = 0.097, TLI = 0.884, and CFI = 0.913. The factor loadings were greater than 0.4 for all items in Model 1 except item 6, which had a factor loading of 0.385. The fit indices for Model 2 were χ2 = 162.9, P < 0.001, SRMR = 0.050, RMSEA = 0.096, TLI = 0.904, and CFI = 0.931. All factor loadings in Models 2 and 3 were greater than 0.4 for all items. Model 3 obtained the best-fit to the data: χ2 = 90.0, P < 0.001, SRMR = 0.037, RMSEA = 0.078, TLI = 0.936, and CFI = 0.957 (Table 2).
Table 2
Factor loadings for the Abb-UCLA-PTSD RI-Korean version
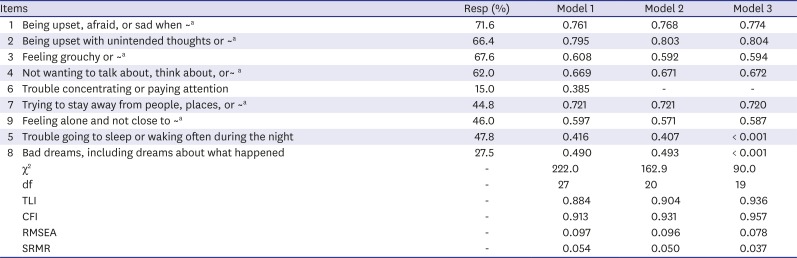
Abb-UCLA-PTSD RI-Korean version = Korean version of the Abbreviated University of California, Los Angeles, Post-Traumatic Stress Disorder Reaction Index, Resp (%) = response rate of more than “few”, Model 1 = nine-item, one-factor model, Model 2 = eight-item, one-factor model, Model 3 = eight-item, two-factor model, df = degree of freedom, TLI = Tucker-Lewis Index, CFI = Comparative Fit Index, RMSEA = root mean square error of approximation, SRMR = standardized root mean square residual.
aFull sentence of each item has not been written to protect copyright of Abb-UCLA-PTSD RI-English version.
DISCUSSION
Using a sample of 765 Korean adolescents aged 11–19 years, the current study assessed the psychometric properties of the Abb-UCLA-PTSD RI-Korean version, including its reliability and validity. Our findings suggest that the eight-item version of this scale has better internal consistency and validity than the nine-item version.
The internal consistency of the Abb-UCLA-PTSD RI-Korean version was good (Cronbach's α = 0.84), similar to that of the original UCLA-PTSD RI (Cronbach's α = 0.85).12 The test-retest reliability of the Abb-UCLA-PTSD RI-Korean version was r = 0.85 (P < 0.001), higher than the 0.70 required for acceptance.1 The criterion-related validity was assessed by comparing the normative and traumatized groups and was also acceptable (t = 7.92; P = 0.001).
As shown in Table 2, Korean adolescents appear to experience post-traumatic stress in terms of being upset, afraid, or sad when thinking about a trauma; being upset with unintended thoughts or pictures of a trauma; feeling grouchy or angry and not wanting to talk about, think about, or have feelings about a trauma. The first step in supporting youth with post-traumatic stress might be to detect the signs and symptoms of being upset or angry and encouraging verbal expression.20 Our identification of the four most common factors can be helpful for assessing and managing the care of adolescents in Korean society.
The nine-item Abb-UCLA-PTSD RI-Korean version did not have good fit according to the CFA. Murray and colleagues reported a good CFA fit with a one-factor model of children with post-traumatic stress.21 The eight-item Abb-UCLA-PTSD RI-Korean version achieved acceptable factor loading scores except for item Q6, “Trouble concentrating or paying attention” (0.385), and had higher internal consistency than the nine-item version. However, the eight-item Abb-UCLA-PTSD RI-Korean version did not satisfy the good model-fit requirements of CFI > 0.95 and RMSEA < 0.8. When a two-factor model was applied to the current data, the CFA showed good model-fit indices of TLI, CFI, SRMR, and RMSEA. The first factor of this model comprised items representing sleep, and the second factor comprised the rest of the items representing other symptoms. In the tripartite DSM-IV PTSD model, Q5, “Trouble going to sleep or waking often during the night” is associated with criterion B, re-experiencing symptoms; and Q8, “Bad dreams, including dreams about what happened” is associated with criterion D, hyperarousal symptoms.22 However, in the eight-item Abb-UCLA-PTSD RI-Korean version, these two questions regarding sleep are merged into one. In addition, the differences between the studies of these two scales are probably due to the different numbers of items, different traumas (sexual violence vs. variable trauma), and different numbers of subjects (352 vs. 765).
There are several limitations of the current research. First, the number of items in the Abb-UCLA-PTSD RI-Korean version is fewer than in the original UCLA-PTSD RI, so the Abb-UCLA-PTSD RI-Korean version might not fully reflect the meaning of all the items in the original UCLA-PTSD RI. Second, self-report instruments can lead to over- or under-estimation in response to questions. Children with trauma are thought to under-report their traumatic symptoms due to their desire to avoid talking about the trauma event, particularly if the events are associated with secrecy or shame, for example child abuse or domestic violence.5 Based on our results, we conclude that the Abb-UCLA-PTSD RI-Korean version is a useful tool for screening post-traumatic stress in Korean adolescents. Moreover, the eight-item version of the Abb-UCLA-PTSD RI-Korean version showed greater validity than the nine-item version. We suggest that the eight-item Abb-UCLA-PTSD RI-Korean version would be useful for assessing post-traumatic stress syndrome in Korean adolescents.
 XML Download
XML Download