

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to the annual report of the causes of death statistics in Korea, 116.9 per 1,000 Korean people (110.8 in men, 123 people in women) died from cardiovascular diseases (CVD) in 2015; the death rate was higher among elderly population aged more than 70 years [1]. High insulin resistance was related to high risk of CVD according to several studies [2345]. Thus, a decrease in insulin resistance may provide health benefits.
Several studies suggest that high sodium diet [6789] and low potassium diet [910] are positively associated with insulin resistance, while others show an inverse association between sodium diet and insulin resistance [11121314] or provide no evidence of these associations [1516]. In addition, according to the 2015 Korea National Health and Nutrition Examination Survey, Koreans had a higher sodium intake (327% in men, 228% in women) and lower potassium intake (96% in men, 78% women) compared with the Adequate Intake of dietary sodium and potassium [17]. Thus, determination of the effects of sodium and potassium on insulin resistance among Korean is a pressing issue with relevance to the health of the Korean population.
Sodium-potassium ratio is a more sensitive indicator than individual sodium and potassium levels to affect blood pressure [18], but there is no study that examines the association between sodium-potassium ratio and insulin resistance to our knowledge. Furthermore, urinary sodium and potassium are more closely related to real digested sodium and potassium in the body compared to the self-reported dietary sodium and potassium intakes provided through dietary assessment of participants [19]. Therefore, the present study was conducted to elucidate how 24-h estimated urinary sodium-potassium ratio relates to insulin resistance or insulin sensitivity among Korean adults.
SUBJECTS AND METHODS
Study population
The Korean genome and epidemiology study (KoGES)_Ansan and Ansung study is one of the population-based cohorts in the KoGES, developed to investigate the genetic etiology and epidemiology of complex diseases (i.e., hypertension, obesity, metabolic syndrome, and cancer) and causes of death with long-term follow-up among the Korea population in 2001. Detailed explanation of this cohort is reported in a previous study [20]. The base-line data collected in 2001-2002 was used for the present study. The KoGES_Ansan and Ansung study included 10,030 participants (5,012 from Ansan city and 5,018 from Ansung city) at the base-line. A total of 3,722 participants aged 40-69 years were included in this study after excluding participants who had not provided urine samples (n = 5,054); were treated with steroids (n = 20); had a history of hypertension (n = 757); were diagnosed with diabetes (n = 193), myocardial infarction (n = 26), congestive heart failure (n = 6), coronary artery disease (n = 21), peripheral vascular disease (n = 12), cerebrovascular disease (n = 22), kidney disease (n = 108), or cancer (n = 75); and had no documented records of fasting insulin and fasting glucose (n = 14). Written informed consent was obtained from all study participants, and this study was approved by the electronic institutional review board (e-IRB) of the Korea national institute for bioethics policy (KoNIBP) (P01-201603-21-006).
Measurement
Data regarding socio-demographic status, life-style, and medical history were collected by trained interviewers through questionnaires. These included age, sex, recruitment area, education status, monthly household income, occupation, marital status, alcohol consumption, cigarette smoking, and presence of diseases (hypertension, diabetes, CVD, kidney disease, and cancer). The daily energy intake was estimated using a food frequency questionnaire (FFQ) including 103 items, which was developed [21] and validated [22] for the KoGES. Height (cm) was measured using a stadiometer. Body mass index (BMI, kg/m2) was calculated by dividing weight (kg) by height in meters squared.
Urinary samples were self-collected by the participants themselves after more than 8 h of fasting, and were transported in conical centrifuge tubes for quantification by biochemical assays in the central laboratory (Seoul Clinical Laboratories, Seoul, Republic of Korea). Similar to our previous study [23], the current study calculated the 24-h estimated sodium and potassium levels, reflecting the actual ingested sodium and potassium in the body [19]. Tanaka equation was formulated in Japan to estimate the 24-h urinary sodium and potassium levels [24] and used to estimate the 24-h urinary sodium and potassium levels using spot urinary samples as in other studies [252627].
The homeostatic model assessment of insulin resistance (HoMA-IR) and fasting circulating insulin levels were used as indices of insulin resistance and the quantitative insulin sensitivity check index (QUICKI) was used as index of insulin sensitivity. The HoMA-IR and QUIKI were obtained using fasting insulin and fasting glucose levels as shown in the equations below.
[28].
[29].
Statistical analysis
The study participants were divided into quartile groups according to the 24-h estimated urinary excretion. The general linear model for continuous variables and the Cochran-Mantel-Haenszel test for categorical variables were used to describe the general characteristics of participants after adjustment for age and sex and to determine the potential confounding factors. Subjects' age, BMI, daily energy intake (kcal), sex, cigarette smoking status, alcohol consumption status, regular exercise status, and household income were adjusted in the multivariable models. The least square means and standard errors of insulin resistance indices according to urinary factors were calculated using the general linear model. When statistically significant effects were demonstrated, Tukey's post hoc comparison test was used to identify group differences. The results were considered statistically significant if the P-value < 0.05 in this study. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, North Carolina).
RESULTS
General characteristics
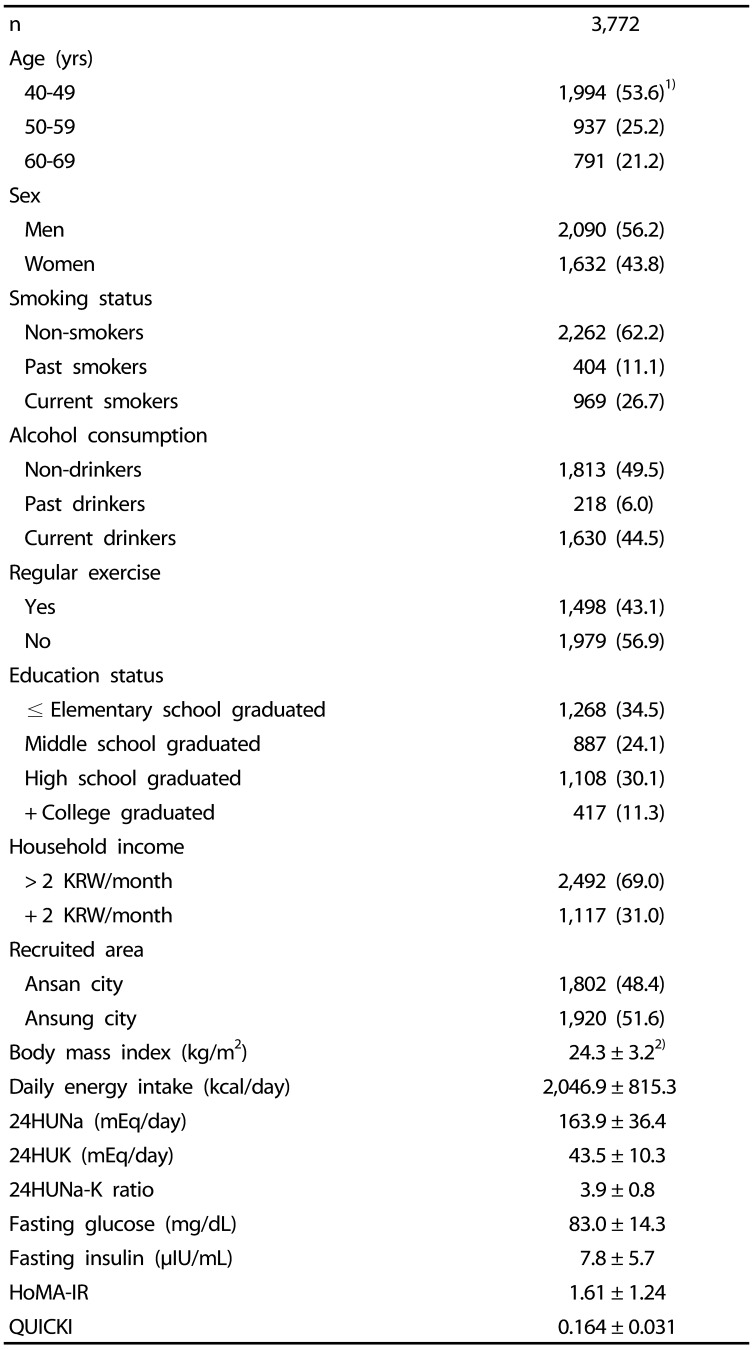
Table 1 shows the general characteristics of the study participants. Among the total subjects, 53.6% were in their 40s and 56.2% were male. The means of 24HUNa, 24HUK, and 24HUNa-K ratio were 163.9 mEq/day, 43.5 mEq/day, and 3.9, respectively. Furthermore, the means of fasting glucose, fasting insulin, HoMA-IR, QUICKI were 83.0 mg/dL, 7.8 µIU/ml, 1.61, and 0.164, respectively.
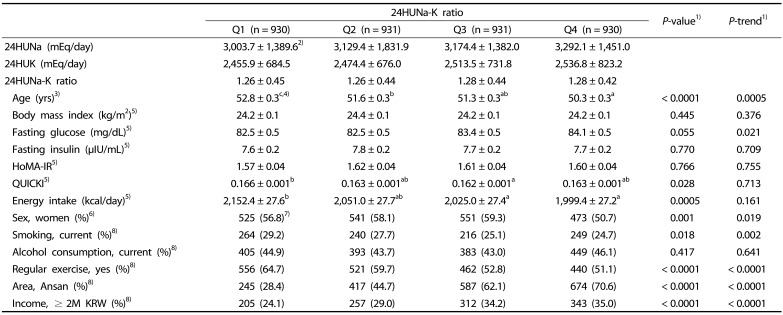
Table 2 lists the characteristics of study participants according to 24-h estimated urinary sodium-potassium ratio. The higher the 24HUNa-K ratio, the lower the age, proportion of women, percentage of current smokers, and percentage of people regularly exercising. On the other hand, the higher the 24HUNa-K ratio, the higher fasting glocose, Ansan residents, and proportion of high income.
Associations between urinary sodium-potassium ratio and insulin resistance
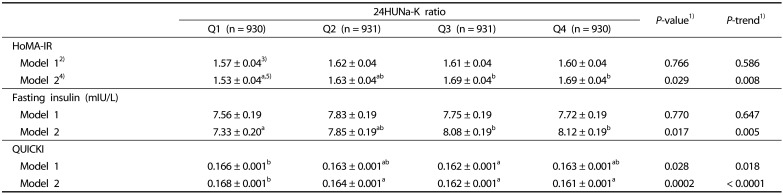
Table 3 shows adjusted means and standard error of HoMA-IR, fasting insulin, and QUICKI according to 24-h estimated urinary excretion of sodium-potassium ratio. Significantly positive correlation of 24HUNa-K ratio with HoMA-IR (P-value = 0.029, P-trend = 0.008) and fasting insulin (P-value = 0.017, P-trend = 0.005) is shown in Model 2. QUICKI was inversely associated with 24HUNa-K ratio in all models (P-value = 0.0002, P-trend < 0.0001 in Model 2).
DISCUSSION
This study was conducted to identify the effects of 24-h estimated urinary sodium-potassium ratio on insulin resistance or sensitivity among Korean adults. Our results suggest that the urinary sodium-potassium ratio was positively associated with insulin resistance and negatively related to insulin sensitivity.
Since there are no studies examining the effect of sodium-potassium ratio on insulin resistance or insulin sensitivity, previous studies examined the effects of sodium or potassium on insulin resistance or insulin sensitivity, respectively. Several studies reported a positive association of high-sodium diet [6789] or low-potassium diet [1011] with insulin resistance that cohere with these results. Sodium intake estimated by the urinary sodium to urinary creatinine ratio was positively associated with insulin resistance among Korean children or adolescents [3031]. Ames RP et al. [6] investigated the effect of modest sodium restriction on insulin resistance during 4 weeks in a cross-over design, and suggested that sodium restriction was associated with reduced insulin resistance. Kuroda S et al. [7] conducted a clinical trial to examine the causal effect of sodium sensitivity on insulin resistance with hypertension over 7 days, and found that a low-salt diet decreased insulin resistance. Dziwura et al. [8] conducted a cohort study to determine the relationship between salt sensitivity and insulin resistance. The groups of treatment were divided into amount of salt as low-, normal-, and high-salt. Results indicated that, participants of the high salt group had an increased HoMA-IR. Wan Z et al. [9] conducted a clinical trial to examine the effects of sodium and potassium on insulin resistance during 7 days, and found that a high salt diet was positively associated with insulin resistance and potassium supplements inversely associated with insulin resistance. Chatterjee R et al. [10] piloted a double-blinded randomized controlled trial to compare the effects of potassium supplements (40 mEq K/d) with matching placebo during 3 months, and found a significant trend for improved insulin sensitivity among the potassium-treated group. On the other hand, no associations between sodium and insulin resistance [1516] and negative associations between sodium and insulin resistance [11121314] were reported by several studies.
Although there are no studies that provide a direct mechanism to explain the effects of sodium-potassium ratio on insulin resistance in the body, hypothetic mechanisms have been proposed for the influence of sodium and potassium intakes on insulin resistance. First, the low-sodium diet decrease blood leptin levels leading to reduced size of abdominal fat cells, which diminishes the risk of obesity and insulin resistance [323334]. Second, the low-sodium intake regulates the expression of glucose transporter type-4 as the insulin receptor in fat cells, which might be associated with decreased insulin resistance [35]. Third, pancreatic beta-cell K(ATP) channels play a central role in glucose mediated insulin secretion. ATP sensitive potassium [K(ATP)] channels founded in the plasma membrane of many cells including pancreatic beta-cells, skeletal muscle, and brain may modulate glucose transport in the insulin target tissue [36].
There are several considerations in interpreting the results. First, because the current study is a cross-sectional design, the causal effect of sodium-potassium ratio on insulin resistance or sensitivity was not identified in this study. Second, we used spot urinary samples collected in specific point in time instead of 24-h urinary samples collected during a day (24 hours) reflecting higher levels of the actual metabolic indicator [19]. Twenty-four-hour urinary samples are generally difficult to use in population-based studies such as the present study because of cost for time and money. Furthermore, the 24-h estimates of urinary sodium and potassium levels, and their ratio are more appropriate than the dietary sodium, potassium, and sodium-potassium ratio obtained by FFQ.
There are two advantages in the present study. First, participants with a history of cardiovascular disease, kidney disease, or cancer were excluded from this study, because these diseases influence diet and lifestyle patterns of patients. Second, we used various parameters including HoMA-IR, fasting insulin, and QUICKI as markers of insulin metabolism, which were validated and frequently used to quantify insulin resistance or sensitivity.
In conclusion, we found that sodium-potassium ratios were positively associated with insulin resistance and inversely associated with insulin sensitivity among Korean adults. In order to decrease insulin resistance, a low sodium intake and a high potassium intake are recommended. Potassium is consumed via fruits and vegetables. Therefore, low-sodium intake should accompany high consumption of fruits and vegetables. Since the present study was a cross-sectional study, further studies are needed to corroborate these findings in clinical trials or prospective studies.
 XML Download
XML Download