

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Predominantly gram-negative anaerobic microflora in the plaque biofilm has been recognized to be a prerequisite for the initiation as well as the progression of periodontitis. However, the pattern and severity of destruction of periodontal tissues in a population cannot be explained exclusively based on a quantitative and/or qualitative analysis of this biofilm. Some additional risk factors and risk indicators have been identified to be associated with the pathogenesis of the inflammatory destruction of the periodontium. Moreover, the possibility that certain regulatory factors influence shifts in favour of protecting and repairing the periodontal tissues even in the presence of inflammation cannot be ruled out. The role of the signalling cascade that moderates the inflammatory process has been in focus recently. In this respect, the antioxidant defence system may be of great importance since oxidative stress has been implicated in a number of inflammatory diseases and conditions including cardiovascular disease [1], metabolic syndrome [2], type 2 diabetes [3], rheumatoid arthritis [4], macular degeneration [5] and inflammatory bowel disease [6], most of which have been associated with periodontitis.
Investigations have reported on the role of antioxidant micronutrients in reducing extracellular oxidative stress and in down-regulating intracellular redox-regulated, proinflammatory gene transcription factors [7]. The synergistic effects of these micronutrients may further reduce the risk and complications of disorders associated with reactive oxygen species (ROS).
Menopause has been reported to be associated with an increase in oxidative stress and a decrease in antioxidants [8,9]. A significantly lower total antioxidant capacity (TAOC) in postmenopausal women compared to healthy controls and a decrease of oxidative stress after hormone replacement therapy (HRT) has been demonstrated [8,10]. Oestrogen is a phenolic compound that shares similarities with the structure of well-known lipophilic antioxidants such as α-tocopherol. Moreover, studies have shown that maintenance of appropriate level of micronutrients in blood is positively influenced by hormonal replacement during menopause.
As oxidative stress has been suggested to form the key orchestration point for proinflammatory cascades that underpin tissue damage in inflammatory conditions [11], it is biologically plausible that additional oxidative stress associated with menopause may contribute towards higher periodontal destruction during the postmenopausal period. Furthermore, systemic inflammation associated with periodontitis during the postmenopausal period may promote increased cellular consumption of key antioxidant micronutrients [12]. We hypothesized that adjunctive supplementation of micronutrients could restore cytoprotective enzymes by quenching free radicals and activating enzymatic antioxidants, thereby improving the clinical outcomes of root surface debridement in postmenopausal women with chronic periodontitis.
In light of the paucity of nutritional interventional studies and the wide heterogeneity of the results of the studies that have been carried out and the corresponding inferences that have been drawn [6,13,14,15,16], the present interventional study explores the impact of adjunctive micronutrients on the cytoprotective enzyme superoxide dismutase (SOD) and periodontal inflammation in postmenopausal women.
MATERIALS AND METHODS
This study was conducted in the Department of Periodontics and Oral Implantology, Post Graduate Institute of Dental Sciences, Rohtak. The study protocol was approved by the Institutional Review Board and carried out in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki, as revised in 2008.
Postmenopausal chronic periodontitis (45-55 years) patients having ≥20 teeth were enrolled into the study. Postmenopausal subjects were identified as subjects who had entered a natural menopause with their last menstrual period at least 12 months ago [8]. Chronic periodontitis patients were diagnosed by the following criteria: at least two or more interproximal sites with attachment loss ≥4 mm, or two or more interproximal sites with probing depths ≥5 mm, not on the same tooth [17].
Subjects were excluded who had undergone oral prophylaxis or who had taken multivitamins or antioxidant micronutrient supplements in the previous six months, who were consuming a micronutrient-rich diet, who were using mouthwashes regularly, current and former smokers, anemic patients, patients who had taken anti-inflammatory or antibiotic drugs within the previous three months, patients with other medical conditions that could influence the results of periodontal treatment, patients who had underwent HRT, and patients who had entered artificial menopause. A detailed history and a consultation with their physicians were relied upon to rule out presence of any of the above-mentioned conditions.
Participants were enrolled into the following groups. Patients in group 1 (n=22) were provided periodontal treatment in the form of scaling and root planing (SRP) and group 2 (n=21) patients received SRP along with systemic administration of micronutrient antioxidants in the form of soft gelatin capsules (Antoxid, Dr. Reddy's Laboratories Ltd., Hyderabad, India) containing 10 mg of beta carotene, 27.5 mg of zinc sulphate monohydrate, 70 mcg of selenium dioxide (as selenious acid), 2 mg of manganese (as manganese sulphate monohydrate), and 1 mg of copper (as copper sulphate pentahydrate) once daily for three months.
Informed consent was obtained from each patient after explaining the study along with the risks and benefits in their own language.
The following parameters were evaluated: probing pocket depth (PPD), clinical attachment level (CAL), bleeding on probing (BOP), gingival index (GI) [18], and plaque index (PI) [19]. The improvement of BOP (%) and GI was taken as the primary outcome. Bleeding scores were expressed as the percentage of positive sites per subject (BOP [%]). All the above parameters were recorded on four sites per tooth except BOP, which was recorded on six sites for each tooth. These parameters were recorded at baseline and at 3 months after the completion of nonsurgical periodontal therapy.
Examiner reproducibility was verified by carrying out double clinical periodontal data recordings on ten patients. Reproducibility was found to be >90% in agreement for PPD and CAL (for PPD, the kappa value ranged from 0.79 to 0.83 whereas for CAL, the kappa value ranged from 0.82 to 0.87).
Collection of samples
All samples of saliva and blood at baseline and at the 3-month follow-up were obtained in the morning following an overnight fast. All participants were told not to eat or drink (except water) for the same period and abstention was checked prior to biological sample collection. Unstimulated whole saliva samples and venous blood from the anticubital vein were collected in plain vacutainer tubes without additives. Serum and saliva aliquots were stored at -80℃ in a deep freezer until analysis.
Periodontal treatment
SRP was performed using manual instruments (Hu-Friedy scalers and curettes, Chicago, IL, USA) and an ultrasonic scaler (P5 booster, Suprasson, Satelec, Merignac, France). The patients were instructed to use only mechanical plaque control aids during the study period. Mouthwashes and/or antimicrobials were not prescribed. Compliance to micronutrient antioxidant consumption in group 2 was assessed by residual capsule counts at the three month recall visit.
SOD assay
The SOD activity of serum and saliva samples was evaluated using an SOD assay Kit (Sigma Aldrich Co., St. Louis, MO, USA) according to the manufacturer's instructions, and an enzyme-linked immunosorbent assay (ELISA) reader (Robonik India Private Ltd., Maharashtra, India) at 450 nm. The SOD activity was obtained from the manufacturer's formula using the values from the ELISA test.
Power calculation and statistical analysis
A minimum sample size of 15 per group is required for detection of a significant difference in BOP (%), assuming the effect size (d) equals to 1, with a two-sided 0.05 level of significance and 80% power [20]. The data for all groups were found to be nonnormally distributed by the Kolmogorov-Smirnov test. The intragroup baseline and the posttreatment comparison of periodontal and biochemical parameters were analyzed using the Wilcoxon signed-rank test. The Mann-Whitney U-test was used to compare changes (Δ) from baseline to 3 months between the groups. All statistical analyses were carried out using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA), with a two tailed P-value of 0.05 used as a threshold for significance.
RESULTS
The patients in both groups received the intended treatment. All except three patients (2 from group 1; 1 from group 2) reported at the 3 months follow-up examination. However, all 43 patients were taken into consideration for statistical analysis as per the requirements of per-protocol analysis. The reasons given for of dropping out from the study included the distant locations of the participants or their families. No complications associated with the study were observed in the participants. Replicating the statistical analysis after excluding the patients who dropped out did not result in any change in the results of the study.
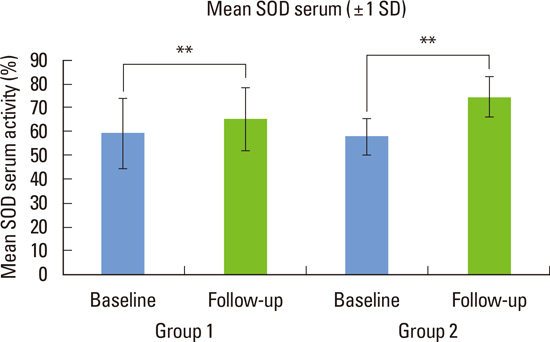
The demographic, periodontal and biochemical characteristics at baseline for both groups are outlined in Table 1. All the periodontal and the biochemical parameters exhibited statistically nonsignificant differences between groups 1 and 2 at baseline. Significant improvements in BOP, GI, PPD, CAL, and PI in groups 1 and 2 following periodontal treatment took place and shown in Table 1. The changes of SOD activity (%) in serum and saliva in groups 1 and 2 at baseline and after therapy are given in Table 1 and Figs. 1, 2. Group 2 showed a better resolution of periodontal inflammation in terms of GI and BOP (%) sites as compared to group 1 (Table 2). Serum and salivary SOD activity significantly increased (P<0.01) following periodontal therapy in both groups. Improvement in systemic SOD level was significantly better in group 2 as compared to group 1 (Table 2).
DISCUSSION
The present trial is the first to evaluate the effects of micronutrient antioxidant supplementation as an adjunct to SRP on periodontal inflammatory parameters and SOD activity (serum and saliva) in postmenopausal women.
Postmenopausal women have a compromised antioxidant-oxidant balance, as demonstrated by various studies [9,10]. Estrogen is a phenolic compound that shares similarities with the structure of well-known lipophilic antioxidants such as α-tocopherol [8]. A deficiency of estrogen leads to increased levels of ROS, which then initiate the production of proinflammatory cytokines (interleukin [IL] 6, IL-8, IL-12), the activation and enhanced expression of transforming growth factor-β, the activation of various matrix metalloproteinases, and osteoclastic activation [21]. Menopause has been suggested to be a potential risk factor for the severity, progression and even initiation of periodontal disease [8,22].
The significant improvement in SOD activity in group 1 may be due to a reduction in the levels of oxidative stress associated with periodontal inflammation. Periodontal inflammation is associated with peripheral neutrophils that are hyperactive and responsible for the production of ROS such as O2-, H2O2, HOCl, and OH-, in response to Fc gamma receptor stimulation. These results are in accordance with Singh et al. [23], Kim et al. [24], and Brock et al. [11].
The significantly greater improvement in systemic SOD in group 2 as compared to group 1 may be attributed to the additional antioxidant enzyme activity resulting from the micronutrients. Studies have shown that supplementation of individual micronutrients as well as combinations thereof have beneficial effects on the antioxidant defense system. Plasma levels of micronutrients, along with some components of the enzymatic antioxidant system, are found to be increased with multinutrient supplementation [25]. This nutritional supplementation also contributed to a marginally better improvement in local SOD activity. Plasma TAOC has also been observed to be associated with dietary intake of antioxidants in postmenopausal women [26]. Copper and manganese levels in serum have been found to be significantly higher in postmenopausal women treated with HRT, patients using oral contraceptives, as well as in the second and third trimesters of pregnancy.
Excess free radicals arising from mitochondria in response to stress trigger several signalling steps that eventually produce the substances responsible for the classical signs of inflammation [27]. Normal cellular functions neutralize these ROS, thereby allowing signalling molecules such as nuclear factor-kappa-B and downstream inflammatory mediators including tumor necrosis factor (TNF)-α, inducible nitric oxide synthase, cyclooxygenese-2, and IL-1β to operate normally, leading to the maintenance of cellular health. Recent studies have also highlighted interactions between CD40 and CD40L regulating oxidative stress and signalling pathways in immunological systems [28]. Thus, a balanced ROS environment has been suggested to be a prerequisite for normal cellular health. As consumption of antioxidant micronutrients increases at the cellular level in systemic inflammation [12], micronutrient supplementation may be useful to maintain a balanced ROS environment in postmenopausal chronic periodontitis patients. Studies have suggested that antioxidant micronutrients including beta-carotene, zinc, and selenium may be effective in suppressing the activation of proinflammatory pathways through the quenching of free radical molecules [29,30]. Zinc acts as an antioxidant through the induction of metallothioneins which scavenge free radicals and bind some of the oxidants in their inert state. It is associated with the regulation of the extracellular form of SOD. It also reduces the formation of highly toxic hydroxyl ion from hydrogen peroxide [29]. Selenium is essential for the activation of glutathione peroxidase [30]. Beta-carotene is also an important member in the chain reaction of antioxidant activity [29]. A shift of balance in favour of antioxidants resulted in an improved reduction of gingival inflammation in group 2. The greater reduction in BOP (%) sites in group 2 as compared to group 1 suggests the possibility of more effective prevention of periodontal loss through adjunctive micronutrient supplementation during the maintenance phase in this population group. However, adjunctive micronutrient supplements had little impact on other periodontal parameters, e.g., PPD and CAL in postmenopausal women. Many studies observe antioxidant micronutrient depletion in periodontitis. TAOC is found to be reduced in periodontitis patients. Chapple et al. [31] found an inverse relationship between plasma vitamin C, bilirubin, and TAOC and periodontitis in National Health and Nutrition Examination Survey III data while adjusting for all known confounders in a multiple logistic regression model.
Linden et al. [32] observed significantly lower levels of α- and β-carotene, β-cryptoxanthin, and zeaxanthin in moderate and generalized severe periodontitis as compared to the remaining population.
The intake of green tea has been found to have an inverse correlation with mean pocket depth, mean CAL, and BOP [33].
Although intracellular SOD is the most prominent antioxidant in mammals [34], several authors have demonstrated the significance of extracellular SOD in plasma and other body fluids [35]. SOD is one of the most important antioxidant enzymes that convert two molecules of superoxide anion into an oxygen molecule and hydrogen peroxide.

This first step is of great importance as it prevents a further chain reaction leading to the formation of other free radicals associated with tissue damage. Moreover, the dismutation of negatively charged superoxide anion to H2O2 and O2 facilitates both the elimination of ROS, thereby moderating its effects, and the removal of H2O2 by other antioxidants. SOD has been reported to reduce periodontal inflammation and promote wound healing [36]. The local injection of SOD into joints effectively suppresses bone destruction in rat models [37]. A recent study observes systemic and local SOD levels to be lowered in chronic periodontitis. Adjunctive vitamin E supplementation was found to improve periodontal healing and antioxidant defence.
A concomitant rise in the levels of the other components of the enzymatic antioxidant system (glutathione and catalase) along with SOD activity following antioxidant supplements has been observed [30]. Therefore, all components of the antioxidant system working in synergy may be the basis for the effectiveness of micronutrient supplements in improving the outcome of root surface debridement. Collectively, these findings suggest that supplemental micronutrients may represent an important adjunctive therapeutic option in the management of chronic periodontitis in postmenopausal women. Decreased neutrophilic infiltration and reduced proinflammatory mediators, TNF-α, and IL-1β have been observed in response to a selenium-enriched diet. Selenium and manganese are both cofactors for enzymes involved in biosynthesis of glycosaminoglycans and proteoglycans.
A rigorous clinical sampling protocol and subject selection criteria were employed in this study to eliminate known confounders of enzymatic antioxidant status. Inclusion of patients belonging to a narrow age range, exclusion of smokers and the use of a highly sensitive assay kit improved the quality of the study results. Care was taken that patients of both the study groups exhibited similar oral hygiene and periodontal inflammatory status. Immunomodulation and redox balance by free radical scavenging along with providing structural precursors for healing are factors to be considered in future nutritional interventional studies.
It is concluded that adjunctive antioxidant micronutrient supplementation may be effective against oxidative stress and results in the more efficient management of periodontal inflammation in this population group. Multicentre randomized trials with large sample sizes and long-term follow-up are required to confirm the impact of micronutrients on the outcome of periodontal therapy in postmenopausal women before it can be generally recommended in a clinical setting.


 XML Download
XML Download