

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Infection with Mycobacterium tuberculosis (MTb) continues to be a major cause of morbidity and mortality throughout the world, with a disproportionate burden occurring in individuals infected with the human immunodeficiency virus (HIV). In 2015, the World Health Organization (WHO) estimated there were 10.4 million new cases of tuberculosis (TB) worldwide with 1.2 million of these in people co-infected with HIV resulting in 400,000 deaths1. HIV infected patients with latent MTb infection (LTBI) have a 5%–10% annual risk of developing active disease2. Unlike active TB, LTBI does not produce clinical symptoms and, although the host is infected, it does not result in cultivable organisms. There is no gold standard for the diagnosis of LTBI. Until recently, the diagnosis of LTBI has relied on the tuberculin skin test (TST), which is based on a delayed hypersensitivity response to MTb within the host. It has a number of limitations including cross reaction against the bacille Calmette-Guerin (BCG) vaccine strain and environmental mycobacteria, reported low sensitivity and anergy in HIV infected patients (resulting in false-negative results), operator variability and the requirement of two consultations3.
Interferon-γ release assays (IGRAs) are an attractive alternative to the TST. There are a number of commercial IGRAs that have been studied: the QuantiFERON-TB Gold in Tube (QFTGT) (Cellestis, Carnegie, Australia) and earlier versions including QuantiFERON-TB (QFT) and QuantiFERON-Gold (QFTG) assays, as well as the T-SPOT.TB (TS.TB) (Oxford Immunotec, Abingdon, UK) assay. The QFTGT measures the release of interferon (IFN)-γ by T cells, through an enzyme linked immunosorbent assay (ELISA), from a stimulated whole blood sample, in response to antigens including the region of difference 1 antigen, culture filtrate protein 10 (CFP-10), early secreted antigen target 6 (ESAT-6), and TB antigen 7.7 peptides. This assay has more antigens than the previous versions. More recently a fourth generation QuantiFERON TB Gold Plus has been released and is currently being evaluated4. In contrast to the QuantiFERON assays, the TS.TB utilizes an enzyme linked immunospot (ELISPOT) method, on a sample of peripheral blood mononuclear cells. In contrast to the TST, indeterminate results may be generated with IGRAs usually due to failure of production of IFN-γ after stimulation with a potent mitogen used as a positive control. Indeterminate results imply abnormal T-cell function or technical error5. The frequency of indeterminate IGRA results in HIV infected individuals may increase with increasing levels of immunodeficiency 6.
As there is no gold standard for the diagnosis of LTBI, the evaluation of IGRAs has been undertaken in subjects with active TB as a marker of true MTb infection. A number of studies and systematic reviews have assessed the performance of these assays in HIV negative subjects, which identified some of the advantages of the IGRA compared to the TST789. IGRA do not appear to react with exposure to certain non-tuberculous mycobacteria or BCG and test reactivity has been shown to correlate with either risk factors associated with acquisition of TB, or exposure to cases of active TB101112. However, as these assays depend on intact T-cell function it is plausible that such assays may perform differently in the immunocompromised host.
Our aim was to systematically review the performance of IGRAs and the TST in HIV infected subjects with active TB or LTBI in different TB prevalence settings.
Materials and Methods
This study was conducted and reported in concordance with PRISMA guidelines for systematic reviews13. Ethics approval was not required for completion of this systematic review.
1. Search strategy
A MEDLINE search for English language articles published between 1966 and January 2017 was undertaken. The search strategy used search terms including (TB infection OR TB disease) AND [(QuantiFERON OR ELISPOT) OR (interferon gamma release assays) OR (tuberculin skin test) OR (t-cell assay)] AND (HIV OR AIDS). Manufacturers of the commercial assays were contacted for any additional material of relevance.
2. Study selection
Three independent reviewers assessed article titles and abstracts for selection for full text review. Articles excluded were commentary, guidelines, policy, review, case studies, those with HIV negative or unknown status patients, immune reconstitution studies, in vitro studies, non-diagnostic, behavioural or modelling studies, serological, therapeutic and vaccine studies. After full text review only studies that presented data in a format allowing comparison between TST and the IGRAs were included. The population included HIV-1 or HIV-2 infected adults or children. Data from studies that recruited subjects of mixed HIV seropositivity were included only if the data pertaining to the HIV infected group could be extracted. TB referred to pulmonary or extra pulmonary disease due to MTb infection. The IGRAs included the commercial assays QFT, QFTG, QFTGT, and TS.TB. In-house ELISPOT (IHE) assays were included if they used antigens against ESAT-6 and CFP-10. Studies were included if the IGRAs were performed on samples from peripheral blood.
3. Data extraction
Once identified studies were separated into studies of active TB disease or LTBI, based on the case definitions employed by the authors, which included variable assessments of clinical, radiological (including computed tomography scan or plain X-ray), microbiological (including detection of acid fast bacilli on light microscopic examination and/or growth in culture media and/or polymerase chain reaction) and/or histological parameters as listed in the study methodology. Countries were determined to be a low incidence TB country if they reported less than 20 cases of TB per 100,000 people and/or were not one of the 63 high TB/HIV burden countries as per WHO definitions1. Study methodology and review of potential bias was extracted in a standardized format and included: recruitment method and exclusion criteria, inclusion of patients with a past history of active TB or LTBI, inpatient or outpatient setting of the study, age (classified into adult or child) and ethnicity of the study population. We assessed the laboratory methods detailed by the authors, including definitions of test positivity (for both TST and IGRA), indeterminate (IGRA only) and whether technicians were blinded to the TST result. HIV specific data including mean or median CD4 T-cell count and proportion of patients taking antiretroviral therapy were also extracted.
4. Statistical analyses
We calculated the proportion of reactive assays and 95% confidence intervals using paired data. To test the measurement of agreement between IGRA and TST Cohen's kappa statistic (k) and p-values reported in studies was used. Statistical calculators were sourced from VasserStats: Website for Statistical Computation (http://vassarstats.net/). Meta-analysis was not undertaken due to heterogeneity of study methodology (population, setting, type of IGRA, type of TST, and non-consecutive recruitment).
Results
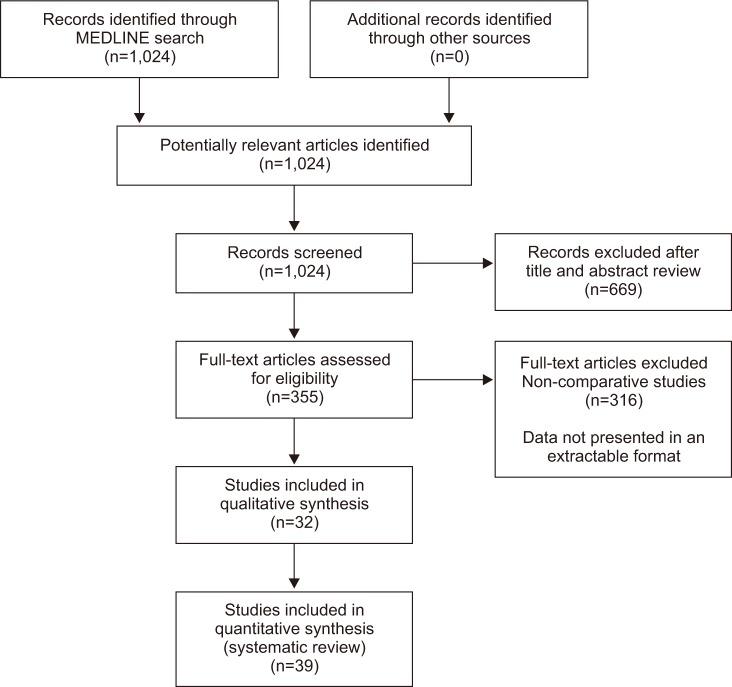
Our search identified a total of 1024 articles (Figure 1) of which 32 studies with a total of 4,856 HIV infected subjects were selected for final review.
1. Active TB disease
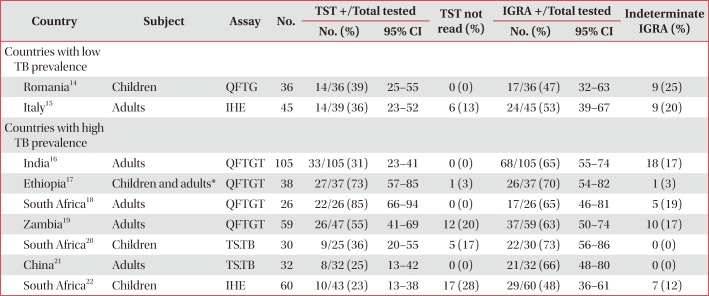
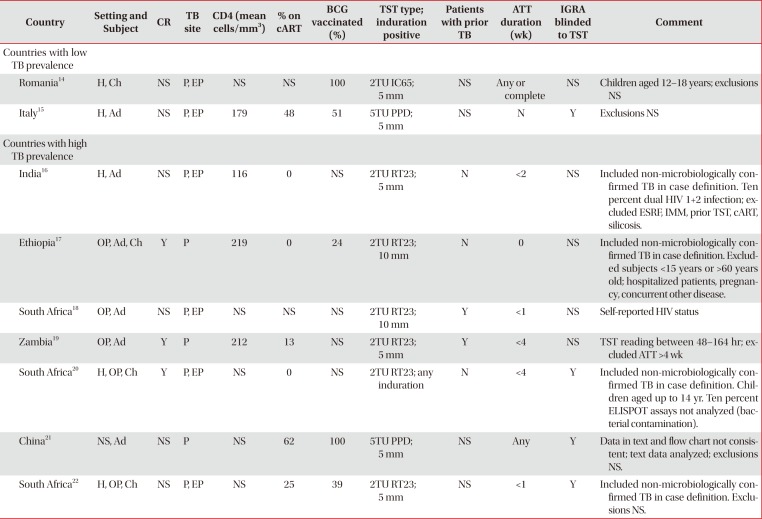
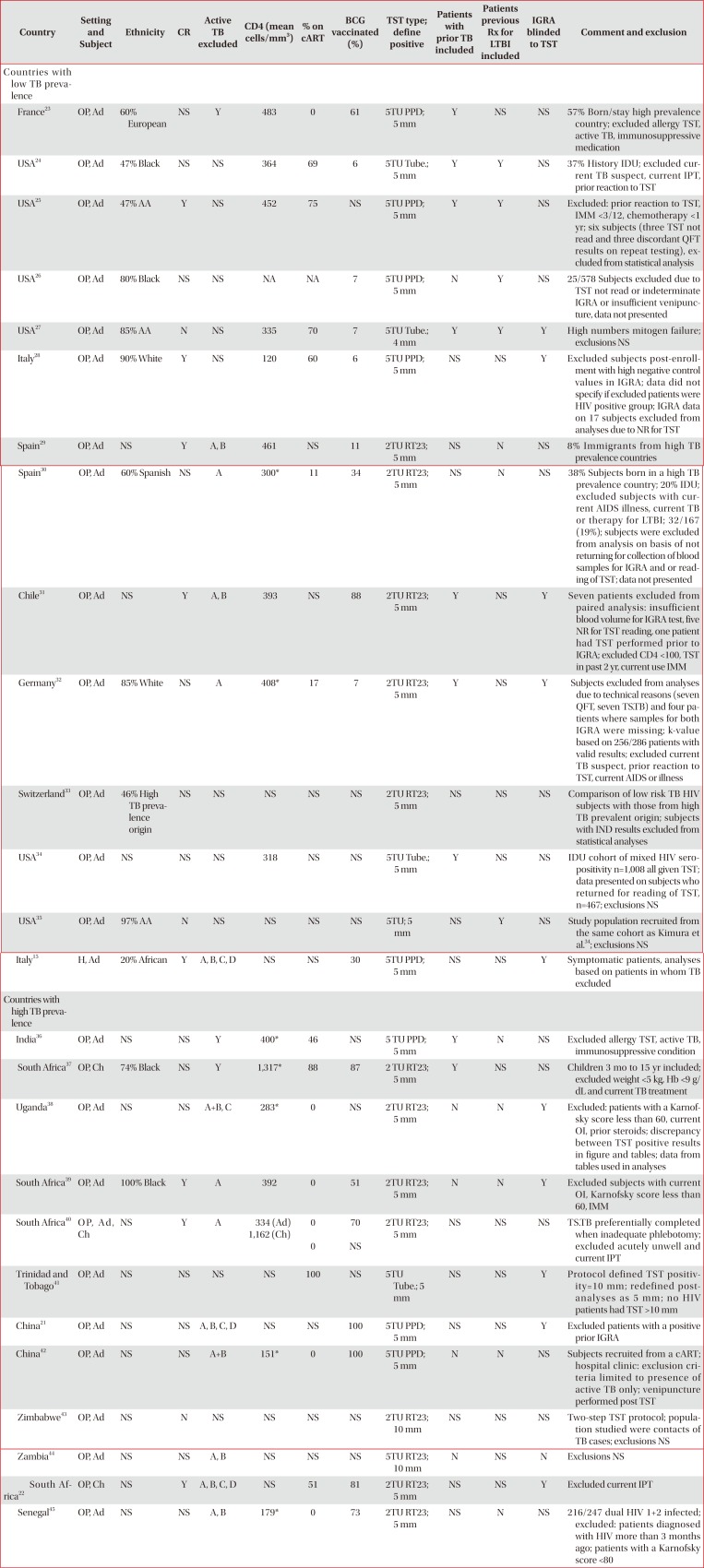
We identified nine studies in which IGRA and TST were performed in 431 patients with active TB (Table 1)141516171819202122. Only two studies1621 reported a greater proportion of positive results in IGRAs than the TST. There was inter- and intra-test variability in test positivity and proportion of indeterminate results. Concordance between the TST and QFTGT was reported in only one Indian study and was found to be low (k=0.27)16. There was considerable heterogeneity in the study design including the case definition of active TB disease and exclusion criteria including varying durations of anti-tuberculous therapy (ATT) at the time of testing (Table 2)141516171819202122.
2. LTBI
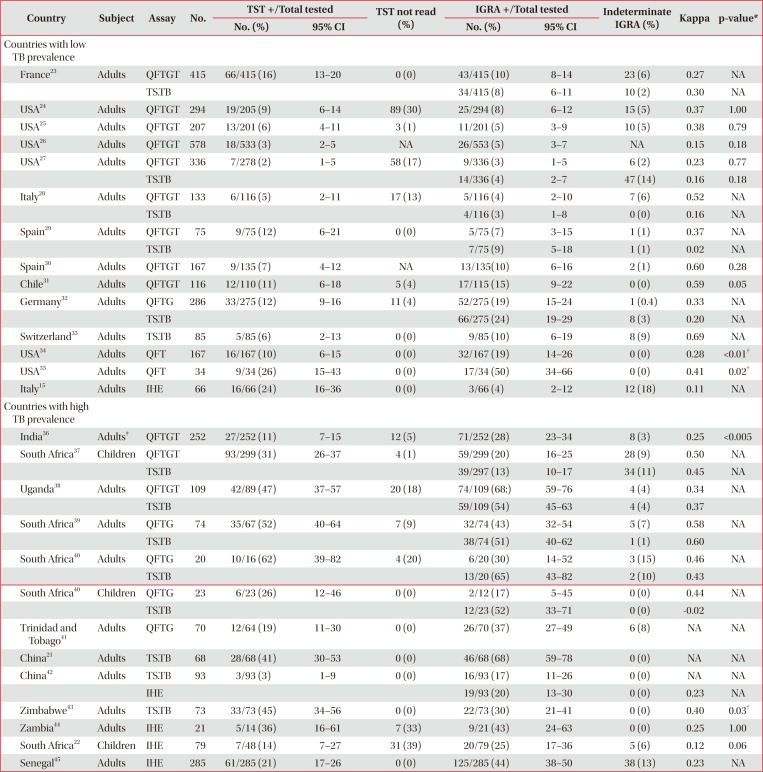
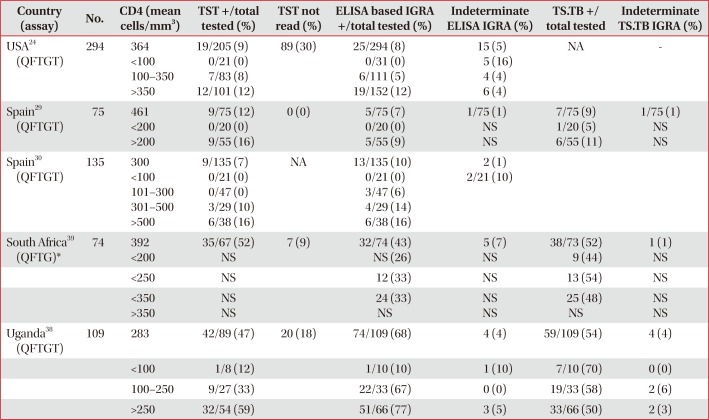
Fourteen studies from low TB prevalence countries were analysed comprising a total of 2,959 HIV adult subjects (Table 3)1521222324252627282930313233343536373839404142434445. There was significant heterogeneity in the studies (Table 4)1521222324252627282930313233343536373839404142434445. There were only three studies where significant differences between IGRA and TST were identified although the direction of difference was inconsistent. The TS.TB (but not the QFTG) had greater reactivity than the TST in one study from Germany32. In contrast the TST had greater reactivity than an IHE in an Italian study15. The TST also had greater reactivity than both the QFTGT and TS.TB in an anti-retroviral naïve French cohort23. The rate of positive reactions was higher in the first generation QFT compared to the TST based on two studies with a total sample size of 201 subjects, in which the study population were from the same cohort of mainly injecting drug users (IDU) in urban United States (Table 4)3435. These findings were not replicated with the more recent versions of the QuantiFERON assay or other IGRAs. Concordance between IGRAs and the TST ranged from extremely poor (k=0.02) to strong (k=0.69). Some authors did not present complete data on all test outcomes in subjects who were excluded from statistical analyses due to an indeterminate IGRA or “technical failure of the sample,” potentially introducing bias (Table 4)25283234. A significant proportion of subjects in some of these studies did not return to have the TST read2832.
Twelve studies (eight in adult subjects) comprising a total of 1,466 subjects (401 children) from high TB prevalence countries were analysed. There were generally higher rates of positive results in all assays (IGRAs and TST) when compared to studies that took place in lower TB prevalence settings. The results were variable with one study finding higher rates of positivity in the TST37 and five with the IGRA being positive more frequently than the TST2136384245.
Discussion
The performance characteristics of the TST, including the previously discussed limitations, are well described in HIV populations and other risk groups. Direct comparative studies of new assays with the TST provide data to assist clinicians when considering which test to use in the diagnosis of LTBI in HIV positive patients. Our analysis highlighted three main issues. Subjects with active TB had higher rates of reactivity in IGRAs when compared to the TST, although neither test type had sufficient sensitivity to be useful diagnostically. Secondly, the TST had similar rates of reactivity as the IGRAs when used in subjects without evidence of active TB. There was variability in rates of test reactivity and concordance between the TST and the different generations of the ELISA and ELISPOT based assays when all three tests were used in the same studies. Lastly, the heterogeneity of study methodology and population precluded a definitive conclusion on test superiority.
In the absence of a gold standard test for LTBI, active TB is commonly used as a surrogate when assessing the performance characteristics of IGRAs. However, they have different immunological and clinical phenotypes and are not equivalent conditions. Although this review identified that the QFTGT performed better than the TST in symptomatic patients with clinical or confirmed TB, it would not be accurate enough to exclude all cases of active TB. There was relatively limited data on the use of the TS.TB within this setting.
Studies used different criteria to include and exclude cases of active TB infection. The clinical evaluation of HIV TB co-infected patients is challenging, particularly with more advanced states of immunodeficiency. The clinical presentation can be varied with higher rates of disseminated disease, lower rates of sputum smear positivity and atypical radiological appearances 4647. This heterogeneity may affect the findings presented here.
The spectrum of the kinetics of the IGRA response to TB infection has not been established. Studies in mainly HIV negative subjects have analysed IHE during ATT, which report intra- and inter-patient variability in the measured MTb immune response and of test reversion from positive to negative in the TS.TB484950. The effect of a prior TST on an individual who subsequently has a further TST can lead to the “boosting” phenomenon, whereby an increased reaction to the injected mycobacterial antigen is observed, attributed to the immunological recall of a previous hypersensitivity reaction51. However, it is unclear how a prior TST can affect the test performance of the IGRAs. The few studies that have investigated this issue, primarily within HIV seronegative subjects, suggest the possibility of boosting the IGRA response52. The spectrum of this effect has not been established. These test performance characteristics of the IGRAs may have impacted on the studies in our review, a number of which included subjects who had been commenced on ATT (with variable treatment duration), had a prior TST, treated past TB infection or isoniazid preventative therapy prior to the IGRA being undertaken.
The population groups studied were diverse. Some of the subjects in studies from low prevalence countries included subjects born in high TB incidence countries. A number of other features varied between studies including the physical performance status of subjects, the inclusion of mainly IDU populations, the proportion of individuals on combination antiretroviral therapy, the degree of immunosuppression and HIV-2 seropositivity. Additionally, there was substantial study design differences including some studies with non-consecutive recruitment, variable definition of TST reactivity and the type and amount of purified protein derivative used.
All assays appeared to be affected by the degree of CD4 T-cell depletion, with the possible exception of the TS.TB assay. The likelihood of a positive reaction in the TST or ELISA based IGRA at lower CD4 strata appears negligible. There is insufficient data to suggest that an ELISA based IGRA performs better than the TST in patients with HIV related immunodeficiency. The proportion of indeterminate IGRA in patients with LTBI was lower than that observed in the studies in patients with active TB. This may reflect the impact of severe immunosuppression and malnutrition occurring within this patient group.
Previous studies have assessed IGRAs within HIV subjects and have reported increased “sensitivity” in diagnosing LTBI in a high and low TB prevalence settings in comparison to the TST6445354. This increased “sensitivity” usually represents increased rates of assay reactivity rather than true sensitivity as there is no gold standard. However, most of these studies did not directly compare the results of concurrent TST and IGRA testing in individual subjects. Prior systematic reviews and meta-analysis of the test performance of the IGRA in HIV infected individuals have attempted to ascertain the sensitivity and specificity of the QFTGT and TS.TB in predicting active and LTBI55565758. However, studies were included that did not perform direct comparisons with the TST and studies using older generation commercial IGRA as well as IHE and TS.TB were excluded.
There are limitations of this review. We have presented data on the first generation commercial QFT test that is no longer commonly available. Most studies had small sample sizes and study heterogeneity precluded formal meta-analysis. Finally, the data included in our review were unable to answer which test performs better in the diagnosis of LTBI due to the lack of a gold standard. We reported on cross sectional differences in test reactivity without longitudinal outcome data. A number of the studies had high non-return rates for TST reading, affecting the outcome measured for TST. This represents the operational result, rather than the intrinsic utility of the assay, although the two visits required for the test is clearly an operational challenge.
Our review of comparative data does not provide robust evidence to support the assertion that the IGRAs are superior to the TST when used in HIV infected subjects without evidence of active TB. Further longitudinal outcome studies are required to establish the prognostic value of a positive IGRA. In the interim, clinicians should be cognizant of the limitations of the data and variable test performance when considering which test to use to diagnose LTBI in this population.
 XML Download
XML Download