

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endometriosis is histopathologically defined by the presence of endometrial glands and/or stroma outside of the endometrium1. Ectopic endometriosis could be developed in many other tissues, most commonly affects pelvic organs such as ovaries, fallopian tubes, uterine ligaments, pelvic wall2. Primary cutaneous umbilical endometriosis, which is also known as Villar's nodule, is a rare manifestation of endometriosis3. Secondary endometriosis mostly occurs at surgical scar tissue after abdominal operations4. The most widely accepted pathogenesis of secondary endometriosis is the iatrogenic implantation of endometrial cells after surgery, commonly after laparoscopic procedures5. However, the pathogenesis of primary endometriosis is still unknown.
To date, umbilical endometriosis has been reported to represent about 0.4% to 4.0% of all endometriosis and accounts for 30% to 40% cases of cutaneous endometriosis. Among cutaneous endometriosis, primary umbilical endometriosis was considered even less common.
CASE REPORT
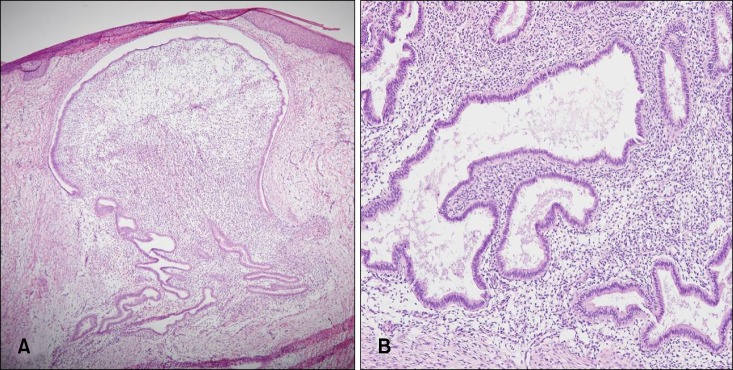
A 38-year-old multigravida female visited our department because of a painful nodule on her umbilicus. The patient recalled that the lesion was observed 2 years ago and the lesion became swollen with spontaneous frank bleeding during menstruation. The patient had no history of surgical procedure, nor any family history of malignancy. The nodule was first diagnosed as a keloid at a private clinic and had been treated with intralesional injection of steroid for several times without any signs of improvement. Physical examination revealed a 2.5×2.0-cm-sized brownish to purple colored nodule on the umbilicus (Fig. 1). Imaging studies were carried out for differential diagnosis with Sister Mary Joseph nodule and keloid. Umbilical ultrasonography showed a mass with heterogenous echogenecity, increased vascularity and abdominal computed tomography (CT) revealed enhancing mass at umbilicus without connection to abdominal organs. Histopathological examination showed dilated glandular structures surrounded by cellular endometrial-type stroma and deep perivascular infiltration of lymphocytes (Fig. 2). According to these findings, the umbilical lesion was diagnosed as primary cutaneous endometriosis and it was removed by local surgical excision. Postoperative period was unremarkable and the patient was followed up for 2 years without recurrence.
DISCUSSION
Cutaneous endometriosis represents 0.5% to 1.0% of all patients with ectopic endometriosis. Less than 30% of cutaneous endometriosis presents without prior surgical operative history, which is termed as primary spontaneous cutaneous endometriosis3. Umbilical endometriosis is composed 0.4% to 4.0% of all endometriosis, high as two-fifths of extragenital endometrioric lesions. Moreover, umbilicus is the most common site of primary cutaneous endometriosis6. Umbilical endometriosis occurs in female of reproductive age and associated symptoms are cyclic pain, bleeding and swelling of the lesion according to the menstrual cycle4.
Several possible pathogenesis of umbilical endometriosis were suggested by multiple investigators. The most commonly accepted mechanisms are lymphatic or vascular migration, cellular metaplasia, and iatrogenic metastasis5. Suggested theory includes migration of endometrial tissue from retrogression of menstruation. Survival of endometrial implants after implantation may depend on local and systemic factors. Inflammatory process is then stimulated by microvascular endothelial injury. Accordingly, it might enhance adhesion of tissue implants in outside of endometrial tissues via production of adhesion molecules such as integrin and e-cadherins7. Major etiologic pathogenesis of secondary umbilical endometriosis could be explained by iatrogenic metastasis, endometrial cells implant in scars after surgery. In comparison, primary umbilical endometriosis may be explained by the theory of vascular or lymphatic migration.
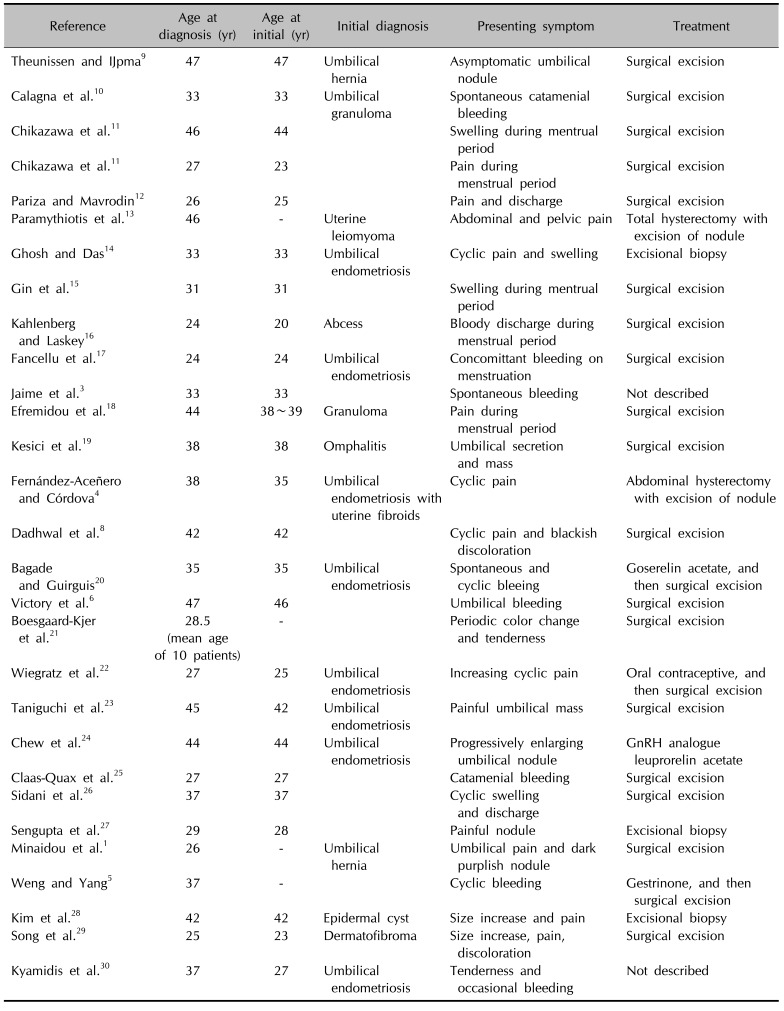
Twenty-nine published studies with primary umbilical endometriosis were identified in the literature written in English and Korean language during the period 2000~2016 (Table 1)1345689101112131415161718192021222324252627282930. Primary umbilical endometriosis is initially very rare condition, but it is now increasing in number. Based on all the reports, the mean age of patients was 35.1 years.
Differential diagnosis of umbilical endometriosis includes keloid, metastasis of visceral carcinoma, which is referred as Sister Mary Joseph nodule and melanoma3. Therefore, physicians should work on imaging studies such as ultrasonography or CT or magnetic resonance imaging. Furthermore, diagnosis must be confirmed histopathologically to exclude malignancy. More importantly, keloid is clinically very similar to umbilical endometriosis. Clinicians should pay particular attention to patients, especially history of surgery or trauma, and presenting symptoms that are related to menstrual cycle. If treatment with steroid intralesional injection does not improve the symptom, umbilical endometriosis should be considered for differential diagnosis.
Surgical excision is the definitive treatment. Hormonal therapy with gonadotropin-releasing hormone agonists, oral contraceptive and danazol can be used before surgical excision to decrease the size of the lesion and make symptom relief831. Recurrence rate is very rare9. In our case, the lesion was confirmed by umbilical ultrasonography and abdominal CT and histopathological finding, and removed by local surgical excision.
In conclusion, cutaneous endometriosis of umbilicus should now be recognized as a primary or metastatic presentation or iatrogenic complication of endometriosis. Patients with primary umbilical endometriosis should undergo careful history and physical examination to rule out potential malignancies. Moreover, differential diagnosis with keloid is very important. If the lesion diagnosed with keloid has cyclic symptoms with menstrual period, and does not improve with treatment, umbilical endometriosis should be suspected. Surgical excision is the treatment of choice to prevent recurrence and to reduce the risk of malignant transformation.

 XML Download
XML Download