

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Many recent trials have investigated the relationship between the presence of chronic total occlusion (CTO) and mortality in various populations. It has been found that the presence of CTO is associated with a higher mortality rate in patients with acute myocardial infarction, multi-vessel disease (MVD), or left main disease.123456 The presence of CTO has also been shown to be associated with a reduced left ventricular ejection fraction (LVEF; <40%) and further deterioration of LVEF in ST-segment elevation myocardial infarction (STEMI) patients.5 In the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter) registry, 61% of CTO patients were treated with medical therapy (MT), while only one third (39%) were treated with early coronary revascularization by percutaneous coronary intervention (PCI; 24%) or coronary artery bypass graft surgery (CABG; 15%).7 Similarly, according to the NCDR (National Cardiovascular Data Registry) database in the United States, the CTO-PCI attempt rate was below −15% between 2004 and 2007, whereas the CABG rate was 18.3%.89
Recently, it has been reported that successful CTO-PCI is associated with improvements in left ventricular function, reducing angina symptoms and reducing the need for CABG, compared with failed CTO-PCI.91011 Additionally, there are studies that report successful CTO-PCI may have an edge on long-term survival.111213141516 Nonetheless, only limited data on comparisons of successful CTO-PCI with conservative MT are available, particularly in the drug-eluting stent (DES) era.17 The aim of this study was to compare the long-term clinical outcomes of successful CTO-PCI with DESs to those of CTO-MT, particularly in a series of the Korean population.
MATERIALS AND METHODS
The design of this registry has been introduced before.17 We obtained data from the CTO registry of Korea University Guro Hospital (KUGH), Seoul, Korea. In brief, it is a single-center, prospective, all-comer registry designed to reflect “real-world” practice since 2004, after the introduction of DESs. Data were collected by a trained study-coordinator with a standardized case report form. The participants or their legal guardians were given a thorough literal and verbal explanation of the study procedures before granting written consent to participate in the study. The study protocol was approved by the Medical Device Institutional Review Board of KUGH. The authors of this manuscript have certified that the information contained herein is true and correct as reflected in the records of the Medical Device Institutional Review Board (#MD07014).
Data source and population
A total of 4909 consecutive patients were diagnosed with significant coronary artery disease (≥70% of coronary stenosis) by coronary angiography. Among these, 840 patients who had CTO lesion on the coronary main vessels were enrolled in KUGH-CTO registry from January 2004 to November 2015. 20.9% (176/840) of all CTO patients had a CTO lesion when they visited acute myocardial infarction and were treated conservatively with MT or staged PCI for CTO lesions.
Study definitions
A CTO lesion was defined as a complete obstruction of the coronary vessel by thrombolysis in myocardial infarction (MI) flow grade 0 for at least 3 months. The coronary main vessels were defined as having a reference vessel diameter (RVD) of >2.5 mm, and CTO lesion must be located on the main vessel at left main, left arterial descending (LAD), left circumflex, right coronary, and ramus artery. Patients were excluded if they had CTO in a small vessel (RVD, ≤2.5 mm) or located on side branch vessels, such as an acute marginal, diagonal, septal and obtuse marginal artery. Major adverse cardiovascular events (MACEs) were defined as the composite of total death, MI, and revascularization, including PCI and CABG. Total deaths were considered cardiac unless an unequivocal non-cardiac cause of death could be confirmed. MI after discharge and in-hospital fatal MI were termed as recurrent MI, defined as either the development of pathological Q wave in at least two contiguous leads or an elevation of serum creatine kinase levels. After the CTO procedure, the periprocedural MI (p-MI), simply increased the cardiac marker, was not included.
Statistical analysis
For continuous variables, differences between groups were evaluated using the unpaired t-test or Mann-Whitney rank test. Data are expressed as mean±standard deviations. For discrete variables, differences are expressed as counts and percentages, and were analyzed with the χ2 or Fisher's exact test. To adjust for any potential confounders, propensity score matching (PSM) analysis was performed using the logistic regression model. We tested all available variables that could be of potential relevance: age, male, cardiovascular risk factors (hypertension, diabetes, dyslipidemia, cerebrovascular disease peripheral artery disease, chronic kidney disease, heart failure and smoking), and angiographic and procedural characteristics (significant coronary lesion artery, CTO lesion artery, lesion locations). Matching was performed via 1:1 matching protocol using the nearest neighbor matching algorithm, with a caliper width equal to 0.05 of the standard deviation of the propensity score, yielding 265 well-matched pairs. Various clinical outcomes up to 5 years were estimated by the Kaplan-Meier analysis, and differences between groups were compared with the log-rank test before and after PSM. Proportional hazard models were used to assess the hazard ratio (HR) of the CTO-PCI group in comparison to the CTO-MT group among the matched population. For all analyses, a two-sided p<0.05 was considered statistically significant. All data were processed with SPSS (version 20.0, IBM Corp., Armonk, NY, USA).
Study endpoints
Primary endpoint was total death, MI, revascularization, such as PCI and CABG, and MACE. The secondary endpoint was the level of change in left ventricular function before and after CTO-PCI within 6 months and 2 years. In this study, the mean follow-up period was 1466±586 days (after PSM: 1446±587), and we could follow up on the clinical data of all enrolled patients through face-to-face interviews at regular outpatient visits, medical chart reviews, and telephone contacts.
RESULTS
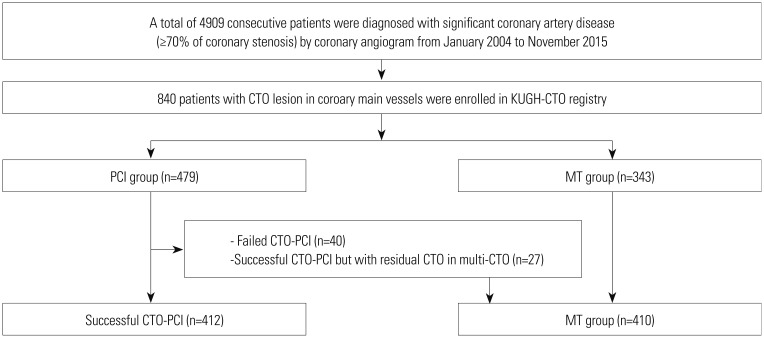
In the present study, 17.1% (840/4909) of patients with significant coronary artery disease diagnosed by coronary angiography had a CTO lesion. Of the 59% of the CTO patients, 479 (57%) of them underwent an early coronary revascularization by PCI and 18 (2%) underwent a CABG. Finally, 412 patients were enrolled in the successful CTO-PCI group and 410 were enrolled in the CTO-MT group, which included 343 patients with conservative MT, 40 patients with failed CTO-PCI and 27 patients who underwent a successful CTO-PCI, but with residual CTO in the multi-CTO lesion (≥2 vessel) (Fig. 1). The overall procedural success rate of CTO-PCI was 85% (452/532 lesion).
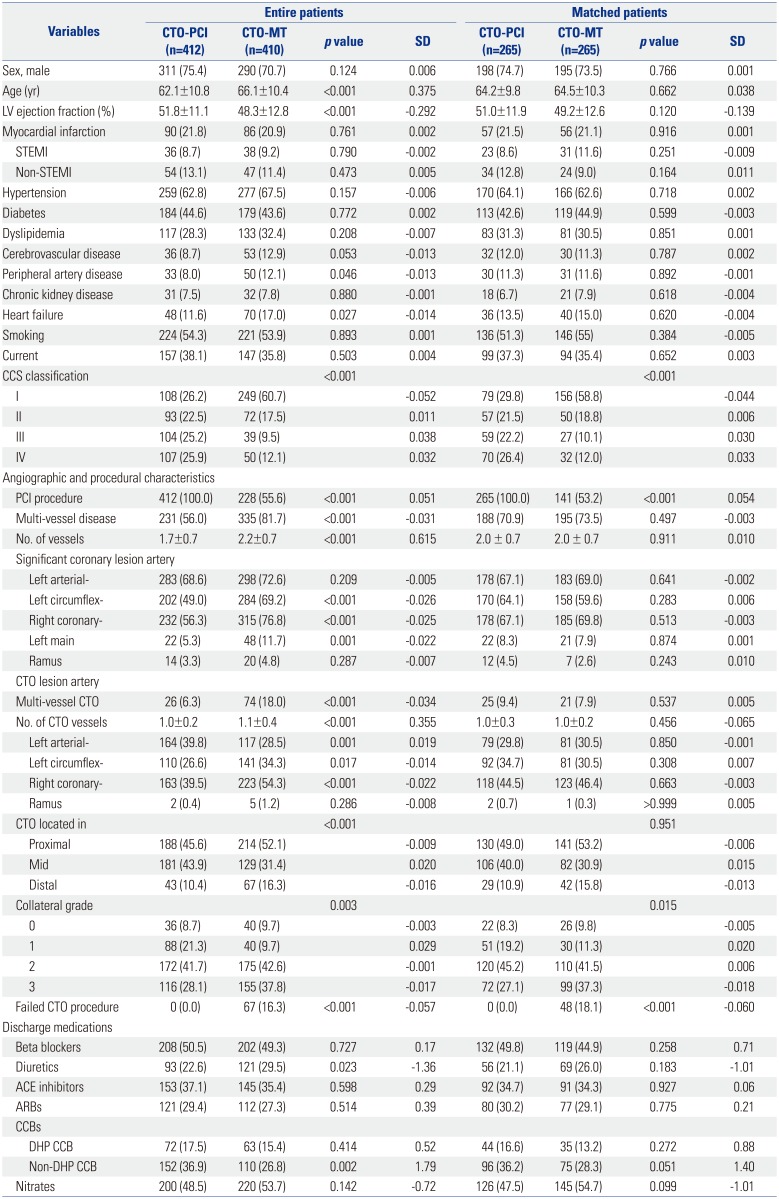
Baseline clinical, angiographic and procedural characteristics are shown in Table 1. In the entire cohort, unfavorable risks, such as old age, lower LVEF, peripheral artery disease, heart failure, MVD, multi-vessel CTO and proximal-CTO, were more common in the CTO-MT group, whereas angina symptom (Canadian Cardiovascular Society class, CCS≥II), LAD-CTO, and lower collateral grade were more prevalent in the CTO-PCI group, reflecting real-world clinical practice. After PSM analysis, two propensity-matched groups (265 pairs, n=530) were generated, and the baseline characteristics were balanced, except that angina symptom and collateral grade were more favorable in the CTO-MT group.
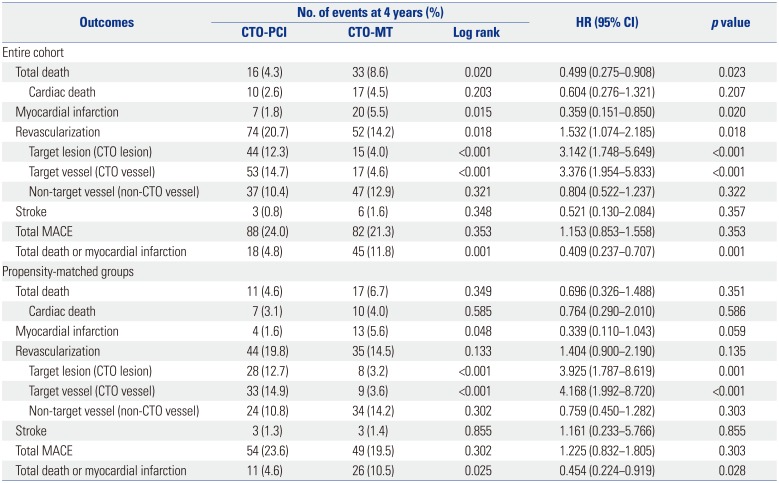
Various clinical outcomes of the 5-year follow up (mean duration: 4.0±1.5 years) were analyzed by Cox-proportional hazard ratio model analysis and Kaplan-Meier curved analysis, as shown in Table 2. In the entire cohort, the CTO-PCI group exhibited a lower incidence of total death, MI, and a composite of total death and MI, but had a higher incidence of revascularization, including target CTO-lesion (target lesion revascularization, TLR) and target CTO-vessel (target vessel revascularization, TVR). After propensity-matching, although the CTO-PCI group demonstrated a higher incidence of revascularization (TLR and TVR), it showed a lower incidence of MI and composite of total death or MI, compared with the CTO-MT group. In the Cox-proportional hazard ratio model analysis, compared with the CTO-MT group, the CTO-PCI group tended to exhibit a lower risk of MI [HR: 0.339, 95% confidence interval (CI): 0.110 to 1.043, p=0.059], and a significantly reduced risk of composite total death and MI (HR: 0.454, 95% CI: 0.224 to 0.919, p=0.028) (Table 2, Supplementary Fig. 1, only online).
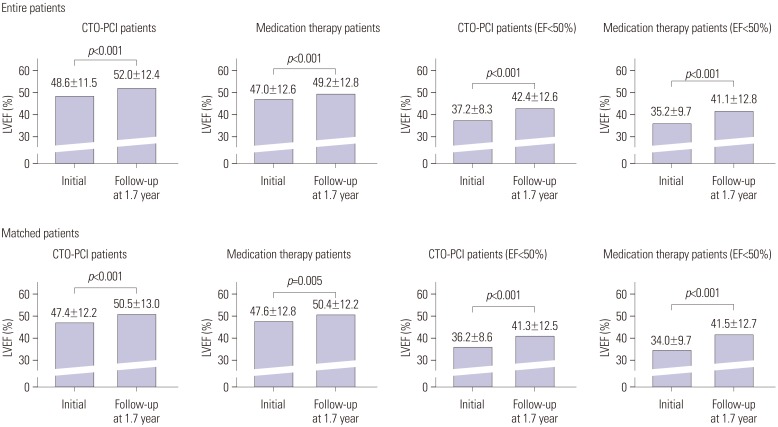
To evaluate changes in LVEF in the first 1.7 years, paired t-test analysis was applied. Both the successful CTO-PCI group and CTO-MT group were associated with a significant improvement in mean LVEF from 48.6% to 52.0% and from 47.0% to 49.2%, respectively. The two groups also showed a significant improvement in mean LVEF among individuals with reduced LVEF (<50%) (Fig. 2).
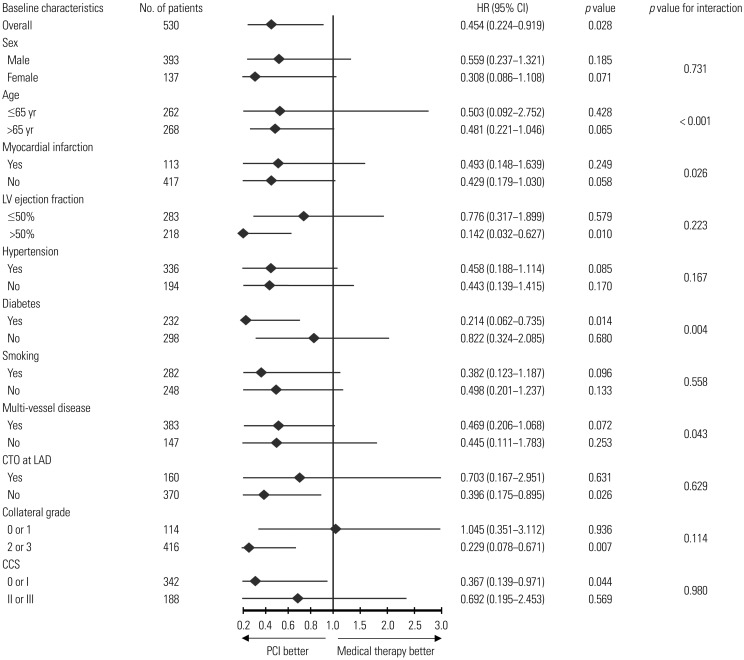
Subgroup analyses were performed to compare the composite of total death and MI of the successful CTO-PCI and CTO-MT groups with Cox-proportional hazard ratio model analysis (Fig. 3). The CTO-PCI group showed a more beneficial effect in individuals with preserved LVEF (>50%), diabetes, non-LAD CTO, well-developed collateral vessel (grade≥2), and lower grade CCS (≤Class I).
DISCUSSION
The main findings of this study are as follows: 1) successful CTO-PCI with DESs, as compared with CTO-MT, reduced the incidence of MI and composite of death or MI over 5 years of follow up. However, 2) during the 1.7 years of follow up, LVEF significantly improved in both the CTO-PCI group and the CTO-MT group. 3) According to the results of sub-group analysis, CTO-PCI may be more effective in patients with diabetes, preserved myocardial viability, such as preserved LVEF (>50%), CTO located in non-LAD arteries, well-developed collateral vessel (>grade 1), and mild chest pain (<CCS class II).
The aim of the present study was to compare CTO-PCI with DESs and CTO-MT in regards to risk of major individual and composite clinical outcomes, as well as the impact of revascularization on serial LV function. Many trials have investigated the relationship between the risk of mortality and CTO in various populations.123456 The HORIZONS-AMI trial reported that the presence of CTO was an independent predictor of both increased early (within 30 days, HR: 2.88, 95% CI: 1.41–5.88, p=0.004) and late mortality (from 30 days to 3 years, HR: 1.98, 95% CI: 1.19–3.29, p=0.009) in STEMI patient.2 The PL-ACS study, reported CTO was an independent predictor of 1-year mortality (HR: 1.42, 95% CI: 1.01–2.00, p=0.047) in patients with non-STEMI.3 In addition, Claessen, et al.5 reported that CTO is associated with reduced LVEF (<40%) and further deterioration of LVEF, as well as an increased risk of long-term mortality, in STEMI patients.
To date, compared with CTO-MT, the effects of CTO-PCI are controversial, and data on a fair comparative assessment of successful CTO-PCI and CTO-MT are limited. Recent studies concluded that successful CTO-PCI is associated with a better long-term survival rate than failed CTO-PCI.111213141516 Mehran, et al.14 reported that successful CTO-PCI reduced long-term cardiac death by 60% during a 5-year follow-up. The Multicenter Korean-Chronic Total Occlusion (K-CTO) registry indicated that successful CTO-PCI reduces the risk of composite cardiac death or MI to 49% during 2 year follow-up study.18 However, these studies had some limitations for application in the real world: CTO-PCI attempt rates were below 15% on average,9 and CTO-PCI exhibited a considerably low procedural success rate (60% to 86%), compared with PCI for non-CTO (98%).14192021 Also, compared with CTO-MT, failed CTO-PCI may have a higher risk for worse clinical outcomes due to procedural coronary injuries, procedural complications, and p-MI.22232425 The incidence of p-MI was reported in 5.4% to 13.8% of CTO patients.22232425 Lo, et al.25 reported that p-MI raised the risk of MACEs (HR: 2.25, p<0.01) during 2.3 years. Godino, et al.26 showed that failed CTO-PCI was associated with a higher incidence of CABG (6.0% vs. 0.7%, p=0.01), but not with death or MACEs over 4 years, compared with CTO-MT.
Comparing the aforementioned trials with the present study, we recorded similar long-term clinical outcomes.11121314151618 Compared with CTO-MT, in the propensity-matched cohort, CTO-PCI reduced the risk of a composite of death or MI by 55% (95% CI: 9–78%, p=0.028) up to 5 years of follow up. Also, LVEF significantly improved in the CTO-PCI group, as well as in the CTO-MT group in the first 1.7 years of follow up. Claessen, et al.5 reported that CTO is associated with a reduced LVEF (HR: 3.5, 95% CI: 1.6 to 7.8) and further deterioration of LVEF (HR: 1.9, 95% CI: 1.3 to 2.8), whereas MVD alone is not associated with reduced LVEF in STEMI patients.
However, we failed to estimate the survival benefits of CTO-PCI, compared with CTO-MT, which may have been due to the insufficient sample size (matched pair=265, total=530), and PCI for the non-CTO lesion. In the present study, the incidence of MVD was 69% (matched population in 72%). 55.6% of CTO-MT patients received PCI procedures (matched population in 53.2%). We speculate that almost all of the CTO patients were treated for clinically-significant non-CTO lesion at their physicians' discretion. Published data have shown that CTO and MVD are reliable independent predictors of long-term mortality.246 Therefore, complete revascularization or CABG may confer a long-term survival benefit in CTO patients.1527 Also, PCI for a non-CTO lesion in CTO patients with MVD may be helpful for the development of collateral vessels, which may be of relevance for myocardial recovery.1028 Therefore, we carefully suggest that PCI can improve the quality of life for both non-CTO and CTO lesion patients through dyspnea and symptom relief via improving left ventricular function.
Although CTO-PCI with DESs in this study reduced the risk of the composite of death or MI, it raised the risk of repeat revascularization: TVR (HR: 4.16, 95% CI: 1.99–8.72) for treated CTO. The incidences of TLR and TVR were 12.7% and 14.9%, respectively, for treated CTO. Published data have shown that the incidences of TVR for stent-treated CTO were 11.6% for DESs and 15.6% for bare-metal stents at 3 years.29 The re-occlusion problems of stents still remained for CTO-PCI.
In subgroup analyses of the composite of total death and MI in propensity-matched groups, CTO-PCI showed a more beneficial effect in individuals with preserved LVEF (>50%), diabetes, non-LAD CTO, well developed collateral vessels (grade≥2), and a lower grade of CCS (≤Class I). Commonly, patients with diabetes have high mortality risk and prevalence of MVD.4 As previously mentioned, successful CTO-PCI improves left ventricular function, which may be helpful to CTO patients with diabetes.5 Also, patient population groups of preserved LVEF (>50%), CTO located in non-LAD, well-developed collateral vessel (>grade 1), and mild chest pain (<CCS class II) are at a relatively lower risk for mortality or MI, compared with their respective counterparts. In these patient groups, successful CTO-PCI may be offered for protective effects against further events. However, further observational studies, sub-analyses, and well-designed randomized trials with larger study populations are needed to confirm these findings.
There are some limitations to this study. First, the present study was analyzed retrospectively, although PSM analysis was performed to minimize confounding factors that might have influenced the results otherwise. Also, the registry was designed with an all-comer prospective registry from 2004. However, we could not adjust for all limiting factors not shown through medical records or collected through telephone contacts. Second, CTO-PCI requires a high level of procedural skill, and the effects of treatment are controversial. Therefore, treatment selection of CTO lesions, such as CTO-MT or CTO-PCI, depended on physician discretion in this study. Also, while PSM was used to minimize selection bias, it is impossible to eliminate these biases completely. Third, the CTO-MT group included 67 patients of unsuccessful CTO-PCI. These patients were survivors who were discharged after PCI, which also might have influenced the results. We only included patients with failed CTO-PCI without major procedure-related complications to minimize bias. Also, in the present study, we failed to identify any clinical differences up to 5 years between the failed CTO-PCI group and the CTO-MT group (Supplementary Fig. 1, only online). Lastly, the present study was undertaken as an observational study, and therefore, well-designed randomized trials are needed to confirm these findings.
 XML Download
XML Download