

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The presence of myocardial ischemia is the most important prognostic factor in patients with coronary artery disease (CAD),1)2)3) and revascularization should be performed for ischemia-causing stenoses. Numerous efforts have been made to detect myocardial ischemia using non-invasive tests. However, only 44.5% of patients underwent non-invasive stress testing prior to elective invasive coronary angiography in real world practice.4) In addition, about 60% of patients with positive non-invasive tests were reported to have no significant obstructive disease upon invasive coronary angiography.5) Therefore, we need a better understanding and more precise diagnostic method for clinically relevant ischemia. In this regard, invasive physiologic assessment has been used for risk stratification and selection of appropriate treatment strategy in the cardiac catheterization laboratory.
Among the invasive physiologic indices, fractional flow reserve (FFR) has been regarded as a reference to define ischemia-causing stenosis in patients without clear evidence of inducible myocardial ischemia.6)7) The development of resting pressure-derived index, instantaneous wave-free ratio (iFR), has served to expand the general applicability of invasive physiologic assessment. Furthermore, there have been continuous efforts to expand the indication and role of invasive physiologic assessment. Nevertheless, there are still some issues that remain to be clarified to fill the gap between evidence and patient care. As such, the following issues will be discussed in this review:
RESTING VERSUS HYPEREMIC PRESSURE-DERIVED PHYSIOLOGIC INDICES
FFR has been the most commonly used invasive physiologic index to detect functionally significant stenosis in the cardiac catheterization laboratory. Previous key FFR trials (DEFER, Fractional Flow Reserve versus Angiography for Multivessel Evaluation [FAME], and FAME II trials) demonstrated 3 important messages. First, DEFER trial showed that FFR-based deferral of revascularization for functionally insignificant stenosis was safe up to 15 years of follow-up and revascularization for those lesions could not improve the prognosis.8) The DEFER-DES trial, which was conducted in the era of drug-eluting stents, also showed similar results to the DEFER trial.9) Second, FAME trial showed that FFR-guided strategy reduced the risk of major adverse cardiac events compared with an angiography-guided strategy, with less use of stents per patient, contrast media, and medical cost.10) Recently published 5-year follow-up data showed no late catch-up of events in the FFR-guided group.11) Third, FAME II trial clearly showed that medical treatment alone for patients with functionally significant stenosis was associated with significantly higher risk of clinical events, compared with FFR-guided percutaneous coronary intervention (PCI). Based on these results, the current European guideline recommends FFR-guided revascularization as class I (level of evidence A) in stable patients when evidence of ischemia is not available,7) and the appropriate use criteria strongly support FFR-guided PCI in management of patients with stable CAD.12)
While additional clinical evidence on FFR is being established, another group focused on a pressure-derived index which can be measured during resting condition. The concept of iFR was originally derived from wave-intensity analysis using both intracoronary pressure and flow velocity data. Davies et al.13) observed a certain period in the cardiac cycle during which the resistance is low and stable.14) iFR is calculated by distal coronary pressure (Pd)/aortic pressure (Pa) ratio at the wave-free period during resting state and does not require hyperemia (Figure 1). Recent 2 large randomized trials showed that clinical outcomes of an iFR-guided strategy were not inferior to that of a FFR-guided strategy.15)16)
Figure 1
Resting and hyperemic pressure-derived invasive physiologic indices. Resting Pd/Pa is measured during the entire cardiac cycle and iFR is measured during “wave-free period” at resting status. Conversely, FFR is measured during the entire cardiac cycle at maximal hyperemia.
FFR = fractional flow reserve; iFR = instantaneous wave-free ratio; Pa = aortic pressure; Pd = distal coronary pressure; Resting Pd/Pa = resting distal to aortic coronary pressure.

DISCORDANCE BETWEEN RESTING AND HYPEREMIC PHYSIOLOGIC INDICES
After the first-in-man study (ADenosine Vasodilator Independent Stenosis Evaluation [ADVISE]) which showed a high diagnostic performance of iFR to predict FFR, there has been debate regarding the clinical relevance and diagnostic performance of iFR.17)18)19)20) Since the 2 pressure-derived indices are measured during different conditions, i.e., FFR under maximal hyperemia versus iFR under resting status, it may be natural to have discordant results in some patients. The incidence of discordance between FFR and iFR was reported to be 10–30% (Table 1) and the mechanism of this discordance and its clinical relevance are under active investigation.
Table 1
Proportion of discordance between FFR and iFR in previous studies
| Study | Sample size | Used cut-off of iFR | Reference cut-off of FFR | Diagnostic accuracy of iFR (%) | Proportion of discordance (%) |
|---|---|---|---|---|---|
| ADVISE, 201245) | 157 lesions | ≤0.83 | ≤0.80 | 93 | 7 |
| ADVISE registry, 201346) | 339 lesions | ≤0.89 | ≤0.80 | 80 | 20 |
| Korean Registry, 201318) | 238 lesions | ≤0.90 | ≤0.80 | 82 | 16 |
| VERIFY study (retrospective), 201317) | 500 lesions | ≤0.80 | ≤0.80 | 60 | 40 |
| ≤0.83 | ≤0.80 | 68 | 32 | ||
| ADVISE In-Practice registry, 201447) | 392 lesions | ≤0.90 | ≤0.80 | 80 | 20 |
| ≤0.85 | ≤0.75 | 88 | 12 | ||
| RESOLVE study (retrospective), 201420) | 1,593 lesions | ≤0.90 | ≤0.80 | 80.4 | 19.6 |
| ADVISE II registry, 201548) | 690 lesions | ≤0.89 | ≤0.80 | 82.5 | 17.5 |
| VERIFY II registry, 201649) | 257 lesions | ≤0.90 | ≤0.80 | 79 | 21 |
| Contrast study, 201650) | 763 patients | ≤0.89 | ≤0.80 | 79.9 | 20.1 |
| IDEAL substudy, 201651) | 362 lesions | ≤0.89 | ≤0.80 | 87.3 | 12.7 |
| 3V-FFR-FRIENDS registry32), Subgroup Analysis 201724) | 975 lesions | ≤0.89 | ≤0.80 | 88.2 | 11.8 |
| 3V-FFR-FRIENDS registry32), Defer Subgroup, 201725) | 821 lesions | ≤0.89 | ≤0.80 | 91.2 | 8.8 |
ADVISE = ADenosine Vasodilator Independent Stenosis Evaluation; FFR = fractional flow reserve; IDEAL = Iberian-Dutch-English Collaborators; iFR = instantaneous wave-free ratio; Pa = aortic pressure; Pd = distal coronary pressure; RESOLVE = Multicenter Core Laboratory Comparison of the Instantaneous Wave-Free Ratio and Resting Pd/Pa With Fractional Flow Reserve; VERIFY = VERification of Instantaneous Wave-Free Ratio and Fractional Flow Reserve for the Assessment of Coronary Artery Stenosis Severity in EverydaY Practice; 3V-FFR-FRIENDS = 3-vessel fractional flow reserve for the assessment of total stenosis burden and its clinical impact in patients with coronary artery disease.
Lee et al.21) investigated 115 patients with left anterior descending artery stenosis who underwent both 13N-ammonia positron emission tomography (PET) and invasive physiologic assessment and found that the threshold of iFR matched with a more severe stenosis level than that for FFR (Figure 2). In another 13N-ammonia PET study,22) lesions with low FFR and high iFR showed higher hyperemic myocardial blood flow and coronary flow reserve (CFR) compared with the concordant abnormal group (p=0.003 and p<0.001, respectively). In addition, the discordant group showed a significantly lower proportion of PET-defined myocardial ischemia than the concordant abnormal group (p=0.010). These results illustrate the difference between resting and hyperemic physiologic indices, and explain why iFR-guided revascularization strategy has resulted in less revascularization than FFR-guided revascularization strategy in the DEFINE-FLAIR and iFR-SWEDEHEART trials.15)16)
Figure 2
Changes of FFR and iFR according to anatomical and hemodynamic stenosis severity. Regardless of (A) anatomical or (B) hemodynamic epicardial stenosis severity indices, the iFR threshold for separating normal from abnormal values matches with a more severe stenosis level than that for FFR. This figure was modified from the original version.21)
FFR = fractional flow reserve; iFR = instantaneous wave-free ratio.

As for the mechanism of discordance, a recent publication by Cook et al.23) showed that iFR represented coronary flow velocity and CFR better than FFR. Lee et al.24) investigated clinical and angiographic lesion characteristics among 4 groups classified according to FFR and iFR; concordant normal (group 1: FFR>0.80 and iFR≥0.90); high FFR and low iFR (group 2: FFR>0.80 and iFR<0.90); low FFR and high iFR (group 3: FFR≤0.80 and iFR≥0.90); and concordant abnormal (group 4: FFR≤0.80 and iFR<0.90). Angiographic stenosis severity and SYNTAX score were increased from group 1 to group 4 (all p<0.001) and FFR decreased proportionally from group 1 to group 4 (all p<0.001). In a multivariable predictive model, females, diabetes mellitus, smaller reference vessel diameter, and higher angiographic stenosis severity were associated with low iFR among high FFR group. Conversely, males, absence of diabetes mellitus and lower angiographic stenosis severity were associated with high iFR among low FFR groups.24) These results support the concept that the discordance between resting and hyperemic pressure-derived indices originates from a complex interaction among clinical characteristics, severity or geometry of the epicardial coronary stenosis, and difference in resting and hyperemic coronary physiologic behaviors. Therefore, lesions with discordance between FFR and iFR may need to be interpreted as a unique physiological and clinical entity.22)
Since both DEFINE-FLAIR and iFR-SWEDEHEART trials adopted exclusive allocations between FFR and iFR-guided strategy groups, the outcomes of deferred lesions with discordant results could not be investigated.15)16) In a substudy of the 3-vessel fractional flow reserve for the assessment of total physiologic atherosclerotic burden and its clinical impact in patients with coronary artery disease (3V-FFR-FRIENDS) study, 2-year clinical events of 821 deferred lesions with both FFR and iFR data were analyzed.25) Among 4 groups classified according to FFR and iFR levels, only the group with concordant abnormal results showed a significantly higher risk of clinical events compared with concordant normal group (hazard ratio [HR], 7.71; 95% confidence interval [CI], 2.62–22.67) and the discordant results between FFR and iFR were not associated with increased risk of clinical events. Although this issue needs further investigation, this study at least demonstrated the benefit of comprehensive physiologic assessment for both resting and hyperemic status. However, it should be noted that iFR can be more vulnerable to patient baseline conditions and measurement artifacts. When the maximum variability in estimated event rates, which is influenced by inherent measurement variability of each index was compared,26) FFR showed a lower maximum variability in estimation of future event rates compared with that of iFR, despite a similar relationship with clinical events (Figure 3).
Figure 3
Association of FFR and iFR with clinical outcomes and the variability in estimated event rates due to intrinsic measurement variability. (A) Both FFR and iFR showed significant association with the estimated 2-year event rates. (B) FFR and iFR showed differences in the variability of the estimated event rates according to the approximate measurement variability. FFR showed lower maximum variability compared with that of iFR. This figure was modified from the original version.25)
CI = confidence interval; FFR = fractional flow reserve; HR = hazard ratio; iFR = instantaneous wave-free ratio.

PRESSURE WIRE ASSESSMENT BEYOND A PER-VESSEL DECISION FOR REVASCULARIZATION
Routine application of pressure wire assessment can alter treatment strategy. Previous studies showed that the per-patient level treatment decision was changed in 26–45% of patients after routine FFR measurement.27)28)29) Ahn et al.30) showed that the routine incorporation of FFR in real practice improved PCI outcomes. In patients with left main disease or 3-vessel disease, the outcomes of PCI were comparable to those of coronary artery bypass graft surgery after routine use of FFR.30) In addition, several studies have demonstrated the prognostic implication of FFR as a continuous variable. In a study by Johnson et al.,31) there was a significant inverse relationship between per-vessel FFR values and normalized 1-year rate of clinical events. Simply speaking, patients with low-normal range of invasive physiologic index have higher risk of future events than those with higher or near normal FFR values. This concept of “risk continuum of FFR” was reproduced in another study (Figure 4).32)
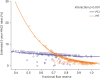
Figure 4
Risk of clinical events in medically treated and revascularized vessels according to FFR. The 2-year MACE rates were plotted according to pre-intervention native vessel FFR in medically treated vessels and stented vessels. The relationship between native vessel FFR and clinical outcome was different between medically treated vessels and stented vessels. In medically treated vessels with FFR<0.75, the risk of 2-year MACE was exponentially increased. In stented vessels with pre-intervention FFR>0.75, the MACE risk was higher than medically treated vessels. This figure was adapted from the authors' original work under permission of the publisher.32)
FFR = fractional flow reserve; MACE = major adverse cardiac events; MT = medical treatment; PCI = percutaneous coronary intervention.
The 3V-FFR-FRIENDS study investigated the clinical relevance of total physiologic atherosclerotic burden assessed by the sum of FFR in 3 major epicardial vessels (3V-FFR).32) The primary hypothesis was that patients with low 3V-FFR would have a higher 2-year clinical event rate than those with high 3V-FFR. In 1,136 patients (3,298 vessels), the median value of 3V-FFR was 2.72 (interquartile range, 2.57–2.79) and the low 3V-FFR group showed a higher event rate than the high 3V-FFR group (7.1% vs. 3.8%; HR, 2.21; 95% CI, 1.20–4.05). In addition, the 3V-FFR value showed significant negative association with the estimated event rate and the difference between the high and low 3V-FFR groups was maintained among patients with per-vessel FFR>0.8 in all 3 vessels (12.6% vs. 3.7%; HR, 3.92; 95% CI, 1.16–12.23).
Although current guidelines do not recommend FFR measurement in stenosis with <40–50% diameter stenosis,6)7) approximately 16% of lesions with percent diameter stenosis <50% showed an FFR of <0.80 in the RIPCORD study.27) Furthermore, a substudy of the 3V-FFR-FRIENDS study revealed that deferred angiographically insignificant stenosis with low FFR showed a significantly higher event rate than those with high FFR. In addition, FFR was an independent predictor of future clinical events in those lesions with angiographically insignificant stenosis.33) In another substudy, patients with multi-vessel moderate CAD (FFR, 0.81–0.87) showed a comparable risk of clinical events with patients with functionally significant CAD.34)
These abovementioned study results suggest that pressure-derived physiologic indices reflect the risk continuum of patients with CAD, and its scope has now been expanded beyond a per-vessel decision for revascularization.
PHYSIOLOGIC EVALUATION FOR MICROVASCULAR DISEASE
Since the coronary artery system has 3 components with different functions (conductive epicardial coronary arteries, arterioles, and capillaries), myocardial ischemia can occur when any one of these systems fails. Thus, the presence of epicardial coronary artery stenosis is not the prerequisite for ischemic heart disease.35) In the FAME II study, 14.6% of the registry arm (FFR>0.80 and deferral of PCI) experienced persistent angina.36) Although the microvascular system cannot be visualized by invasive coronary angiography, its function and presence of microvascular disease can be evaluated by invasive physiologic indices. Index of microcirculatory resistance (IMR) is a specific index for microvascular status, and can be measured by a thermodilution technique. CFR represents the microvascular status when there is no significant epicardial disease and can be measured using a Doppler wire or a pressure/temperature-sensor guide wire (Figure 5).
Figure 5
Concept of coronary flow reserve and IMR. (A) Using thermodilution technique, Tmn, which is the surrogate marker of coronary flow, can be measured in both resting and hyperemic conditions. CFR is calculated by resting Tmn/hyperaemic Tmn. IMR is calculated by Pd×Tmn during hyperaemia. (B) The patient presented with typical chest pain on exertion and a positive exercise stress test. Coronary angiography showed no obstructive epicardial coronary artery disease and FFR was insignificant in both LAD and LCX. However, CFR was low and IMR was high in both LAD and LCX, suggesting the presence of overt microvascular disease.
CAD = coronary artery disease; CFR = coronary flow reserve; FFR = fractional flow reserve; IMR = index of microcirculatory resistance; LAD = left anterior descending artery; LCX = left circumflex artery; Tmn = mean transit time; TMT = treadmill test.

Several studies evaluated the association between macro- and microvascular disease using invasive physiologic indices. The international IMR registry evaluated 1,096 patients (1,452 vessels) who underwent FFR and IMR measurement, and found that there was no correlation between IMR and FFR values (r=0.01; p=0.62) and between IMR and angiographic % diameter stenosis (r=−0.03; p=0.25).37) Kobayashi et al.38) evaluated 93 patients who underwent comprehensive physiologic assessment in all 3 major coronary vessels. The majority of patients (59.1%) had no microvascular disease, 23.7% had 1-vessel microvascular disease, 14.0% had 2-vessel microvascular disease, and 3.2% had 3-vessel microvascular disease. The SYNTAX score, a surrogate marker of macrovascular disease burden, had no significant correlation with IMR.38) These results support the hypothesis that macro- and microvascular diseases are different disease processes with different predisposing factors39)40)41) and underscores the importance of comprehensive physiologic assessment to discriminate the cause of ischemic heart disease.
Previous studies also demonstrated the importance of comprehensive physiologic assessment in view of prognostic implication. Meuwissen et al.42) reported that among patients with FFR≥0.75, those with abnormal Doppler-derived CFR had a higher 1-year event rate compared to those with normal CFR. Similarly, van de Hoef et al.43) reported the long-term outcomes of 157 patients with intermediate stenosis and showed that patients with high FFR and low CFR had a higher 10-year event rate than the patients with high FFR and high CFR (relative risk, 2.8). In these studies, low CFR was used as a surrogate marker of microvascular disease in patients with high FFR.
Some patients can have discordant results between CFR and IMR, as CFR represents the flow ratio between hyperemic and resting conditions while IMR represents microvascular resistance in a hyperaemic condition. Therefore, combining CFR and IMR might provide a more precise stratification of patients with overt microvascular disease. In this regard, Lee et al.44) evaluated the prognosis of patients according to CFR and IMR levels. Among patients with high FFR, 61.3% had normal CFR and IMR, 18.3% had high CFR despite high IMR, 13.5% had low CFR despite low IMR, and 7.0% had low CFR and high IMR. Although there were no significant differences in clinical or angiographic characteristics, the 4 groups showed different risk of patient-oriented composite outcomes. Among the 4 groups, only those with low CFR and high IMR (overt microvascular disease) had a significantly higher risk of clinical events than the concordant normal group (HR, 5.62; 95% CI, 1.23–25.62). In addition, the presence of low CFR in conjunction with high IMR was the most powerful independent predictor for clinical events among patients with high FFR. These results suggest that invasive physiologic assessment for microvascular disease combined with CFR and IMR can help identify patients at high risk for future cardiovascular events among those with high FFR. However, further studies are needed to investigate the mechanism of clinical events in patients with microvascular disease and optimal treatment strategy for those patients.
CONCLUSION
Comprehensive understanding of the coronary circulation, coronary artery stenosis, ischemic heart disease, and the role of revascularization is needed for adequate assessment and treatment of patients with CAD. Recent progress in the field of invasive coronary physiology has expanded the role of pressure-derived invasive physiologic indices, from a binary decision tool for revascularization, to a comprehensive tool for risk assessment and selection of optical treatment strategy. Now is the time for us to become more physiologic and smarter than FFR or iFR, to fill the gap between evidence and practice for the benefit of our patients.
 XML Download
XML Download