

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Brachytherapy in combination with external beam radiotherapy (EBRT) is an important radiotherapeutic modality for treating cancers of the cervix, prostate, breast, head and neck, respiratory tract, and digestive organs [1]. In brachytherapy, radioisotope sources can be positioned adjacent to the tumor site. A rapid dose fall-off around the radioactive sources in brachytherapy makes it possible to increase tumor control while sparing the surrounding organs [1]. Based on its therapeutic advantages, brachytherapy has been regarded as a standard treatment for several types of cancer, especially for cervical cancer and other gynecological cancers. Therefore, a large number of radiation treatment facilities have performed brachytherapy for several decades. The latest Korean survey in 2006 showed that 65% of radiation oncology centers in Korea operate brachytherapy units [2].
However, the use of brachytherapy in Korea has been declining as the number of patients with cervical cancer has been decreasing. According to the Korea Central Cancer Registry, the age-standardized incidence rate of cervical cancer per 100,000 persons fell from 16.3 in 1999 to 10.6 in 2010, marking an average annual fall of 4.3% during the period [3]. Because cervical cancer is one of the most common indications for brachytherapy, the use of brachytherapy is speculated to be declining as the incidence of cervical cancer decreases. Nonetheless, there is insufficient information on the status of brachytherapy in Korea. In order to establish future brachytherapy policies in Korea, it is crucial to understand the current status of infrastructures and patterns of care for brachytherapy. The aim of the present study was to acquire information on brachytherapy resources in Korea through a national survey of radiation oncologists.
MATERIALS AND METHODS
Between October 2014 and January 2015, a questionnaire on the current status of brachytherapy was distributed to all 86 radiation oncology departments in Korea. The division of gynecologic cancer of the Korean Radiation Oncology Group (KROG) designed the questionnaire for distribution. The questionnaire was divided into the following three sections: general information including human resources, status of brachytherapy, and policy suggestions for brachytherapy.
Questions regarding personnel at each radiation oncology center were asked in the general information section. Infrastructure and the number of patients treated with brachytherapy at each center were examined in the brachytherapy status section. For radiation oncology centers without brachytherapy equipment, the questionnaire asked their policies in the management of patients requiring brachytherapy. In the future policy section, respondents were asked to comment on difficulties in operating brachytherapy centers and to state their plans for brachytherapy operations.
The survey was sent via email to the director of the Radiation Oncology Department in each hospital with a request to return the results to the researchers.
RESULTS
Of the 86 radiation oncology departments, 76 completed the questionnaire and 10 did not respond to the request. Therefore, the response rate of the current survey was 88.3%.
1. Human resources
Among the 76 participating centers, which consisted of 63 academic and 13 non-academic centers, there were 247 board-certified radiation oncologists. The average number of radiation oncologists per center was 2.3 (95% CI, 1.9 to 2.8). A total of 52 centers (72.3%) had two or fewer radiation oncologists. Additionally, 68 radiation oncology residents were in the course of training in 20 centers (26.3%). There were 123 radiation oncology physicists in 71 centers, while no physicists were present in five centers. The details of human resources in each center are presented in Table 1.
Table 1
Distribution of human resources among 76 radiation oncology centers in Korea

2. Status of brachytherapy
There were brachytherapy equipment installations in 32 radiation oncology centers. Among these 32 centers, 28 currently provide brachytherapy to patients while four had stopped performing brachytherapy at the time of survey. Consequently, brachytherapy is currently available in 36.8% (28 of 76) of the radiation oncology centers in Korea. The number of brachytherapy installations per million inhabitants is 0.55. In each brachytherapy center, there were one or two physicians specialized in brachytherapy. Each brachytherapy center had one brachytherapy treatment system. A regional distribution of the 28 brachytherapy centers is depicted in Fig. 1. All 28 centers perform high-dose rate (HDR) brachytherapy using iridium-192 (192Ir, 26 centers) or cobalt-60 (60Co, two centers). For centers using 192Ir, the intervals for radioisotope source replacement are between 3 and 10 months. Among the centers using 192Ir sources, 42.3% treated fewer than 40 patients over the last 12 months. In the two centers using 60Co sources, the number of patients per year was 16 and 120, respectively. In addition, 22 brachytherapy centers (78.5%) treated gynecological cancers only, while six centers (21.5%) used brachytherapy for other cancers in addition to gynecological cancers (Table 2). In treating gynecologic cancers, all 28 brachytherapy centers apply brachytherapy for cervical and endometrial cancers. For patients with cervical cancer, brachytherapy is used for definitive treatment (in 28 centers) and postoperative therapy (in 24 centers) in combination with external beam whole pelvic radiotherapy. For endometrial cancer, brachytherapy is administered as definitive treatment (in 18 centers) and postoperative treatment (in 28 centers). Various fractionation schedules are used in brachytherapy for cervical and endometrial cancers in the 28 centers (Supplementary Tables 1, 2). A total of 31 patients with non-gynecological cancer were treated in the six centers over the last 12 months, with the number at each hospital ranging between 1 and 20.
Fig. 1
Regional distribution of the 28 brachytherapy centers in Korea. The value in parentheses presents brachytherapy equipment per million inhabitants in each region.

Table 2
Status of brachytherapy among the 28 brachytherapy centers in Korea

There were 48 radiation oncology centers that do not perform brachytherapy. To manage patients requiring brachytherapy, 35 centers referred the patients to other hospitals for brachytherapy, while seven centers treated the patients either with EBRT as a substitute for brachytherapy or referred them to other brachytherapy centers. Asked if they had a brachytherapy center to where patients are often referred, 33 centers responded positively, while nine said they did not (Table 3).
Table 3
Management of patients who need brachytherapy in 48 radiation oncology centers not performing brachytherapy

3. Future policy for brachytherapy
To understand hardships in operating brachytherapy centers, respondents were asked to verify difficulties in introducing or maintaining brachytherapy equipment. In the 48 radiation oncology centers not performing brachytherapy, high expenses for source replacement was the most frequent reason for not installing brachytherapy equipment. The most frequently cited difficulties in the operation of the 28 brachytherapy facilities were cost related (Table 4).
Table 4
Opinions of radiation oncologists regarding operation of brachytherapy center

Asked to identify their future plans for introducing brachytherapy, 42 of the 48 radiation oncology centers that do not practice brachytherapy provided responses. A total of 26 centers (54.2%) said that they would not install brachytherapy equipment, whereas 16 centers (33.3%) considered introducing brachytherapy as long as the treatment would generate profit or if departmental revenues would cover expenses. Meanwhile, among the 28 brachytherapy centers, 27 stated their plans for brachytherapy. Of these, 21 centers (75.0%) said they will sustain the current brachytherapy system, four (14.4%) noted plans to upgrade the system, and two (7.2%) answered that they considered discontinuing brachytherapy due to cost burdens of radioisotope source replacement.
To formulate future policies for brachytherapy, all 76 respondents were asked to choose at least one suggestion among the following: (1) maintain the present brachytherapy policy; (2) raise the medical fee for brachytherapy; and (3) designate regional brachytherapy centers and request government subsidies. The frequencies of selection of each answer were 3, 42, and 42, respectively.
DISCUSSION
The present study is the first to investigate the current status of brachytherapy in Korea through a national survey of radiation oncologists. As of January 2015, only 32.5% of Korean radiation oncology centers could provide brachytherapy to patients. All centers had a HDR brachytherapy system, and about 43% of the brachytherapy centers treated fewer than 40 patients per year. Further, more than 70% of the centers applied brachytherapy only to the patients with gynecological cancers. For radiation oncology centers without brachytherapy equipment, the most common response for not having brachytherapy equipment was high expenses for replacement of the radionuclides source.
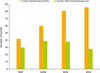
Notably, the number of brachytherapy centers and the proportion of Korean radiation oncology centers offering brachytherapy have decreased since 2006. According to reports by the Korean Society for Radiation Oncology, there were 39 brachytherapy centers among 60 radiation oncology centers in 2006 [2,4]. In the current survey, a total of 28 brachytherapy centers were identified among 76 radiation oncology centers, showing a 28.2% decrease since 2006 (Fig. 2). In addition, the number of brachytherapy units per million inhabitants fell from 0.79 to 0.55 between 2006 and 2014. We have also found that the brachytherapy centers are unevenly distributed across the regions of Korea. A total of 53.5% (15 of 28) brachytherapy centers are located in the capital Seoul and its surrounding metropolitan areas. Outside the metropolitan area, fewer than three brachytherapy centers were identified in each province, except in Gyeongnam province, which includes Busan, the second largest city in Korea. Moreover, no brachytherapy units are installed in Chungbuk province and the province of Jeju Island. Thus, regional patients who opt for brachytherapy will incur travel and accommodation expenses.
The proportion of radiation oncology centers offering brachytherapy is lower in comparison to other countries. According to studies, the number of brachytherapy centers is 29 in the United Kingdom, 39 in Spain [5], 30 in Canada [6], and 125 in Germany [7]. The proportions of brachytherapy centers in Canada, Europe, and Latin America have been listed as 90.9%, 60.3%, and 50.6%, respectively [6-9]. Because the year of data acquisition and the rate of response to the surveys were different among the studies, one cannot directly compare the availability of brachytherapy in Korea to other countries using this data. However, the availability of brachytherapy has become worse over the last two decades because of a rapid decrease in the number of brachytherapy centers and an uneven regional distribution of units.
The low proportion of brachytherapy centers raises the possibility of providing inadequate treatments for tumor, particularly for cancer in the intact uterine cervix. Patients with cancer in the intact uterine cervix should be treated with EBRT along with brachytherapy. In cases where a patient with cancer in the intact cervix receives EBRT in a radiotherapy center without brachytherapy equipment, the patient should be transferred to another center for brachytherapy. Because almost two thirds of radiation oncology centers in Korea do not have brachytherapy equipment, a large number of patients with cervical cancer should have such a referral. However, there are no well-organized referral systems in Korean radiation oncology centers. A total of 18.8% (9 of 48) radiation oncology centers without brachytherapy equipment did not have any pre-established network to brachytherapy centers. Even in the radiation oncology centers that have outside links to brachytherapy centers, radiation oncologists have no formal role beyond providing patients with information about hospitals with a brachytherapy center. Moreover, 14.6% (7 of 48) of the surveyed centers replied that they had cases treated with EBRT instead of brachytherapy. In treating cancer of the intact uterine cervix, brachytherapy is an essential treatment. Not providing brachytherapy is detrimental to the survival of patients with cervical cancer [10,11]. In addition, extending the overall duration of radiotherapy to more than 56 days has been reported to be significantly associated with an increased risk of pelvic failure in concurrent chemoradiotherapy for cervical cancer [12]. Therefore, it is crucial to build a well-organized referral system to expedite patient referral.
Of note, most of the surveyed radiation oncology centers applied brachytherapy only to patients with gynecological cancers. Even the centers that performed brachytherapy for patients with non-gynecological cancers treated fewer than 20 such patients in a year. Moreover, there were only 31 patients with non-gynecological cancers treated with brachytherapy in a year among all responding radiation oncology centers in the current study. Given that more than 40% of brachytherapy in other countries is applied to non-gynecological cancers, such as the prostate or breast cancer, it is worth broadening the application of brachytherapy in Korea [6,8].
In Korea, the medical reimbursement system is strictly controlled by the government. No private medical reimbursement system is allowed. Even though there is an annual negotiation between the government and organizations of health care providers, increases in charges are almost always set according to restrictions suggested by the government. The Korean Society of Radiation Oncology tried to raise teletherapy charges, rather than brachytherapy, owing to a dramatic rise in the provision of teletherapy and rapid decrease in prescriptions of brachytherapy. Consequently, insufficient reimbursement was the most frequently noted barrier to installing and sustaining brachytherapy centers. For intracavitary brachytherapy with 5 to 15 fractions, including simulation and planning, the Korean National Health Insurance reimburses 1,300,000 Korean won (KRW) or about 1,213 US $ (using the 2014 average exchange rate of 1,071 KRW to the US $) [13]. The 1,300,000 KRW includes expenses for source replacement as well as procedure costs. Because most brachytherapy is completed within 15 fractions, a radiotherapy center will be paid a total of 1,300,000 KRW for the entire course of brachytherapy per patient. In brachytherapy centers using 192Ir sources, the source should be changed four times per year, considering that the half-life of 192Ir is 74 days [14]. The purchase cost of 192Ir is about 13,000,000 KRW per replacement in Korea. Therefore, at least 40 new patients a year are necessary for cost-effective operation of the 192Ir brachytherapy centers. All but two Korean brachytherapy centers adopted 192Ir sources, and 42.3% of the centers treated fewer than 40 patients per year. Under the current circumstances, most Korean brachytherapy centers are expected to suffer a deficit for the operation of brachytherapy. Indeed, four radiation oncology centers ceased to operate brachytherapy due to the high expenses of source exchange compared to the reimbursement.
To overcome such a deficit caused by an imbalance of fee-to-source expenses, several centers exchanged the 192Ir source fewer than four times a year. Only one brachytherapy center changed 192Ir sources within 3 months, while half of the centers replaced the source every 6 months. A longer interval of 192Ir source replacement than 3 months causes low source strength, decreasing dose rate and increasing treatment times, creating a vicious cycle of inefficiency, leading to therapeutically inferior results. To provide high quality brachytherapy to patients, it is necessary to set adequate brachytherapy fees that can cover the source replacement expense. In the Medicare reimbursement of the Unites States, the cost of radionuclide sources is charged in addition to fees for brachytherapy simulation, planning, image guidance, procedures, and medical physics consultation [15]. Korean radiation oncologists expressed in the current survey that the national reimbursement system needs to be similarly adjusted to cover the expenses of radionuclide sources.
At present, only a third of Korean radiation oncology centers can provide brachytherapy to patients. Given the finite brachytherapy resources, it is important to use them efficiently while maintaining high-quality brachytherapy. To provide patients with properly qualified brachytherapy, the respondents to the current survey suggested constructing referring networks of brachytherapy with designated referral centers by region. According to experts, centers treating low number of patients should refer the patients to larger centers for brachytherapy as continued practice of brachytherapy is needed to maintain skills [16,17]. Given that about 7% of brachytherapy centers in Korea treated fewer than 10 patients per year, the referral networks are also necessary for brachytherapy centers with a low volume of patients. With well-organized referral networks, patients are expected to have timely brachytherapy without treatment delay. To set up such a system, it is necessary to estimate how many patients are referred to another hospital for brachytherapy. To facilitate patient’s referral and to maintain high quality of treatment, some financial support might be helpful for brachytherapy referral centers. The KROG and Ministry of Health and Welfare should cooperate in constructing the referring networks for brachytherapy in the future.
In conclusion, the present study shed light on the current status of brachytherapy in Korea, focusing on the resources and facilities available. The quantity of brachytherapy resources is decreasing and these resources are distributed unequally across Korea. Financial difficulties were the major barriers to the practice of brachytherapy in Korean radiation oncology centers. Given the limited resources available, a network linking base brachytherapy centers was proposed, to facilitate referring patients in timely fashion.
 XML Download
XML Download