

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In gynecology endosalpingiosis is a benign condition in which fallopian tube-like epithelium is found outside of the fallopian tube. Endosalpingiosis is associated with the formation of psammoma bodies, which may lead to the misdiagnosis of malignancy such as serous carcinoma.1
The significance of endosalpingiosis is not settled; medical experts differ on whether it causes pelvic pain, or is an incidental (asymptomatic) finding discovered in the course of investigating pelvic pain, menstrual irregularities or infertility.
Endosalpingiosis is diagnosed by a pathologist on excision and biopsy. Endosalpingiosis is occasionally found in lymph nodes, and may be misinterpreted as an adenocarcinoma metastasis.
In one study, they found that 34.5% of endosalpingiosis cases had concurrent endometriosis; 40% of the endosalpingiosis group were postmenopausal. Endometriosis was significantly associated with infertility and chronic pelvic pain. In contrast, there was no significant link between endosalpingiosis and infertility nor chronic pelvic pain. Gynecologic malignancy occurred significantly more in premenopausal women with endosalpingiosis than in those without. Endosalpingiosis appears to affect postmenopausal women at a rate much higher than previously reported.2
Case Report
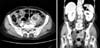
A 75-year-old woman, gravida 2, postmenopausal women, presented with vaginal bleeding which occurred a week ago. She had hyperlipidemia and took medical therapy. Under the impression of pelvic mass, cancer antigen 125 (CA-125), CA 19-9, complete blood cell count, serum chemistry, contrast enhanced - abdomen - computer tomography were done. CA 19-9 is 9.8 U/mL, CA-125 is 13.5 U/mL and glucose is 118 mg/dL. In contrast enhanced chest computer tomography, image showed multiseptated cystic mass in left adnexa which adhesion with left psoas muscle, adjacent small and large bowel loops and there is possibility of underlying chronic inflammatory process with abscess (Fig. 1). To rule out mucinous cyst adenoma, we executed exploratory laparotomy. Pathologic result shows endosalpingiosis near ovary. Vaginal bleeding is caused by the atrophic vaginitis considering that the patient's age is 75 years old.
Discussion
Endosalpingiosis is a non-neoplastic process and is generally considered to be derived from the secondary Müllerian system, which consists of structures covering the peritoneal mesothelium, the adjacent mesenchyme in the small pelvis and the lower part of the female abdominal cavity.3 Proliferation of these structures can result in the creation of three different types of lesions: endometriosis, which occurs most frequently, and the less common endosalpingiosis and endocervicosis.4
The symptom of endosalpingiosis is not settled; medical experts differ on whether it causes pelvic pain,5 or is an incidental (asymptomatic) finding discovered in the course of investigating pelvic pain, menstrual irregularities or infertility.6
The causes of the endosalpingiosis are unknown. In this case the endosalpingiosis was found incidentally. However, it is almost always an incidental finding, either at the time of operation or, more commonly, on microscopic examination.7 It is most commonly encountered on the pelvic peritoneum covering the uterus, Fallopian tubes, ovaries and culde-sac. Less frequent sites include the pelvic parietal peritoneum, omentum, bladder and bowel serosa, paraaortic area and skin.8 Only a few examples of tumor-like cystic endosalpingiosis localized to the female pelvis have been described, and most of these cases are reported to be derived from the serosal surface of the uterus and the ovary 6-10 or from the paraovarianregion.8
For diagnosis of endosalpingiosis, pathology on excision (e.g. biopsy), is needed. It is characterized by cysts with tubal-type epithelium (e.g. ciliated epithelium) surrounded by a fibrous stroma. Unlike endometriosis, it is not associated with hemorrhage. A tubal-type epithelial surrounded by endometrial-type stroma is a variant of endometriosis, not endosalpingiosis. Endosalpingiosis is occasionally found in lymph nodes, and may be misinterpreted as an adenocarcinoma metastasis.9 The pathological differential diagnosis of endosalpingiosis is discussed in detail in previously reported cases.7,10,11,12,13,14 However, the clinical differential diagnosis of an intramural mass, whether it causes any symptoms or not, is more important for clinicians when discussing further surgery with the patient. Therefore the symptoms and the imaging findings of this rare entity are very important. As endosalpingiosis, generally, is not considered a pathology, no treatment is necessary.
Endosalpingiosis appears to affect an older age group, with 40% of endosalpingiosis cases occurring in postmenopausal women.2 Premenopausal women with endosalpingiosis were more likely to have a gynecologic malignancy.2 Endosalpingiosis appears to affect postmenopausal women at a much higher rate than previously thought, and in consequence the average age of women presenting with endosalpingiosis was higher than expected.2 In this case, 75-year-old woman, gravida 2, postmenopausal women, presented with vaginal bleeding was reported. The patient showed untypical symptom and clinical manifestation. Her chief complain was vaginal bleeding. The most common symptom of endosalpingiosis is chronic pelvic pain. However, it must be kept in mind that vaginal bleeding can be caused by endosalpingiosis, especially in the postmenopausal elderly women. Possibility of endosalpingiosis must be considered in the differential diagnostic spectrum of vaginal bleeding, thus avoiding the problem of misdiagnosis of endosalpingiosis.
 XML Download
XML Download